
Abstract
Background
During the last decades transaxillary breast augmentation (TBA) has gained worldwide acceptance. Breast augmentation via transaxillary access endoscopically assisted in the subglandular, subfascial, and submuscular planes has been previously described. Although TBA is a well-studied procedure, few reports exist concerning the subfascial plane of implant insertion and none exist comparing the three different planes of insertion by TBA.
Methods
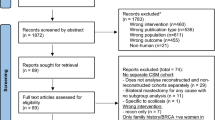
A perspective study to evaluate the outcomes, complications, and patient satisfaction of TBA using the three different planes of implant insertion was performed during 2004-2005. Fifty-three patients fulfilled the inclusion criteria. They were randomly divided into three groups corresponding to the three planes of silicone insertion. All patients had a silicone texturized implant that ranged from 190 to 300 cc. Overall satisfaction with the breast appearance after TBA was rated on a scale of 1-5, where 1 is poor, 2 is fair, 3 is good, 4 is very good, and 5 is excellent. The evaluation was made at the follow-up times of 6 months and 3 years.
Results
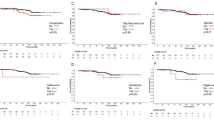
There were 18 patients enrolled for the subcutaneous TBA (Group A), 18 for the subfascial TBA (Group B), and 17 for the submuscular TBA (Group C). Axillary incision-related complications occurred in 9% of the patients and included formation of a hypertrophic scar and small-wound dehiscence. There was no hematoma formation and no case of infection. There was one patient from Group A who developed seroma and was treated conservatively. Twenty-seven months postoperatively the same patient developed Baker III capsule contracture, which required silicone implant replacement in the subfascial plane. One case of stretch marks in a young nulliparous woman from Group B did not need treatment. One patient from Group A underwent implant exchange because of implant size dissatisfaction. Three patients in Group C had mild distortion of the implant during pectoral contracture. A meta-analysis of patient satisfaction 6 months and 3 years after TBA is presented.
Conclusion
Transaxillary breast augmentation provides consistent, satisfactory results with ease of dissection, when properly indicated. Although the subfascial augmentation mammaplasty has all the advantages of the subpectoral and subglandular augmentation mammaplasties and eliminates the disadvantages of increased postoperative discomfort, implant visibility, and distortion, patients of all three groups had similar rates of satisfaction. Further follow-up is needed in order to compare the long-term effects of the three different planes of insertion.








Similar content being viewed by others

References
Giordano PA, Rouif M, Laurent B, Mateu J (2007) Endoscopic transaxillary breast augmentation: clinical evaluation of a series of 306 patients over a 9-year period. Aesthet Surg J 27(1):47–54
Pacella SJ, Codner MA (2009) The transaxillary approach to breast augmentation. Clin Plast Surg 36(1):49–61, vi
Ersek RA, Navarro JA (1991) Transaxillary subpectoral placement of textured breast prostheses. Ann Plast Surg 27(1):93–96
Graf RM, Bernardes A, Auersvald A, Damasio RC (2000) Subfascial endoscopic transaxillary augmentation mammaplasty. Aesthetic Plast Surg 24(3):216–220
Benito-Ruiz J (2003) Transaxillary subfascial breast augmentation. Aesthet Surg J 23(6):480–483
Howard PS, Oslin BD, Moore JR (1996) Endoscopic transaxillary submuscular augmentation mammaplasty with textured saline breast implants. Ann Plast Surg 37(1):12–17
Siclovan HR, Jomah JA (2008) Advantages and outcomes in subfascial breast augmentation: a two-year review of experience. Aesthetic Plast Surg 32(3):426–431
Prado A, Andrades P, Leniz P (2007) Implications of transaxillary breast augmentation: lifetime probability of breast cancer development and sentinel node mapping interference. Aesthetic Plast Surg 31(4):317–319
Munhoz AM, Aldrighi C, Buschpiegel C, Ono C, Montag E, Fells K, Arruda E, Sturtz G, Kovac P, Filassi JR, Gemperli R, Ferreira MC (2005) The feasibility of sentinel lymph node detection in patients with previous transaxillary implant breast augmentation: preliminary results. Aesthetic Plast Surg 29(3):163–168
Sado HN, Graf RM, Canan LW, Romano GG, Timi JR, Matias JE, Yamada AS, Woellner LC, Cruz GA (2008) Sentinel lymph node detection and evidence of axillary lymphatic integrity after transaxillary breast augmentation: a prospective study using lymphoscintography. Aesthetic Plast Surg 32(6):879–888
Mottura AA, Del Castillo R (2007) Transaxillary breast augmentation: two breast cancer patients with successful sentinel lymph node diagnosis. Aesthetic Plast Surg 31(5):544–549 discussion 550–552
Hwang K, Kim DJ (2005) Anatomy of pectoral fascia in relation to subfascial mammary augmentation. Ann Plast Surg 55(6):576–579
Jinde L, Jianliang S, Xiaoping C, Xiaoyan T, Jiaqing L, Qun M, Bo L (2006) Anatomy and clinical significance of pectoral fascia. Plast Reconstr Surg 118(7):1557–1560
Serra-Renom J, Garrido MF, Yoon T (2005) Augmentation mammaplasty with anatomic soft, cohesive silicone implant using the transaxillary approach at a subfascial level with endoscopic assistance. Plast Reconstr Surg 116(2):640–645
Graf RM, Bernardes A, Rippel R, Araujo LR, Damasio RC, Auersvald A (2003) Subfascial breast implant: a new procedure. Plast Reconstr Surg 111(2):904–908
Baxter RA (2005) Subfascial breast augmentation: theme and variations. Aesthet Surg J 25(5):447–453
Stevens WG, Pacella SJ, Gear AJ, Freeman ME, McWhorter C, Tenenbaum MJ, Stoker DA (2008) Clinical experience with a fourth-generation textured silicone gel breast implant: a review of 1012 Mentor Memory Gel breast implants. Aesthet Surg J 28(6):642–647
Spear SL, Schwartz J, Dayan JH, Clemens MW (2009) Outcome assessment of breast distortion following submuscular breast augmentation. Aesthetic Plast Surg 33(1):44–48
Hendricks H (2007) Complete submuscular breast augmentation: 650 cases managed using an alternative surgical technique. Aesthetic Plast Surg 31(2):147–153
Strasser EJ (2006) Results of subglandular versus subpectoral augmentation over time: One surgeon’s observations. Aesthet Surg J 26(1):45–50
Zhibo X, Miaobo Z (2009) Effect of sustained-release lidocaine on reduction of pain after subpectoral breast augmentation. Aesthet Surg J 29(1):32–34
Momeni A, Padron NT, Bannasch H, Borges J, Björn Stark G (2006) Endoscopic transaxillary subpectoral augmentation mammaplasty: a safe and predictable procedure. J Plast Reconstr Aesthet Surg 59(10):1076–1081
Keramidas E, Rodopoulou S (2008) Striae distensae after subfascial breast augmentation. Aesthetic Plast Surg 32(2):377–380
Cash TF, Duel LA, Perkins LL (2002) Women’s psychosocial outcomes of breast augmentation with silicone gel-filled implants: a 2-year prospective study. Plast Reconstr Surg 109(6):2112–2121 discussion 2122–2123
Pereira LH, Sterodimas A (2007) Definite size of the augmented breast could be up to a breast cup smaller than the early postoperative size. Aesthetic Plast Surg 31(6):759
Murphy DK, Beckstrand M, Sarwer DB (2009) A prospective, multi-center study of psychosocial outcomes after augmentation with natrelle silicone-filled breast implants. Ann Plast Surg 62(2):118–121
Solvi AS, Foss K, von Soest T, Roald HE, Skolleborg KC, Holte A (2009) Motivational factors and psychological processes in cosmetic breast augmentation surgery. J Plast Reconstr Aesthet Surg. 2009 (Epub ahead of print)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pereira, L.H., Sterodimas, A. Transaxillary Breast Augmentation: A Prospective Comparison of Subglandular, Subfascial, and Submuscular Implant Insertion. Aesth Plast Surg 33, 752–759 (2009). https://doi.org/10.1007/s00266-009-9389-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-009-9389-x