
Abstract
Objective
To describe infraspinatus tendon injuries with associated intramuscular edema in light of more recently elucidated anatomical knowledge.
Material and methods
A retrospective review was performed to identify MRI cases with infraspinatus tendon injury accompanied by muscle edema. MR images were reviewed to evaluate the location of the injury, to assess the degree of tendon retraction, and to assess for muscular changes. Clinical and surgical data were reviewed when available.
Results
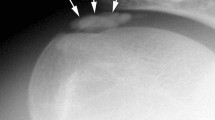
Twenty-three patients were identified (13 males, 10 females, mean age of 52 years). MRI demonstrated infraspinatus muscle edema in all cases with variably retracted infraspinatus tendon fibers. Three patients (13 %) presented acutely after traumatic falls, 11 patients (48 %) presented after a minor trauma or recalled event, and 9 patients (39 %) presented with more chronic symptoms. Of the nine patients who underwent arthroscopic surgery, six patients (67 %) did not have an identifiable corresponding lesion, despite the findings described on the preoperative MRI. In these six cases, some superficial fibers of the transverse portion of the infraspinatus tendon remained intact on the MRI. Three patients (13 %) had follow-up MRI examinations with one progressing to severe muscle atrophy, one without progression of existing muscle atrophy, and one with no atrophy on the initial or subsequent evaluation. Eighteen of 23 patients had concomitant partial-thickness or full-thickness tears of the adjacent supraspinatus tendon.
Conclusion
Injuries of the infraspinatus tendon with resultant muscle edema and variable muscle atrophy may, in fact, represent delaminating type injuries with differential retraction of a layered tendon and may be missed on arthroscopy.







Similar content being viewed by others

References
Lunn JV, Castellanos-Rosas J, Tavernier T, Barthélémy R, Walch G. A novel lesion of the infraspinatus characterized by musculotendinous disruption, edema, and late fatty infiltration. J Shoulder Elb Surg. 2008;17(4):546–53.
Tavernier TH, Walch G, Barthelemy R. Isolated lesion of the infraspinatus at the myotendinous junction: a new lesion. Clin Imaging. 2007:295–298.
Walch G, Nové-Josserand L, Liotard JP, Noël E. Musculotendinous infraspinatus ruptures: an overview. Orthop Traumatol Surg Res. 2009;95(7):463–70.
Guerini H, Pluot E, Pessis E, Thevenin F, Campagna R, Feydy A, et al. Tears at the myotendinous junction of the infraspinatus: ultrasound findings. Diagn Interv Imaging. 2015;96(4):349–56.
Kolbe AB, Collins MS, Sperling JW. Severe atrophy and fatty degeneration of the infraspinatus muscle due to isolated infraspinatus tendon tear. Skelet Radiol. 2012;41(1):107–10.
Chang EY, Chung CB. Current concepts on imaging diagnosis of rotator cuff disease. Semin Musculoskelet Radiol. 2014;18(4):412–24.
Tavernier T, Walch G, Barthelemy R, Nove-Josserand L, Liotard JP. Isolated lesion of the infraspinatus at the myotendinous junction: a new lesion. J Radiol. 2006;87(12 Pt 1):1875–82.
Kato A, Nimura A, Yamaguchi K, Mochizuki T, Sugaya H, Akita K. An anatomical study of the transverse part of the infraspinatus muscle that is closely related with the supraspinatus muscle. Surg Radiol Anat. 2012;34(3):257–65.
Taneja AK, Kattapuram SV, Chang CY, Simeone FJ, Bredella MA, Torriani M. MRI findings of rotator cuff myotendinous junction injury. AJR Am J Roentgenol. 2014;203(2):406–11.
Collin P, Treseder T, Lädermann A, Benkalfate T, Mourtada R, Courage O, et al. Neuropathy of the suprascapular nerve and massive rotator cuff tears: a prospective electromyographic study. J Shoulder Elb Surg. 2014;23(1):28–34.
Acknowledgments
Eric Y. Chang, MD, gratefully acknowledges support from the VA Clinical Science Research and Development (1IK2CX000749 and 1I01CX001388).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest.
Rights and permissions
About this article

Cite this article
Huang, B.K., Chang, E.Y. Delaminating infraspinatus tendon tears with differential retraction: imaging features and surgical relevance. Skeletal Radiol 46, 41–50 (2017). https://doi.org/10.1007/s00256-016-2506-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-016-2506-4