
Abstract
Purpose
The purpose of this study is to evaluate whether fluorodeoxyglucose (FDG) uptake of the large arteries can predict coronary artery calcium (CAC) progression in asymptomatic individuals.
Methods
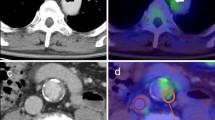
Ninety-six asymptomatic individuals who underwent FDG positron emission tomography (PET) and CAC scoring on the same day for health screening and follow-up CAC scoring ≥1 year after baseline studies (mean 4.3 years) were included. Vascular FDG uptake was measured and corrected for blood pool activity to obtain peak and average target-to-blood pool ratios (TBRpeak and TBRavg, respectively) for the carotid arteries, and ascending and abdominal aorta. CAC scores at baseline and follow-up of each individual were measured and absolute CAC change (ΔCAC), annual CAC change (ΔCAC/year), and annual CAC change rate (ΔCAC%/year) were calculated. CAC progression was defined as ΔCAC >0 for individuals with negative baseline CAC; ΔCAC/year ≥10 for those with baseline CAC of 0<x<100; ΔCAC%/year ≥10 % for those with baseline CAC ≥100. Vascular FDG uptake and other clinical risk factors were compared between CAC-progressors and non-CAC-progressors. Multivariate analysis was performed to evaluate whether vascular FDG uptake can independently predict CAC progression.
Results
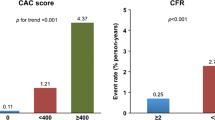
Thirty-one subjects showed CAC progression. CAC-progressors showed significantly higher TBRpeak and TBRavg as compared to non-CAC-progressors for all three arteries. TBRpeak of the abdominal aorta was significantly associated with CAC progression in multivariate analysis, with age and baseline CAC. A higher TBRpeak of the abdominal aorta (≥2.11) was associated with CAC progression among subjects with negative baseline CAC only. In subjects with positive baseline CAC, only the amount of baseline CAC was significantly associated with CAC progression. However, the positive predictive value of the TBRpeak of the abdominal aorta was <40 % when age was <58 or baseline CAC was negative.
Conclusions
Higher FDG uptake of the large arteries is associated with an increased risk of CAC progression in asymptomatic subjects with negative baseline CAC. But its clinical application needs further validation.





Similar content being viewed by others

References
Morin RL, Gerber TC, McCollough CH. Radiation dose in computed tomography of the heart. Circulation. 2003;107:917–22.
Budoff MJ, Hokanson JE, Nasir K, Shaw LJ, Kinney GL, Chow D, et al. Progression of coronary artery calcium predicts all-cause mortality. J Am Coll Cardiol Img. 2010;3:1229–36.
Wong ND, Nelson JC, Granston T, Bertoni AG, Blumenthal RS, Carr JJ, et al. Metabolic syndrome, diabetes, and incidence and progression of coronary calcium. J Am Coll Cardiol Img. 2012;5:358–66.
Okwuosa TM, Greenland P, Burke GL, Eng J, Cushman M, Michos ED, et al. Prediction of coronary artery calcium progression in individuals with low Framingham risk score: the multi-ethnic study of atherosclerosis. J Am Coll Cardiol Img. 2012;5:144–53.
Gassett AJ, Sheppard L, McClelland RL, Olives C, Kronmal R, Blaha MJ, et al. Risk factors for long-term coronary artery calcium progression in the multi-ethnic study of atherosclerosis. J Am Heart Assoc. 2015. doi:10.1161/JAHA.114.001726.
Cassidy-Bushrow AE, Bielak LF, Sheedy PF, Turner ST, Kullo IJ, Lin X, et al. Coronary artery calcification progression is heritable. Circulation. 2007;116:25–31.
Lusis AJ. Atherosclerosis. Nature. 2000;407:233–41.
Budoff MJ. Progression of coronary calcium not as predictable as 1-2-3. Eur Heart J. 2014;35:2934–5.
Tarkin JM, Joshi FR, Rudd JH. PET imaging of inflammation in atherosclerosis. Nat Rev Cardiol. 2014;11:443–57.
Abdelbaky A, Corsini E, Figueroa AL, Fontanez S, Subramanian S, Ferencik M, et al. Focal arterial inflammation precedes subsequent calcification in the same location: a longitudinal FDG-PET/CT study. Circ Cardiovasc Imaging. 2013;6:747–54.
Goyen M, Herborn CU, Kroger K, Lauenstein TC, Debatin JF, Ruehm SG. Detection of atherosclerosis: systemic imaging for systemic disease with whole-body three-dimensional MR angiography - initial experience. Radiology. 2003;227:277–82.
Rudd JHF, Myers KS, Bansilal S, Machac J, Woodward M, Fuster V, et al. Relationships among regional arterial inflammation, calcification, risk factors, and biomarkers: a prospective fluorodeoxyglucose positron-emission tomography/computed tomography imaging study. Circ Cardiovasc Imaging. 2009;2:107–15.
Tahara N, Tahara A, Narula J, Imaizumi T. Statin therapy resolves coronary artery inflammation. J Am Coll Cardiol Img. 2013;6:1119–20.
Tawakol A, Fayad ZA, Mogg R, Alon A, Klimas MT, Dansky H, et al. Intensification of statin therapy results in a rapid reduction in atherosclerotic inflammation: results of a multicenter fluorodeoxyglucose-positron emission tomography/computed tomography feasibility study. J Am Coll Cardiol. 2013;62:909–17.
Zeb I, Li D, Nasir K, Malpeso J, Batool A, Flores F, et al. Effect of statin treatment on coronary plaque progression - a serial coronary CT angiography study. Atherosclerosis. 2013;231:198–204.
Oh JR, Seo JH, Chong A, Min JJ, Song HC, Kim YC, et al. Whole-body metabolic tumour volume of F-18-FDG PET/CT improves the prediction of prognosis in small cell lung cancer. Eur J Nucl Med Mol Imaging. 2012;39:925–35.
Noh TS, Yoo J, Kim SW, Lee EJ, Choi JY, Kim BT, et al. Effects of coverage extent and slice skipping on mean and maximum arterial 18F-FDG uptake ratios in patients with carotid plaque. Ann Nucl Med. 2012;26:715–22.
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte Jr M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15:827–32.
Marzola MC, Saboury B, Chondrogiannis S, Rampin L, Grassetto G, Ferretti A, et al. Role of FDG PET/CT in investigating the mechanisms underlying atherosclerotic plaque formation and evolution. Rev Esp Med Nucl Imagen Mol. 2013;32:246–52.
Jenny NS, Brown ER, Detrano R, Folsom AR, Saad MF, Shea S, et al. Associations of inflammatory markers with coronary artery calcification: results from the multi-ethnic study of atherosclerosis. Atherosclerosis. 2010;209:226–9.
Alman AC, Kinney GL, Tracy RP, Maahs DM, Hokanson JE, Rewers MJ, et al. Prospective association between inflammatory markers and progression of coronary artery calcification in adults with and without type 1 diabetes. Diabetes Care. 2013;36:1967–73.
Tawakol A, Migrino RQ, Bashian GG, Bedri S, Vermylen D, Cury RC, et al. In vivo 18F-fluorodeoxyglucose positron emission tomography imaging provides a noninvasive measure of carotid plaque inflammation in patients. J Am Coll Cardiol. 2006;48:1818–24.
Tawakol A, Migrino RQ, Hoffmann U, Abbara S, Houser S, Gewirtz H, et al. Noninvasive in vivo measurement of vascular inflammation with F-18 fluorodeoxyglucose positron emission tomography. J Nucl Cardiol. 2005;12:294–301.
Meller J, Sahlmann CO, Scheel AK. 18F-FDG PET and PET/CT in fever of unknown origin. J Nucl Med. 2007;48:35–45.
Bleeker-Rovers CP, Vos FJ, Corstens FH, Oyen WJ. Imaging of infectious diseases using [18F] fluorodeoxyglucose PET. Q J Nucl Med Mol Imaging. 2008;52:17–29.
Stary HC, Chandler AB, Dinsmore RE, Fuster V, Glagov S, Insull W Jr, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation. 1995;92:1355–74.
McEvoy JW, Blaha MJ, Defilippis AP, Budoff MJ, Nasir K, Blumenthal RS, et al. Coronary artery calcium progression: an important clinical measurement? A review of published reports. J Am Coll Cardiol. 2010;56:1613–22.
Blaha M, Budoff MJ, Shaw LJ, Khosa F, Rumberger JA, Berman D, et al. Absence of coronary artery calcification and all-cause mortality. J Am Coll Cardiol Img. 2009;2:692–700.
Sarwar A, Shaw LJ, Shapiro MD, Blankstein R, Hoffmann U, Cury RC, et al. Diagnostic and prognostic value of absence of coronary artery calcification. J Am Coll Cardiol Img. 2009;2:675–88.
Nadra I, Mason JC, Philippidis P, Florey O, Smythe CD, McCarthy GM, et al. Proinflammatory activation of macrophages by basic calcium phosphate crystals via protein kinase C and MAP kinase pathways: a vicious cycle of inflammation and arterial calcification? Circ Res. 2005;96:1248–56.
Joshi FR, Rajani NK, Abt M, Woodward M, Bucerius J, Mani V, et al. Does vascular calcification accelerate inflammation? A substudy of the dal-PLAQUE trial. J Am Coll Cardiol. 2016;67:69–78.
Hertzer NR, Beven EG, Young JR, O’Hara PJ, Ruschhaupt WF 3rd, Graor RA, et al. Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann Surg. 1984;199:223–33.
von Kemp K, van den Brande P, Peterson T, Waegeneers S, Scheerlinck T, Danau W, et al. Screening for concomitant diseases in peripheral vascular patients. Results of a systematic approach. Int Angiol. 1997;16:114–22.
Myers KS, Rudd JHF, Hailman EP, Bolognese JA, Burke J, Pinto CA, et al. Correlation between arterial FDG uptake and biomarkers in peripheral artery disease. J Am Coll Cardiol Img. 2012;5:38–45.
Purohit BS, Ailianou A, Dulguerov N, Becker CD, Ratib O, Becker M. FDG-PET/CT pitfalls in oncological head and neck imaging. Insights Imaging. 2014;5:585–602.
Kang WJ, Chung JK, So Y, Jeong JM, Lee DS, Lee MC. Differentiation of mediastinal FDG uptake observed in patients with non-thoracic tumours. Eur J Nucl Med Mol Imaging. 2004;31:202–7.
Kronmal RA, McClelland RL, Detrano R, Shea S, Lima JA, Cushman M, et al. Risk factors for the progression of coronary artery calcification in asymptomatic subjects: results from the multi-ethnic study of atherosclerosis (MESA). Circulation. 2007;115:2722–30.
Lee KK, Fortmann SP, Fair JM, Iribarren C, Rubin GD, Varady A, et al. Insulin resistance independently predicts the progression of coronary artery calcification. Am Heart J. 2009;157:939–45.
Fairweather D. Sex differences in inflammation during atherosclerosis. Clin Med Insights Cardiol. 2014;8 Suppl 3:49–59.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Sang-Geon Cho, Ki Seong Park, Jahae Kim, Sae-Ryung Kang, Seong Young Kwon, Hyun Ju Seon, Zeenat Jabin, Young Jae Kim, Geum-Cheol Jeong, Minchul Song, Ho-Chun Song, Jung-Joon Min, and Hee-Seung Bom declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Cho, SG., Park, K.S., Kim, J. et al. Prediction of coronary artery calcium progression by FDG uptake of large arteries in asymptomatic individuals. Eur J Nucl Med Mol Imaging 44, 129–140 (2017). https://doi.org/10.1007/s00259-016-3523-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-016-3523-1