
Abstract
Purpose
Defunctioning loop ileostomy in low anterior resection (LAR) is routinely used to reduce consequences of anastomotic leakage. The purpose of this study was to analyze which examination technique is optimal for evaluating the integrity of the anastomosis prior to loop ileostomy reversal.
Methods
Retrospective analysis of 95 patients who had been subjected to LAR at Helsingborg Hospital and Skåne University Hospital, Sweden, was undertaken between January 2007 and June 2009. The examination techniques of the rectal anastomosis prior to reversal and the clinical outcome after reversal were studied.
Results
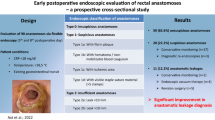
Radiologic anastomosis control using water soluble contrast enema, digital rectal examination (DRE), and rectoscopy were performed in 53 % (50/95), 98 % (93/95), and 69 % (66/95), respectively. In two patients, no control of the anastomosis was performed before reversal. Fifty-two percent (49/95) of the patients were examined using all techniques. Six patients demonstrated leakage detected before reversal of which two were only radiological leakages. These two patients underwent loop ileostomy reversal after delay without complications. They were the only ones where the three examination techniques did not prove coherence. Four patients had symptomatic leakage; these were detected with rectoscopy and DRE and verified with enema. Three patients developed anastomotic leakage after loop ileostomy reversal despite normal preoperative examinations. Two of these patients had rectovaginal fistulas (AVFs).
Conclusions
This retrospective study indicates that contrast enema does not provide additional information if rectoscopy and DRE are normal. Despite negative examinations, three of nine leakages were diagnosed after loop ileostomy reversal. Especially, AVFs seem difficult to diagnose.

Similar content being viewed by others


References
Heald R, Husband E, Ryall R (1982) The mesorectum in rectal cancer surgery—the clue to pelvic recurrence? Br J Surg 10:613–616
Wibe A, Eriksen M, Syse A, Myrvold H, Soereide O, Norwegian Rectal Cancer Group (2003) Total mesorectal excision for rectal cancer- what can be achieved by a national audit? Colorectal Dis 5:471–477
Rullier E, Laurent C, Garrelon J, Michel P, Saric J, Parneix M (1998) Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 85:355–358
Matthiessen P, Hallböök O, Andersson M, Rutegård J, Sjödahl R (2004) Risk factors for anastomotic leakage after anterior resection of the rectum. Colorectal Dis 6:462–469
Bruce J, Krukowski ZH, Al-Khairy G, Russell E, Park KG (2001) Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. Br J Surg 9:1157–1168
Matthiessen P, Hansson L, Sjödahl R, Rutegård J (2010) Anastomotic-vaginal fistula (AVF) after anterior resection of the rectum for cancer—occurrence and risk factors. Colorectal Dis 12:351–357. doi:10.1111/j.1463-1318.2009.01798.x
Matthiessen P, Hallböök O, Rutegård J, Simert G, Sjödahl R (2007) Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: a randomized multicenter trial. Ann Surg 246:207–214
Veenhof A, van der Peet D, Meijerink W, Cuesta M (2008) Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: a randomized multicenter trial. Ann Surg 4:718–719. doi:10.1097/SLA.0b013e31816a7493
Tan W, Tang C, Shi L, Eu K (2009) Meta-analysis of defunctioning stomas in low anterior resection for rectal cancer. Br J Surg 4:462–467. doi:10.1002/bjs.6594
Khair G, Alhamarneh O, Avery J, Cast J, Gunn J, Monson J, Hartley J (2007) Routine use of gastrografin enema prior to the reversal of a loop ileostomy. Dig Surg 24:338–341. doi:10.1159/000105525
Kalady M, Mantyh C, Petrofski J, Ludwig K (2008) Routine contrast imaging of low pelvic anastomosis prior to closure of defunctioning ileostomy: is it necessary? J Gastrointest Surg 7:1227–1231. doi:10.1007/s11605-008-0510-2
Tang C, Seow-Choen F (2005) Digital rectal examination compares favourably with conventional water-soluble contrast enema in the assessment of anastomotic healing after low rectal excision: a cohort study. Int J Colorectal Dis 3:262–266
Karsten B, King J, Kumar R (2009) Role of water-soluble enema before takedown of diverting ileostomy for low pelvic anastomosis. Am Surg 75:941–944
Hong S, Kim D, Yeop Oh S, Wook Sug K (2012) Routine barium enema prior to closure of defunctioning ileostomy is not necessary. J Korean Surg Soc 83:88–91. doi:10.4174/jkss.2012.83.2.88
Alves A, Panis Y, Lelong B, Doussett B, Benoist S, Vicaut E (2008) Randomized clinical trial of early versus delayed temporary stoma closure after proctectomy. Br J Surg 6:693–698. doi:10.1002/bjs.6212
Jörgren F, Johansson R, Damber L, Lindmark G (2011) Anastomotic leakage after surgery for rectal cancer: a risk factor for local recurrence, distant metastasis and reduced cancer-specific survival. Colorectal Dis 13:272–283. doi:10.1111/j.1463-1318.2009.02136.x
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Larsson, A., Lindmark, G., Syk, I. et al. Water soluble contrast enema examination of the integrity of the rectal anastomosis prior to loop ileostomy reversal may be superfluous. Int J Colorectal Dis 30, 381–384 (2015). https://doi.org/10.1007/s00384-014-2113-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-014-2113-6