
Abstract
Objective
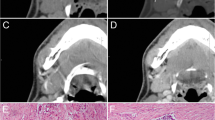
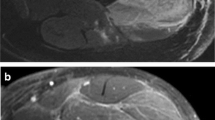
Myxofibrosarcoma frequently shows curvilinear extensions of high T2 signal that also enhance on magnetic resonance imaging; these “tails” represent fascial extension of tumor at histopathological examination. This study was performed to determine whether the tail sign is helpful in distinguishing myxofibrosarcoma from other myxoid-containing neoplasms.
Materials and methods
The study group consisted of 44 patients with pathologically proven myxofibrosarcoma; the control group consisted of 52 patients with a variety of other myxoid-predominant tumors. Three musculoskeletal radiologists independently evaluated T2-weighted (and/or short-tau inversion recovery) and post-contrast MR images for the presence of one or more enhancing, high-signal intensity, curvilinear projections from the primary mass. Sensitivity and specificity for the diagnosis of myxofibrosarcoma were calculated for each reader. Interobserver variability was assessed with kappa statistic and percentage agreement.
Results
A tail sign was deemed present in 28, 30, and 34 cases of myxofibrosarcoma and in 11, 9, and 5 of the controls for the three readers respectively, yielding a sensitivity of 64–77 % and a specificity of 79–90 %. The interobserver agreement was moderate-to-substantial (kappa = 0.626).
Conclusion
The tail sign at MRI is a moderately specific and sensitive sign for the diagnosis of myxofibrosarcoma relative to other myxoid-containing tumors.






Similar content being viewed by others

References
Willems SM, Wiweger M, Graadt van Roggen JF, Hogendoorn PCW. Running GAGs: myxoid matrix in tumor pathology revisited. What’s in it for the pathologist? Virchows Arch. 2010;456:181–92.
Nishimura H, Zhang Y, Ohkuma K, Uchida M, Hayabuchi N, Sun S. MR imaging of soft-tissue masses of the extraperitoneal spaces. Radiographics. 2001;21(5):1141–54.
Waters B, Panicek DM, Lefkowitz RA, Healey JH, Athanasian EA, Brennan MF. Low-grade myxofibrosarcoma; CT and MRI patterns in recurrent disease. AJR. 2007;188:193–8.
Sung MS, Kang HS, Suh JS, et al. Myxoid liposarcoma: appearance at MR imaging with histologic correlation. Radiographics. 2000;20:1007–19.
Dinauer PA, Brixey CJ, Moncur JT, Fanburg-Smith JC, Murphey MD. Pathologic and MR imaging features of benign fibrous soft-tissue tumors in adults. Radiographics. 2007;27:173–87.
Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. From the archives of the AFIP: benign musculoskeletal lipomatous lesions. Radiographics. 2004;24:1433–66.
Ohguri T, Aoki T, Hisaoka M, et al. Differential diagnosis of benign peripheral lipoma from well-differentiated liposarcoma on MR imaging: is comparison of margins and internal characteristics useful? AJR Am J Roentgenol. 2003;180:1689–94.
Willems SM, Debiec-Rychter M, Szuhai K, Hogendoorn PCW, Sciot R. Local recurrence of myxofibrosarcoma is associated with increase in tumor grade and cytogenetic aberrations, suggesting a multistep tumor progression model. Mod Pathology. 2006;19:407–16.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74.
Murphey MD, Arcara LK, Fanburg-Smith J. From the archives of the AFIP: imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation. Radiographics. 2005;25:1371–95.
Angervall L, Kindblom LG, Merck C. Myxofibrosarcoma. A study of 30 cases. Acta Pathol Microbiol Scand. 1997;85A:127–40.
Huang HY, Lal P, Qin J, Brennan MF, Antonescu CR. Low-grade myxofibrosarcoma: a clinicopathologic analysis of 49 cases treated at a single institution with simultaneous assessment of a efficacy of 3-tier and 4-tier grading system. Hum Pathol. 2004;35:612–21.
Weiss SW, Enzinger FM. Myxoid variant of malignant fibrous histiocytoma. Cancer. 1977;39:1672–85.
Mentzel T, Calonje E, Wadden C, et al. Myxofibrosarcoma. Clinicopathologic analysis of 75 cases with emphasis on the low-grade variant. Am J Surg Pathol. 1996;20:391–405.
Manoso MW, Pratt J, Healey JH, Boland PJ, Athanasian EA. Infiltrative MRI pattern and incomplete initial surgery compromise local control of myxofibrosarcoma. Clin Orthop Relat Res. 2006;450:89–94.
Kaya M, Wada T, Nagoya S, et al. MRI and histological evaluation of the infiltrative growth pattern of myxofibrosarcoma. Skeletal Radiol. 2008;37:1085–90.
Erlemann R, Reiser MF, Peters PE, et al. Musculoskeletal neoplasms: static and dynamic Gd-DTPA—enhanced MR imaging. Radiology. 1989;171:767–73.
Narváez JA, Martinez S, Dodd LG, Brigman BE. Clinical observations: acral myxoinflammatory fibroblastic sarcomas: MRI findings in four cases. AJR Am J Roentgenol. 2007;188:1302–5.
Tateishi U, Hasegawa T, Onaya H, Satake M, Arai Y, Moriyama N. Myxoinflammatory fibroblastic sarcoma: MR appearance and pathologic correlation. AJR Am J Roentgenol. 2005;184:1749–53.
Presant CA, Russell WO, Alexander RW, Fu YS. Soft-tissue and bone sarcoma histopathology peer review: the frequency of disagreement in diagnosis and the need for second pathology opinions. The Southeastern Cancer Study Group experience. J Clin Oncol. 1986;4:1658–61.
Acknowledgements
We would like to thank Roselyn Latorre for her timely assistance with data organization for this project.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lefkowitz, R.A., Landa, J., Hwang, S. et al. Myxofibrosarcoma: prevalence and diagnostic value of the “tail sign” on magnetic resonance imaging. Skeletal Radiol 42, 809–818 (2013). https://doi.org/10.1007/s00256-012-1563-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-012-1563-6