
Abstract
This article aims to assess how the risk perceptions of smokers affect survival expectations and subjective health. Data from the Survey of Health, Ageing and Retirement in Europe, which include a numerical measure of subjective survival probability, are used to estimate a joint recursive system of equations that describe the relationships among survival expectations, subjective health status and smoking duration. A finite mixture model is used to address endogeneity and unobservable heterogeneity. This approach allows for two types of individuals with different observable characteristics to be identified in the examined population. We find that only in the population of the first type, current and former smokers incorporate the effects of smoking duration into their assessments of survival probabilities. For both types, quitting smoking affects current perceptions of smoking risks, causing the overestimation of both survival probability and subjective health.
Similar content being viewed by others

Notes
Schoenbaum (1997) finds that non-smokers overestimate the mortality risk of smoking while heavy smokers underestimate the negative effect of smoking intensity on survival probability. Viscusi (1990) and Viscusi and Hakes (2008) find that smokers overestimate the smoking-related risks of lung cancer, the life expectancy loss and total mortality risk. They also show that higher risk perception lowers the probability of beginning to smoke and increase the probability of quitting. Smith et al. (2001a, b) find significant heterogeneity among smokers. Heavy smokers are excessively optimistic about their future survival, whereas current smokers reduce their survival expectations more dramatically than former and never smokers when they experience smoking-related health shocks. More evidence supporting underestimation of the health risks of smoking is provided by Hammar and Johansson-Stenman (2004) and Khwaja et al. (2007).
Carbone et al. (2005) compare and contrast two hypothetical and extreme scenarios: in one scenario, individuals’ beliefs about the probability of dying depend on both their current health and prior smoking habit (the irreversible case), whereas in the other scenario, these beliefs depend only on health status (the reversible case).
Myopic models describe smokers as irrational addicts who fail to consider the impact of current consumption on their future consumption and utility (see Thaler and Shefrin 1981; Winston 1980). Tobacco consumption only depends on current price and past consumption; individuals care more about current utility derived from smoking than about the future. The negative effects of smoking on an individual’s future health and survival are not considered. The theory of rational addiction regards addictive tobacco consumption as a rational choice (Becker and Murphy 1988; Becker et al. 1994). Smokers are forward-looking individuals who care about the effects of today’s consumption on their future consumption and utility; the detrimental effects of smoking are internalised when making consumption decisions.
The SHARE collects data in 2006–2007 (wave 2) and in 2008–2009 (SHARELIFE). Ideally, the longitudinal dimension should be exploited in the analysis. However, we cannot used SHARELIFE because it does not investigate survival expectations and smoking behaviour. Panel data analysis is excellent for addressing unobservable heterogeneity and the endogeneity of regressors (e.g. internal instruments could be used in the absence of valid instrumental variables). However, the availability of only two survey waves limits the potential for using panel analysis (only a balanced sample can be used but at the cost of a loss of about 45 % of observations due to attrition and item non-response). Attrition bias represents another challenge to the use of panel analysis because only the respondents who are less frail would remain in the sample. Moreover, in addition to mortality, which is per se related to the health measures that are utilised in this study, other reasons for drop-outs might create bias in a panel analysis (e.g. individuals whose health dramatically deteriorates between waves may not participate in wave 2 of the survey due to either a serious illness or institutionalisation). Thus, appropriate techniques that are based on inverse probability weights, or calibrated weights, should be employed for a panel analysis. However, this solution is not viable because the EM algorithm used in the present study already utilises weights in the estimation procedure.
Individuals older than 85 years of age have been excluded because they are not heavily represented in the target sample and because they may have provided assessments that were less accurate than the responses of other survey participants. Moreover, most individuals of the same age are likely to be living in nursing homes, and the SHARE is not representative of the institutionalised population.
These target ages correspond to the age categories 50–65, 66–70, 71–75, 76–80 and 81–85, with a difference from each respondent’s current age ranging between 14 and 25 years. We exclude from the individuals those who were not matched to the appropriate target age.
The two events living better and living worse in the future are complements; therefore, the two subjective probabilities associated with these questions must sum to one. A subjective probability of 0 for both events indicates a high expected probability that the standard of living in the future will be unchanged. Using a tolerance level of 0.10, we exclude 831 individuals (about 3 % of the original sample) for whom the sum of the probabilities for the two questions is greater than 1.10. As a robustness check, we estimate the simultaneous recursive model with and without the use of this sample restriction. Estimated coefficients are very similar in magnitude; the signs and significance levels are unaffected. The log-likelihood and the information criteria favour the model estimated using the sample that excludes non-coherent responses.
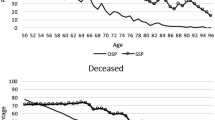
Winter (2008) use information about the vital status of respondents at subsequent waves to demonstrate that, for each level of SAH, the average SSP is higher for survivors than for individuals who are deceased by wave 2 of the SHARE; he finds that SSP reported in wave 1 well predicts mortality that occurs between waves.
Note that information on vital status at wave 2 is unavailable for about 29 % of our sample; therefore, statistics and estimates are computed from a smaller sample. As a robustness check, we have estimated a probit model for the probability of dying between waves 2 and 3. Results, available upon request, confirm that SSP is a good predictor of subsequent mortality.
Etilè and Milcent (2006) suggest the aggregation of responses into two broader categories as a method of reducing the reporting heterogeneity bias. In particular, they transform SAH into a binary indicator of poor/non-poor health. To account for reporting style Jürges (2007) proposes a five-point scale. As a robustness check, we re-estimated the model presented in Sect. 4 with ordinal values of SAH. Coefficients in the SSP equation of both models are very similar in magnitude; have the same signs and significance levels. For the purpose of our analysis, the binary version of SAH appears to accurately capture both the correlation between subjective health and survival expectations and the heterogeneity among different types of smokers with respect to SAH. Results are available upon request.
This indicator of household composition suffer from a remarkable problem of item non-response in wave 2, thus providing another motive for using wave 1 only.
The beta distribution is often employed for proportions or subjective beliefs about the probabilities of future events (Ferrari and Cribari-Neto 2004; Smithson and Verkuilen 2006), because it well models continuous and bounded variables that are characterised by spikes at certain response foci. We rescale \(y_{1}\) to lie in the interval (0, 1). To avoid taking the logarithm of zeros and ones, \(y_1 =\left( {\frac{\mathrm{{SSP}}}{100}\cdot ({N-1}) +a}\right) \), where \(N\) is the sample size and \(a\) is a constant (in this case, \(a = 0.5\)). Alternative transformations can be utilised.
The logarithm transformation of the continuous indicator is used to ensure flexibility in the relationship.
Although lifestyle choices are likely endogenous to subjective health and survival expectations, our model does not control for this issue, but instead assumes the exogeneity of these factors. This assumption might represent a limitation of the analysis. As a robustness check, we have compared our model with another one that excludes lifestyles, but raises the issue of omitted variable bias. The coefficients of SAH and smoking in the SSP equation are very similar in magnitude for these two models; the signs and significance levels are unchanged. Information criteria favour the model that includes lifestyles. Results are available upon request.
This indicator of pessimism, which denotes whether a respondent reports that she has no hope for the future, is one of the items that is collected by the SHARE to define the EURO-D symptoms scale, which measures mental health.
Dardanoni and Li Donni (2012) estimate a finite mixture model to explore the self-reporting effect of individual characteristics on SAH, and assume two latent classes of good health and bad health (in essence, SAH is conditional on an individual’s unobservable true health). A similar framework is employed by our model, which assumes that true mortality risk and true health status of an individual directly go into the unobservable component of the model; thus, the latent classes are characterised by different states of unobservable health and true mortality risk.
The Weibull has been chosen among other distributions on the basis of information criteria and Cox–Snell residuals test.
The model is parameterised with respect to the accelerated failure time metric. The estimated coefficients should, therefore, be interpreted in terms of acceleration (or deceleration) of time until an individual ceases smoking.
FM models provide an alternative and flexible method of accounting for the unobserved individual effect in the case of non-linear models (see Cameron and Trivedi 2005). They have recently been used with panel data for pooled, population-averaged and random-effects models (see Bago d’Uva 2006; Bago d’Uva and Jones 2009) because of the following advantages: any parametric distribution for the unobservable heterogeneity is required and heterogeneity is allowed in the intercept as well as in the slopes. Deb and Trivedi (2013) have recently proposed a fixed-effect FM model for count data in short balanced panels (minimum T \(=\) 4) with exogenous regressors, using the EM algorithm. This type of extension to our model is problematic due to the availability of only two waves and the prospect of attrition bias.
Mroz (1999) uses a latent factor model, which is a type of FM, to control for the endogeneity of a regressor. He shows that his methodology performs better than alternative estimators, particularly in the case of non-normality.
The baseline individual is a single female from the Netherlands who is between 81 and 85 years of age, is in fair or poor health, has never smoked, maintains a healthy lifestyle, earns a low level of income, has no education and is unemployed (or works as a housekeeper).
Partial effects are computed for each individual as the change in the probability that SAH \(=\) 1 caused by a change in a covariate, then averaged across the whole sample. Therefore, they refer to the entire population. We use the finite difference method for dummy variables and the calculus method for continuous variables as in Wooldridge (2002).
Table B.4, available in the electronic supplementary material, compares individuals in sub-sample 1, drawn from the first population, with individuals in sub-sample 2. We find that these two groups of individuals differ in terms of observable characteristics and particularly in terms of smoking behaviour. Such differences are in line with the FM model results that we have previously discussed.
References
Adda J, Lechene V (2012) Health selection and the effects of smoking on mortality. IZA discussion papers 6206
Arcidiacono P, Sieg H, Sloan F (2007) Living rationally under the volcano? An empirical analysis of heavy drinking and smoking. Int Econ Rev 48(1):37–65
Bago d’Uva T (2006) Latent class models for use of health care. Health Econ 15:329–343
Bago d’Uva T, Jones AM (2009) Health care utilisation in Europe: new evidence from the ECHP. J Health Econ 28:265–279
Balia S, Jones AM (2011) Catching the habit: a study of inequality of opportunity in smoking-related mortality. J R Stat Soc A 174(1):175–194
Becker GS, Murphy K (1988) A theory of rational addiction. J Polit Econ 96(4):675–700
Becker GS, Grossman M, Murphy KM (1994) An empirical analysis of cigarette addiction. Am Econ Rev 84(3):396–418
Bruine de Bruin W, Fischbeck PS, Stiber NA, Fischhoff B (2002) What number is “fifty–fifty”?: redistributing excessive 50 % responses in elicited probabilities. Risk Anal 922(4):713–723
Cameron AC, Trivedi PK (2005) Microeconometrics. Methods and applications. Cambridge University Press, New York
Carbone JC, Kverndokkb S, Røgebergb OJ (2005) Smoking, health, risk, and perception. J Health Econ 24:631–653
Cawley J, Ruhm CJ (2011) Chapter Three-the economics of risky health behaviors. In: Mark V Pauly, Thomas G Mcguire, Pedro P Barros (eds) Handbook of Health Economics, vol 2. Elsevier, Amsterdam, pp 95–199
Chaloupka F (1991) Rational addictive behavior and cigarette smoking. J Polit Econ 99(4):722–742
Chapman S, Wong W, Smith W (1983) Self-exempting beliefs about smoking and health: differences between smokers and ex-smokers. Am J Public Health 83(2):215–219
Cutler DM, Glaeser EL (2009) Why do Europeans smoke more than Americans? In: Wise DA (ed) Developments in the economics of aging. NBER book, Cambridge, MA, pp 255–282
Dardanoni V, Li Donni P (2012) Reporting heterogeneity in health: an extended latent class approach. Appl Econ Lett 19(12):1129–1133
Deaton AS, Paxson C (1998) Ageing and inequality in income and health. Am Econ Rev Papers Proc 88:248–253
Deb P, Trivedi PK (2006) Specification and simulated likelihood estimation of a non-normal treatment-outcome model with selection: application to health care utilization. Econom J 9:307–331
Deb P, Trivedi PK (2013) Finite mixture for panels with fixed effects. J Econom Methods 2(1):35–51. doi:10.1515/jem-2012-0018
Delavande A, Rohwedder S (2011) Differential survival in Europe and the United States: estimates based on subjective probabilities of survival. Demography 48:1377–1400
Dempster AP, Laird N, Rubin DB (1977) Maximum likelihood from incomplete data via EM algorithm. J R Stat Soc B 34(1):1–38
Di Novi C (2010) The influence of traffic-related pollution on individuals’ life-style: results from the BRFSS. Health Econ 19:1318–1344
Dominitz J, Manski CF (1997) Using expectation data to study subjective income expectations. J Am Stat Assoc 92:855–867
Douglas S, Hariharan G (1994) The hazard of starting smoking: estimates from a split population duration model. J Health Econ 13(2):213–230
Etilè F, Milcent C (2006) Income-related reporting heterogeneity in self-assessed health: evidence from France. Health Econ 15:956–981
Ferrari S, Cribari-Neto F (2004) Beta regression for modelling rates and proportions. J Appl Stat 31(7):799–815
Forster M, Jones AM (2001) The role of tobacco taxes in starting and quitting smoking: duration analysis of British data. J R Stat Soc A 164:517–547
Gilleskie D, Strumpf KL (2005) The behavioral dynamics of youth smoking. J Hum Resour 40:822–866
Grossman M (1972) On the concept of health capital and the demand for health. J Polit Econ 80(2):223–255
Guiso L, Tiseno A, Winter J (2005) Expectations. In: Börsch-Supan A, Brugiavini A, Jürges H, Mackenbach J, Siegrist J, Weber G (eds) Health, Ageing, and Retirement in Europe. Mannheim, Mannheim Research Institute for the Economics of Aging, pp 332–338
Hammar H, Johansson-Stenman O (2004) The value of risk-free cigarettes-do smokers underestimate the risk? Health Econ 13:59–71
Hill D, Perry M, Willis R (2005) Estimating knightian uncertainty from survival probabilities on the HRS, Manuscript. University of Michigan
Hurd M, McFadden D, Merrill A (1999) Predictors of mortality among the elderly. NBER working paper 7440
Hurd M, McGarry K (1995) Evaluation of the subjective probabilities of survival in the health and retirement study: data quality and early results. J Hum Resour 30:268–S292
Hurd M, McGarry K (2002) The predictive validity of subjective probabilities of survival. Econ J 112:966–985
Jacho-Chávez DT, Trivedi PK (2009) Computational considerations in empirical microeconometrics: selected examples. In: Mills TC, Patterson K (eds) Palgrave handbook of econometrics, vol 2. Applied Econometrics. Part V. Palgrave Macmillan, Basingstoke
Jarvis MJ (1996) The association between having children, family size and smoking cessation in adults. Addiction 91(3):427–434
Jürges H (2007) True health vs response styles: exploring cross-country differences in self-reported health. Health Econ 16:163–178
Khwaja A, Sloan F, Chung S (2007) The relationship between expectations and behaviours: mortality expectations and smoking decisions. J Risk Uncertain 35:179–201
Manski CF (2004) Measuring expectations. Econometrica 72(5):1329–1376
Marcus BH, Lewis BA, Hogan J, King TK, Albrecht AE, Bock B, Parisi AF, Niaura R, Abrams DB (1999) The efficacy of exercise as an aid for smoking cessation in women: a randomized controlled trial. Arch Intern Med 159:1229–1234
McLachlan GJ, Krishnan T (1996) The EM algorithm and extensions. Wiley, New York
McLachlan J, Peel D (2000) Finite mixture models. Wiley, New York
Michaud PC, Goldman D, Lakdawalla D, Gailey A, Zheng Y (2011) Differences in health between Americans and Western Europeans: effects on longevity and public finance. Soc Sci Med 73:254–263
Mroz TA (1999) Discrete factor approximations in simultaneous equation models: estimating the impact of a dummy endogenous variable on a continuous outcome. J Econom 92:233–274
Paolino P (2001) Maximum likelihood estimation of models with beta-distributed dependent variables. Polit Anal 9(4):325–346
Peracchi F, Perotti V (2010) Subjective survival probabilities and life tables: evidence from Europe. EIEF working paper 10/16
Schafer JL (1997) Analysis of incomplete multivariate data, vol 72. In: Monographs on statistics ad applied probability. Chapman and Hall, London
Schoenbaum M (1997) Do smokers understand the mortality effects of smoking? Evidence from the health and retirement survey. Am J Public Health 87(5):755–759
Smith VK, Taylor DH, Sloan FA (2001a) Longevity expectations and death: can people predict their own demise? Am Econ Rev 91:1126–1134
Smith VK, Taylor DH, Sloan FA, Johnson FR, Desvousge WH (2001b) Do smokers respond to health shocks? Rev Econ Stat 83(4):675–687
Smithson M, Verkuilen J (2006) A better lemon squeezer? Maximum likelihood regression with Beta distributed dependent variables. Psychol Methods 11(1):54–71
Thaler R, Shefrin H (1981) An economic theory of self-control. J Political Econ 89(2):392–406
van Doorslaer E, Gerdtham UG (2003) Does inequality in self-assessed health predict inequality in survival by income? Evidence from Swedish data. Soc Sci Med 57:1621–1629
Viscusi WK (1990) Do smokers underestimate risks? J Polit Econ 98(6):1253–1269
Viscusi WK (1991) Age variations in risk perceptions and smoking decisions. Rev Econ Stat 73(4):577–588
Viscusi WK, Hakes JK (2008) Risk beliefs and smoking behavior. Econ Inq 46(1):45–59
WHO (2011) Noncommunicable diseases country profiles 2011. http://www.who.int
Winston G (1980) Addiction and backsliding: the theory of compulsive consumption. J Econ Behav Organ 1:295–324
Winter J (2008) Expectations and attitudes. In First results from the Survey of Health, Ageing and Retirement in Europe (2004–2007). In: Börsch-Supan A, Brugiavini A, Jürges H, Kapteyn A, Mackenbach J, Siegrist J, Weber G (eds) Starting the longitudinal Dimension. MEA, Mannheim, pp 306–311
Wooldridge J (2002) Econometric analysis of cross section and panel data. MIT Press, Cambridge
Acknowledgments
This paper uses data from release 2.5.0 of the SHARE results; these data are current as of May 24th, 2011. The study data are supplied by CentERdata. The collection of SHARE data in 2004–2007 was primarily funded by the 5th and 6th framework programmes of the European Commission. More information about the SHARE is available at http://www.share-project.org/. I wish to thank Andrew Jones, Casey Queen, Teresa Bago d’Uva, Martin Forster, Rinaldo Brau, Silvana Robone, Cinzia Di Novi, Emanuela Marrocu, participants in the SIEP conference (2008) and in the iHEA congress in Toronto (2011), two anonymous referee and an anonymous associate editor for valuable suggestions and comments.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Balia, S. Survival expectations, subjective health and smoking: evidence from SHARE. Empir Econ 47, 753–780 (2014). https://doi.org/10.1007/s00181-013-0750-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00181-013-0750-1