
Abstract
Summary
An age–period cohort model was fitted to analyse time effects on hip fracture incidence rates by sex (Portugal, 2000–2008). Rates increased exponentially with age (age effect). Incidence rates decreased after 2004 for women and were random for men (period effect). New but comprehensive fluctuations in risk were coincident with major political/economic changes (cohort effect).
Introduction
Healthcare improvements have allowed prevention but have also increased life expectancy, resulting in more people being at risk. Our aim was to analyse the separate effects of age, period and cohort on incidence rates by sex in Portugal, 2000–2008.
Methods
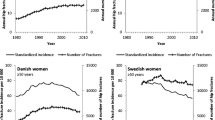
From the National Hospital Discharge Register, we selected admissions (aged ≥49 years) with hip fractures (ICD9-CM, codes 820.x) caused by low/moderate trauma (falls from standing height or less), readmissions and bone cancer cases. We calculated person-years at risk using population data from Statistics Portugal. To identify period and cohort effects for all ages, we used an age–period–cohort model (1-year intervals) followed by generalised additive models with a negative binomial distribution of the observed incidence rates of hip fractures.
Results
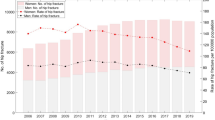
There were 77,083 hospital admissions (77.4 % women). Incidence rates increased exponentially with age for both sexes (age effect). Incidence rates fell after 2004 for women and were random for men (period effect). There was a general cohort effect similar in both sexes; risk of hip fracture altered from an increasing trend for those born before 1930 to a decreasing trend following that year. Risk alterations (not statistically significant) coincident with major political and economic change in the history of Portugal were observed around birth cohorts 1920 (stable–increasing), 1940 (decreasing–increasing) and 1950 (increasing–decreasing only among women).
Conclusions
Hip fracture risk was higher for those born during major economically/politically unstable periods. Although bone quality reflects lifetime exposure, conditions at birth may determine future risk for hip fractures.



Similar content being viewed by others

References
Hopkins RB, Goeree R, Pullenayegum E, Adachi JD, Papaioannou A, Xie F, Thabane L (2011) The relative efficacy of nine osteoporosis medications for reducing the rate of fractures in post-menopausal women. BMC Musculoskelet Disord 12:209. doi:10.1186/1471-2474-12-209
Ioannidis G, Flahive J, Pickard L, Papaioannou A, Chapurlat RD, Saag KG, Silverman S, Anderson FA Jr, Gehlbach SH, Hooven FH, Boonen S, Compston JE, Cooper C, Diez-Perez A, Greenspan SL, Lacroix AZ, Lindsay R, Netelenbos JC, Pfeilschifter J, Rossini M, Roux C, Sambrook PN, Siris ES, Watts NB, Adachi JD (2012) Non-hip, non-spine fractures drive healthcare utilization following a fracture: the Global Longitudinal Study of Osteoporosis in Women (GLOW). Osteoporos Int. doi:10.1007/s00198-012-1968-z
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359(9321):1929–1936. doi:10.1016/s0140-6736(02)08761-5
Hunter DJ, Sambrook PN (2000) Bone loss: epidemiology of bone loss. Arthritis Res 2(6):441–445. doi:10.1186/ar125
Cooper C, Westlake S, Harvey N, Javaid K, Dennison E, Hanson M (2006) Review: developmental origins of osteoporotic fracture. Osteoporos Int 17(3):337–347. doi:10.1007/s00198-005-2039-5
Baird J, Kurshid MA, Kim M, Harvey N, Dennison E, Cooper C (2011) Does birthweight predict bone mass in adulthood? A systematic review and meta-analysis. Osteoporos Int 22(5):1323–1334. doi:10.1007/s00198-010-1344-9
Langley J, Samaranayaka A, Davie G, Campbell AJ (2011) Age, cohort and period effects on hip fracture incidence: analysis and predictions from New Zealand data 1974–2007. Osteoporos Int 22(1):105–111. doi:10.1007/s00198-010-1205-6
Rosengren B, Ahlborg H, Mellstrom D, Nilsson J, Bjork J, Karlsson M (2012) Secular trends in Swedish hip fractures 1987–2002: birth cohort and period effects. Epidemiology 23(4):623–630
Evans JG, Seagroatt V, Goldacre MJ (1997) Secular trends in proximal femoral fracture, Oxford record linkage study area and England 1968–86. J Epidemiol Commun Health 51(4):424–429
Jean S, O’Donnell S, Lagace C, Walsh P, Bancej C, Brown JP, Morin S, Papaioannou A, Jaglal SB, Leslie WD (2013) Trends in hip fracture rates in Canada: an age–period–cohort analysis. J Bone Miner Res 28(6):1283–1289. doi:10.1002/jbmr.1863
Cumming RG, Nevitt MC, Cummings SR (1997) Epidemiology of hip fractures. Epidemiol Rev 19(2):244–257
Fisher A, Martin J, Srikusalanukul W, Davis M (2010) Bisphosphonate use and hip fracture epidemiology: ecologic proof from the contrary. Clin Interv Aging 5:355–362. doi:10.2147/cia.s13909
Reginster JY, Kaufman JM, Goemaere S, Devogelaer JP, Benhamou CL, Felsenberg D, Diaz-Curiel M, Brandi ML, Badurski J, Wark J, Balogh A, Bruyere O, Roux C (2012) Maintenance of antifracture efficacy over 10 years with strontium ranelate in postmenopausal osteoporosis. Osteoporos Int 23(3):1115–1122. doi:10.1007/s00198-011-1847-z
Fisher AA, O’Brien ED, Davis MW (2009) Trends in hip fracture epidemiology in Australia: possible impact of bisphosphonates and hormone replacement therapy. Bone 45(2):246–253. doi:10.1016/j.bone.2009.04.244
Alves SM, Economou T, Oliveira C, Ribeiro AI, Neves N, Goméz-Barrena E, Pina MF (2013) Osteoporotic hip fractures: bisphosphonates sales and observed turning point in trend. A population-based retrospective study. Bone 53(2):430–436
Cooper C, Cole ZA, Holroyd CR, Earl SC, Harvey NC, Dennison EM, Melton LJ, Cummings SR, Kanis JA (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22(5):1277–1288. doi:10.1007/s00198-011-1601-6
Barros P, de Almeida Simões J (2007) Portugal: Health system review, vol 9 (5). Health Systems in Transition. WHO Regional Office for Europe
ACSS (2011) Auditoria da codificação clínica [Clinical codification Audits]. http://portalcodgdh.min-saude.pt/index.php/Auditoria_da_codificação_cl%C3%ADnica. 2012
Melton LJ 3rd, Kearns AE, Atkinson EJ, Bolander ME, Achenbach SJ, Huddleston JM, Therneau TM, Leibson CL (2009) Secular trends in hip fracture incidence and recurrence. Osteoporos Int 20(5):687–694. doi:10.1007/s00198-008-0742-8
INE (2012) Instituto Nacional de Estatística. 2011
Carstensen B (2007) Age–period–cohort models for the Lexis diagram. Stat Med 26(15):3018–3045. doi:10.1002/sim.2764
Morris JA, Gardner MJ (2000) Epidemiological studies. In: Altman DG, Machin D, Bryant TN, Gardner MJ (eds) Statistics with confidence, second edition ed. BMJ Books, Bristol
Faraway JJ (2006) Extending the linear model with R: generalized linear, mixed effects and nonparametric regression models. Texts in statistical science series. Chapman & Hall, Boca Raton
Carstensen B, Plummer M, Laara E, Hills M (2012) Epi: a package for Statistical analysis in epidemiology. R package version 1.1.40 ed
Holford TR (1983) The estimation of age, period and cohort effects for vital rates. Biometrics 39:311–324
Clements MS, Armstrong BK, Moolgavkar SH (2005) Lung cancer rate predictions using generalized additive models. Biostatistics 6(4):576–589. doi:10.1093/biostatistics/kxi028
Hastie T, Tibshirani R (1995) Generalized additive models for medical research. Stat Methods Med Res 4(187–196)
Wood SN (2011) Fast stable restricted maximum likelihood and marginal likelihood estimation of semiparametric generalized linear models. J R Stat Soc (B) 73(1):3–36
Samelson EJ, Zhang Y, Kiel DP, Hannan MT, Felson DT (2002) Effect of birth cohort on risk of hip fracture: age-specific incidence rates in the Framingham Study. Am J Public Health 92(5):858–862
Heaney RP, Abrams S, Dawson-Hughes B, Looker A, Marcus R, Matkovic V, Weaver C (2000) Peak bone mass. Osteoporos Int 11(12):985–1009
História de Portugal [History of Portugal] (1994). Círculo de Leitores
Rothman KJ, Greenland S (2005) Causation and causal inference in epidemiology. Am J Public Health 95(Suppl 1):S144–S150. doi:10.2105/ajph.2004.059204
INE (2001) Estatísticas Históricas Portuguesas [Historical statistics in Portugal].
Melton LJ 3rd, O’Fallon WM, Riggs BL (1987) Secular trends in the incidence of hip fractures. Calcif Tissue Int 41(2):57–64
Acknowledgments
This work was supported by FEDER funds through the Programa Operacional Factores de Competitividade (COMPETE) and by Portuguese funds through Fundação para a Ciência e a Tecnologia (FCT) within the framework of the project PEst-C/SAU/LA0002/2011 and by PTDC/SAU-EPI/113424/2009 grant and SFRH/BD/40978/2007 fellowship.
We like to acknowledge the Central Administration of Health Services (ACSS) for the data from the National Hospital Discharge Register. We also like to acknowledge Paulo Nossa for helping with the understanding of economic, social and political history of Portugal.
Conflict of Interests
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alves, S.M., Castiglione, D., Oliveira, C.M. et al. Age–period–cohort effects in the incidence of hip fractures: political and economic events are coincident with changes in risk. Osteoporos Int 25, 711–720 (2014). https://doi.org/10.1007/s00198-013-2483-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2483-6