
Abstract
Purpose
Impingement is a major source for decreased range of motion (ROM) and dislocation in total hip arthroplasty (THA). In the current study we analyzed the impact of soft tissue impingement on ROM compared to bony and/or prosthetic impingement.
Methods
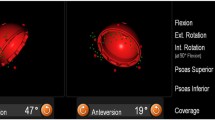
In the course of a prospective clinical trial 54 patients underwent cementless total hip arthroplasty in the lateral decubitus position using imageless navigation. The navigation device enabled intra-operative ROM measurements indicating soft tissue impingement. Post-operatively, all patients received postoperative 3D-CT. Absolute ROM without bony and/or prosthetic impingement was calculated with the help of a collision-detection-algorithm.
Results
Due to soft tissue impingement we found a reduced ROM of over 20° (p < 0.001) compared to bony and/or prosthetic impingement regarding flexion, extension, abduction and adduction and of over 10° regarding external rotation (p < 0.001). In contrast, soft tissue impingement showed less impact on internal rotation in 90° of flexion (p = 0.76). Multivariate analysis showed an association between BMI and flexion, whereas all other ROM directions were independent of BMI.
Conclusions
Soft tissue has a major impact on impingement-free ROM after THA. For the majority of movements, soft tissue restrictions are more important than bony and prosthetic impingement. Future models of patient individual joint replacement including pre-operative (CT) planning and intra-operative navigation should include algorithms additionally accounting for soft tissue impingement.




Similar content being viewed by others
References
Digioia AM 3rd, Jaramaz B, Plakseychuk AY, Moody JE Jr, Nikou C, Labarca RS, Levison TJ, Picard F (2002) Comparison of a mechanical acetabular alignment guide with computer placement of the socket. J Arthroplasty 17:359–364
Dorr LD, Malik A, Wan Z, Long WT, Harris M (2007) Precision and bias of imageless computer navigation and surgeon estimates for acetabular component position. Clin Orthop Relat Res 465:92–99
Craiovan B, Grifka J, Keshmiri A, Moser B, Wörner M, Renkawitz T (2015) Bone defect adjusted strategy in revision arthroplasty of the hip: wich implant in wich situation? Innovations and approved methods. Orthopade 44(5):366–374
Trousdale RT, Cabanela ME, Berry DJ (1995) Anterior iliopsoas impingement after total hip arthroplasty. J Arthroplasty 10:546–549
Yoshimine F (2006) The safe-zones for combined cup and neck anteversions that fulfill the essential range of motion and their optimum combination in total hip replacements. J Biomech 39:1315–1323
D’Lima DD, Urquhart AG, Buehler KO et al (2000) The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. J Bone Joint Surg Am 82:315
Miki H, Yamanashi W, Nishii T et al (2007) Anatomic hip range of motion after implantation during total hip arthroplasty as measured by a navigation system. J Arthroplasty 7:946–952
Seki M, Yuasa N, Ohkuni K (1998) Analysis of optimal range of socket orientations in total hip arthroplasty with use of computer-aided design simulation. J Orthop Res 16:513
Shoji T, Yamasaki T, Izumi S, Hachisuka S, Ochi M (2016) The influence of stem offset and neck shaft angles on the range of motion in total hip arthroplasty. Int Orthop 40(2):245–253
Hirata M, Nakashima Y, Hara D, Kanazawa M, Kohno Y, Yoshimoto K, Iwamoto Y (2015) Optimal anterior femoral offset for functional range of motion in total hip arthroplasty--a computer simulation study. Int Orthop 39(4):645–651
Renkawitz T, Weber M, Springorum R, Sendtner E, Woerner M, Ulm K, Weber T, Grifka J (2015) Impingement-free range of movement, acetabular component cover and early clinical results comparing 'femur-first' navigation and 'conventional' minimally invasive total hip arthroplasty: a randomised controlled trial. Bone Joint J 97(7):890–898
Widmer KH, Zurfluh B (2004) Compliant positioning of total hip components for optimal range of motion. J Orthop Res 22:815
Shoji T, Yasunaga Y, Yamasaki T, Mori R, Hamanishi M, Ochi M (2013) Bony impingement depends on the bone morphology of the hip after total hip arthroplasty. Int Orthop 37(10):1897–1903
Michel M, Witschger P (2007) MicroHip: a minimally invasive procedure for total hip replacement surgery using a modified Smith-Peterson approach. Ortop Traumatol Rehabil 9:46–51
Renkawitz T, Haimerl M, Dohmen L, Woerner M, Springorum HR, Sendtner E, Heers G, Weber M, Grifka J (2012) Development and evaluation of an image-free computer-assisted impingement detection technique for total hip arthroplasty. Proc Inst Mech Eng H 226(12):911–918
Renkawitz T, Haimerl M, Dohmen L, Gneiting S, Wegner M, Ehret N, Buchele C, Schubert M, Lechler P, Woerner M, Sendtner E, Schuster T, Ulm K, Springorum R, Grifka J (2011) Minimally invasive computer-navigated total hip arthroplasty, following the concept of femur first and combined anteversion: design of a blinded randomized controlled trial. BMC Musculoskelet Disord 12:192
Sendtner E, Tibor S, Winkler R et al (2010) Stem torsion in total hip replacement. Acta Orthop 81:579–582
Turley GA, Ahmed SM, Williams MA, Griffin DR (2011) Establishing a range of motion boundary for total hip arthroplasty. Proc Inst Mech Eng H 225:769–782
Wu G, Siegler S, Allard P et al (2002) ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—part I: ankle, hip, and spine. International Society of Biomechanics. J Biomech 35:543–548
Brooks PJ (2013) Dislocation following total hip replacement: causes and cures. Bone Joint J 95-B:67–69
Preininger B, Haschke F, Perka C (2014) Diagnostics and therapy of luxation after total hip arthroplasty. Orthopade 43(1):54–63
Hayashi S, Nishiyama T, Fujishiro T, Hashimoto S, Kanzaki N, Nishida K, Kurosaka M (2012) Obese patients may have more soft tissue impingement following primary total hip arthroplasty. Int Orthop 36(12):2419–2423
Elkins JM, Daniel M, Pedersen DR, Singh B, Yack HJ, Callaghan JJ, Brown TD (2013) Morbid obesity may increase dislocation in total hip patients: a biomechanical analysis. Clin Orthop Relat Res 471(3):971–980
Malik A, Maheshwari A, Dorr LD (2007) Impingement with total hip replacement. J Bone Joint Surg Am 89-A:1832–1842
McCollum DE, Gray WJ (1990) Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop Relat Res 261:159–170
Parratte S, Pagnano MW, Coleman-Wood K, Kaufman KR, Berry DJ (2009) The 2008 Frank Stinchfield award: variation in postoperative pelvic tilt may confound the accuracy of hip navigation systems. Clin Orthop Relat Res 467:43–49
Babisch JW, Layher F, Amiot LP (2008) The rationale for tilt-adjusted acetabular cup navigation. J Bone Joint Surg Am 90-A:357–365
Acknowledgments
The help of Ms. S. Kling, Ms. C. Jendrewski, Ms. M. Riedl, Mr. M. Schubert, Mr. A. Hapfelmeier, Mr. B. Messmer, Mr. L. Dohmen, and Dr. M. Haimerl in this project is appreciated.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval and informed consent
All procedures performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of interest
No author’s financial or any other conflicts of interest are related directly or indirectly to the subject of this article. Funding for this clinical trial was provided by the German Federal Ministry of Education and Research (BMBF; grant number 01EZ0915). No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Rights and permissions
About this article

Cite this article
Woerner, M., Weber, M., Sendtner, E. et al. Soft tissue restricts impingement-free mobility in total hip arthroplasty. International Orthopaedics (SICOT) 41, 277–282 (2017). https://doi.org/10.1007/s00264-016-3216-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-016-3216-1