
Abstract
We examine the impact of assisted reproductive technology on women’s choice to pursue professional careers. We hypothesize that the availability of assisted reproductive technology increases the expected benefits of a professional degree by allowing women to delay childbearing in their 20s and 30s while establishing their careers, thereby reaping greater financial benefit from human capital investment. State-level timing differences in the enactment of laws which mandated infertility treatment coverage in employer-sponsored health plans allow us to exploit state, year, and cohort variation in women’s ages at the time the laws are passed. These insurance mandates dramatically increase access to assisted reproductive technology. Using a triple difference strategy, we find that a mandate to cover assisted reproductive technology does increase the probability that a woman chooses to invest in a professional degree and to work in a professional career.
Similar content being viewed by others

1 Introduction
Advances in reproductive technology have had a significant impact on women’s labor force choices. For example, as shown in Goldin and Katz (2002), the ability to delay childbearing through the use of oral contraceptives increased women’s age at first marriage, allowing them more time to invest in professional degrees. However, the expected benefits of investing in a professional degree are likely to be mitigated if a woman postpones having children until merely the early years of her career, specifically before a promotion or partnership is achieved. This is due to the well-documented fact that taking breaks from work early in one’s career can result in significant penalties to lifetime earnings (Miller 2011; Leung et al. 2016). Moreover, these costs have climbed over the past decades as the fraction of women entering professional and more highly compensated occupations has increased.Footnote 1
Another factor entering into a woman’s career decision is a biological constraint. If women delay childbearing, they are faced with declining fecundity as they age. While contraceptives make it easier for women to postpone childbearing, there remains a biological limit to that delay. It can be argued that the costs of interruption to a professional career are increasingly diminished the further into the future a woman can delay having children, since a longer time horizon at work allows her to better establish her career. For example, she may acquire more job-specific human capital or obtain a promotion before taking time off for childbearing. Once she has accumulated more experience, a woman is better able to retain her value to her employer, and thus mitigate potential losses to her lifetime earnings.
In this paper, we examine the impact of assisted reproductive technology (ART) on women’s education and career choices. By potentially expanding the time horizon for childbearing to a later point in a woman’s professional career, ART may increase the expected returns to investing in a professional degree with a resulting change in occupational choice. Although earlier research has shown that the increased efficacy and availability of ART has had a significant impact on the use of infertility treatments (Bitler and Schmidt 2012), marriage timing (Abramowitz 2014), fertility among older women (Schmidt 2007; Buckles 2013) and allocation of labor supply over the life cycle (Buckles 2007), the existing literature does not speak directly to the impact of ART on human capital investment and career choice.
ART is distinct from other reproductive therapies in a crucial way. Not only is ART extremely expensive but unlike other reproductive technologies such as contraceptives, it is generally not covered by insurance. Moreover, to the extent that health insurance coverage for ART is available, it is typically the result of state government mandates. Thus, in states where such mandates exist, the costs of postponing childbearing in order to invest in human capital should be lower. In particular, this cost decrease will be the most significant to women in careers that carry high wage returns to advanced schooling and intensive on-the-job training. This characteristic of the ART mandates generates an interesting policy question: are women who reside in states where ART coverage is mandated more likely to invest in career-oriented human capital?
Using a a difference in difference in differences (triple difference) approach, we find that the presence of a mandate to cover ART increases the probability that college-educated women are in professional occupations by 1.2 percentage points, and increases the probability of completing a professional degree by 0.8 percentage points. Our definition of treatment by the mandate allows us to interpret our results as the causal effect of access to ART on human capital stock. These point estimates support the hypothesis that young women view the early years of a professional career as an investment period, in which declining fertility is a significant cost of investment. Although we primarily focus on the investment in education, career-driven migration is an alternative investment decision that may be impacted significantly by the ability to delay fertility. It is likely that the mandates additionally increase human capital stock through high-skilled emigration into a state with ART coverage.
The remainder of the paper is organized as follows: Section 2 provides a brief background on infertility and insurance coverage for fertility treatments, Section 3 presents the conceptual framework, Section 4 describes the dataset, Section 5 explains our empirical strategy, Section 6 discusses the results, Section 7 shows robustness checks, and Section 8 concludes.
2 Background
According to the Centers for Disease Control and Prevention (CDC 2014), fecundity begins to decrease rapidly after a woman turns 35, and roughly one third of couples that wait to conceive until after the woman is 35 will experience fertility problems. While maternal age is not the only cause of infertility, it is the most common factor seen when a couple has difficulty conceiving. There are many medical options for treating infertility, including drugs to encourage ovulation, intrauterine insemination, surgery, or a class of procedures known collectively as assisted reproductive technology (ART). ART includes all fertility treatments in which both ova and sperm are manipulated in the laboratory, and primarily refers to in-vitro fertilization (IVF) and extensions of this procedure.Footnote 2
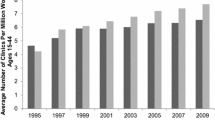
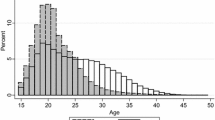
We use data from the 2002 National Survey of Family Growth to describe differences in the use of infertility treatments by age group. Figure 1 shows the fraction of women who sought fertility counseling by age group; this rate is clearly increasing with age. Figure 2 shows the use of various infertility treatments broken down by type of treatment and age group. Ovulation drugs are the most common type of treatment, followed by artificial insemination, surgery, and in-vitro fertilization (IVF). Less invasive and less expensive treatments, such as medications that induce ovulationFootnote 3 are the most common infertility treatment chosen for younger women (women aged 25 to 34). Infertile women older than 40 are more likely to be treated with artificial insemination and IVF. The use of surgery is higher among women who are older than 30.

The number of women receiving advice for infertility treatment increases with age

The number of women using infertility treatments increases with age. Notes: Data from the 2002 National Survey of Family Growth, weighted to represent US aggregate population
Infertility treatments are extremely expensive and generally not covered by health insurance (RESOLVE 2014). In 2006, Resolve.org quoted the American Society of Reproductive medicine in reporting the average cost of one IVF cycle to be $ 12,400 (2006 dollars).Footnote 4 Online cost calculators available from https://www.univfy.com/ and http://ivfcostcalculator.com/ estimate that the average cost for medication, pre-cycle procedures, and one cycle of IVF for a 35-year-old woman is approximately $19,000 to $ 20,000 (2014 dollars). Moreover, it often takes multiple cycles to achieve a pregnancy: the CDC reports that 22 % of all IVF cycles performed in 2009 resulted in a live birth, but this success rate differs widely with maternal age and health. As a result, in the absence of insurance coverage, it is realistic to expect out-of-pocket expenses close to $100,000 to achieve a healthy birth through IVF. The high cost of ART is the primary obstacle that keeps women with infertility from receiving this form of treatment. The total cost of infertility treatments also includes lost wages, travel and accommodation costs, medical testing costs, and cryogenic storage of embryos.Footnote 5
Currently, only 25 % of health care plans contain coverage for any form of fertility treatments and the extent of this coverage varies by state (William and Mercer Company 1997; Bitler and Schmidt 2012). Virtually all coverage of ART procedures only exists due to state-level legislation.Footnote 6 Although most health insurance companies do not cover ART as a matter of course, there are now 15 states which mandate that group health plans (generally employer-sponsored health plans) must include coverage for certain infertility treatments.
Hamilton and McManus (2012) and Bitler and Schmidt (2012) both demonstrate that IVF usage increased substantially as a result of the mandates to cover ART. This suggests that insurance companies are unlikely to cover ART treatments in the absence of such a mandate. These policy changes provide a unique source of exogenous variation in access to ART because they vary at the state and year level independently of individual women’s career choices. To date, only nine states (Arkansas, Connecticut, Hawaii, Illinois, Maryland, Massachusetts, Montana, New Jersey, and Rhode Island) have passed laws explicitly mandating coverage of IVF in employer health care plans.Footnote 7 New York, Ohio, and West Virginia have passed laws that mandate coverage of some fertility treatments but exclude IVF. Texas, California, and Louisiana have passed laws that only require insurers to offer such plans to employers; the employers still have the option to choose plans that do not include ART coverage. Table 1 summarizes the coverage and timing of laws passed in the relevant states. Our coding is based on information collected on the RESOLVE website and on the coding previously done by Bitler and Schmidt (2012).Footnote 8 We refer to the group of nine states with a mandate to cover ART as the “mandate states.” The three states requiring coverage of some fertility procedures but not IVF, and the three states mandating only that insurance companies offer such coverage are referred to as “weak mandate” states.
In our analysis, we focus on the impact of the mandates to cover infertility treatments that include IVF: that is, our treatment group is made up of the mandate states. Our control group comprises states that never passed any type of fertility coverage mandate. As in Buckles (2007), (2013), we completely exclude the weak mandate states from our main analysis of the mandates. Including these states as non-treatment states might compromise the control group and decrease the precision of the estimated treatment effect.Footnote 9
Previous studies show that the insurance mandates affect ART utilization and fertility outcomes among older women. In particular, Schmidt (2007) finds that the mandates increase first birth rates for older women. Machado and Sanz-de-Galdeano (2015) show that the infertility insurance mandates increase age at first birth without changing total completed fertility. Furthermore, these first order results are concentrated among older women belonging to a relatively high socioeconomic status (Bitler and Schmidt 2012; Buckles 2013).Footnote 10 Ohinata (2011) and Abramowitz (2012) find evidence that mandates delay the timing of the first child among white, highly educated women. The heterogeneous first-order effects of these mandates suggest that any impact on higher education should also be limited to a particular type of woman. In the context of this study, we expect the mandates to be relevant for the career decisions of college-educated women who were relatively young when a mandate was introduced. Importantly, Buckles (2007) finds that mandates increased participation in the labor force for women younger than 35 and decreased participation for those women older than 35. This suggests a reallocation of labor supply away from later in the life cycle to earlier in the life cycle resulting from delayed fertility breaks.
Since we posit that IVF coverage plays a significant role in women’s career investment decisions, it is logical to wonder how much detailed information young women have about their policy environment. Admittedly, hard data on young women’s specific knowledge of IVF mandates is difficult to come by. In evaluating the plausibility of mandates as a factor in human capital investment decisions, we consider the public understanding (or lack thereof) of fertility and the impact of this information on career decisions.
Firstly, there is anecdotal evidence that young women are increasingly conscious of the career-family tradeoff. A 2015 article in the New York Times cites a survey of Harvard Business School graduates that reveals this tradeoff (Miller 2015).Footnote 11 Not only did many of the women surveyed intentionally choose a job with greater flexibility, a significant fraction also turned down career advancement as a result of family considerations. Secondly, young women tend to have an excessive fear of suffering from infertility, possibly driven by a strongly held (mis)conception that their chances for childbearing will be drastically compromised by age 35 (Aleccia 2011, North 2012, Polis and Zabin 2012, Ryan 2011).Footnote 12 Finally, a study by Adashi et al. (2000) revealed that the vast majority of survey participants in the USA, UK, and Australia had some knowledge of IVF and viewed it as a dependable solution for infertility that should be a reimbursed medical expense. Hewlett (2002) also finds evidence that women are overly optimistic in both their expectations of IVF success and IVF availability. This is an important finding because in order for mandates to impact career choice, women need only believe that IVF will allow them greater flexibility in delaying fertility. Once this belief is in place, any increased awareness of IVF access can encourage women to invest more in professional career paths.
Beyond this type of explicit mechanism, there is another plausible pathway by which IVF mandates could influence women’s career choices. Given the pressure of the career family tradeoff, social norms that support delayed childbirth and dispel the notion of grim fertility odds after age 35 can logically play a huge role. IVF mandates can lead to such changes in social norms. As shown in Schmidt (2007), these mandates increase first births in highly educated, older women. Abramowitz (2012) further emphasizes that this effect is due in part to delayed first birth in states with a mandate to cover IVF. This process of shifting first-birth patterns for highly educated, older women in mandate states will influence social norms and expectations towards fertility. As it becomes more widely acceptable for young women to delay childbirth, they will be more likely to invest in professional degrees and careers. Although this trend should include all women, we would expect the change to occur the most rapidly in mandate states because these populations have the most exposure to changes in women’s fertility behavior.
3 Conceptual framework
In this section, we use a simple conceptual framework to explain how infertility insurance mandates may affect a woman’s decision to invest in a professional degree. This framework is inspired by a model of human capital formation (Becker 1975) combined with a model of the effect of motherhood timing on wages (Miller 2011).
Individuals invest in graduate education if the expected benefits of the education exceed the expected costs. Expected costs include the direct costs of a graduate degree—such as tuition and books—as well as the opportunity cost that is due to foregone earnings. Expected benefits are measured as the increase in lifetime earnings that results from obtaining the degree. Suppose that a woman can start working immediately after graduating from college (at age 22) or she can invest in a professional degree. Figure 3 depicts the shift in the age-wage profile that occurs with a graduate degree. The light gray line represents the age-wage profile of a person who enters the labor force directly after college and continues working for the duration of her career life. The dark gray line represents the profile of someone who invests in further schooling after college. We assume that wages increase with experience; this is reflected in the positive slope of both age-wage profiles. It is standard to also assume that the age-wage profile is concave: wages grow faster in the early phases of the career due to investment in training and positive but decreasing returns to experience. If a woman invests in a professional degree, her earnings are negative while she is in school. After graduation, her wages are higher than the wages of bachelor graduates of the same age and increase at a faster rate, reflecting intensive training and higher returns to experience.

Conceptual framework: costs and benefits of a professional degree
Using data from the NLSY79,Footnote 13 Miller (2011) shows that women experience a reduction in their wages after motherhood, which is consistent with a fixed cost of motherhood represented by a downward shift in the wage profile. She also finds that motherhood causes women’s returns to experience to decrease after motherhood, resulting in a flatter wage profile and diminished average earnings for the duration of the life cycle. Miller notes that the decline in returns to experience may be especially strong for women working in professional occupations because these occupations exhibit particularly steep earnings profiles early in the career (p. 1077). Accordingly, in this framework, we focus on the reduction in earnings caused by a decline in returns to experience.
A central implication of this model is that expected returns to investment in professional degrees are quite low for women who plan to have children. Figure 4 depicts the conceptual earnings penalty of fertility for professional women. A professional woman who never has a child and works continuously will remain on the solid dark gray path, and one who interrupts her career for a period of time will move onto a dotted path. The two dotted profiles illustrate the impact of an interruption early in the career (when the profile slope is very steep) versus an interruption later in the career (after the profile has flattened). Following Miller (2011), we assume that women may have up to one child and motherhood causes a career interruption that lasts for a fixed amount of time. During a career interruption, women earn no wages. Upon returning to work after a maternity interruption, women’s wages are lower than their pre-interruption wages: Miller refers to this drop as a “motherhood penalty.” Moreover, after returning to work, their wages grow at a slower rate than before, due to relatively lower returns to experience for mothers than for non-mothers.

Conceptual framework: returns to motherhood delay
As shown in Fig. 4, motherhood reduces the expected benefits of a professional degree through four channels: foregone wages during career interruption, reduced wages when returning to work, reduced experience and lower returns to experience. Since foregone wages increase with women’s age at motherhood, this channel predicts a greater fixed cost associated with interruptions later in the career. On the other hand, reduced wages when returning to work—possibly due to human capital depreciation—affect the remaining life-cycle trajectory of earnings and thus make early motherhood more costly in terms of lifetime earnings. Wage penalties resulting from career interruptions and lower returns to experience are decreasing in age at motherhood. As a result, these two channels are linked to a greater cost for interruptions that occur early in the career. Miller provides empirical evidence that the magnitude of these last two channels dominates the foregone wages effect. Delaying motherhood results in higher earnings over the course of the life cycle, documented in both increased wages and greater hours worked (Miller 2011). Further evidence of the earnings return to delayed motherhood is demonstrated by Leung et al. (2016), who find that Danish women with and without a college education significantly reduce their losses to lifetime earnings if they delay childbirth until after age 30. These results are also supported by Buckles (2007) findings that ART mandates increase wages for older women, suggesting that the ability to delay can meaningfully decrease the motherhood wage penalty.
Given the empirical evidence that a delayed interruption is significantly less costly to professional women than is an early interruption, we assume that women would tend to delay fertility if it were not for the biological constraints.Footnote 14 By allowing women to delay the birth of their first child, infertility insurance mandates raise the expected benefit of a graduate degree.
4 Data
In this section, we describe the dataset on women’s careers and present summary statistics for the main sample used in the empirical analysis. The primary data set comes from the nationally representative March Supplement of the 1977–2012 Current Population Survey (CPS).Footnote 15 The CPS contains information on women’s education and occupation as well as their demographic characteristics. Throughout the analysis, we restrict the sample to civilian women aged 35 to 64 with at least a college degree,Footnote 16 since only women with a college degree can apply for a professional degree program.Footnote 17 The age restrictions are intended to capture working-age women who are beyond college and who are likely to have already completed their professional degree had they decided to invest in one.Footnote 18 In fact, the majority of women who invest in professional degrees complete their degree by age 35 (Fig. 5).

Professional degrees by age. Notes: Data from 2000 Census. Sample: college educated women aged 22–64. Data are weighted to represent U.S. aggregate population
Using the Integrated Public Use Microdata Series (IPUMS) classification for occupations, we define a woman to be in a professional occupation if she is currently working or if she has worked in one of the following occupations in the past 5 years: attorney, judge, physician, dentist, or veterinarian (King et al. 2010). We select these occupations for three reasons. First, since professional degrees are lengthy and expensive, these occupations require a large and costly upfront investment in human capital. Goldin and Katz (2002), who studied the effect of early legal access to oral contraceptive pills on occupational upgrading by women, wrote that “the most relevant careers to study in the context of our framework are those that require extensive, up-front education, such as the professions of law, medicine, dentistry, and business administration” (page 748). Second, these occupations typically require working long hours, especially at the beginning of the career. Third, high earnings make career interruptions especially costly in these occupations. In sum, we chose occupations that satisfy three criteria: high up-front educational investment, long work schedule, and high earnings.
In order to correspond as closely as possible to our professional occupation definition, we identify professional degrees as JDs, LLS degrees, MDs, and DDS/DMDs.Footnote 19 From 1992 onward, the CPS data allow us to observe if a woman has completed a professional degree, although the particular field of degree is not explicitly stated. Prior to 1992, only the total years of post-secondary schooling is observable, but not the type of degree completed. Hence, within the CPS, we utilize only survey years 1992–2012 for the analysis of completed education. Since this limits the number of policy changes that we can observe in the CPS data, we additionally carry out our analysis in a combined dataset of Census and ACS samples, 1980–2011.
Panel A of Table 2 shows the descriptive statistics for the 1977–2012 sample from the March CPS, constructed with use of sampling weights.Footnote 20 The main sample used in the analysis includes mandate states (treatment group) and states that did not pass any mandates (control group). We refer to this sample as the “mandate sample”: columns 1 to 3 show the statistics for the mandate sample. For robustness, we also use a “weak mandate sample” which includes both the mandate states and the weak mandate states in the treatment group: columns 4 to 6 describe the weak mandate sample.Footnote 21 The mandate and weak mandate samples exhibit similar key characteristics.
Panel B of Table 2 represents only observations from the years 1992–2012, which is the CPS dataset used for the analysis of completed degrees. Again, the first three columns are for the mandate sample, and the next three are for the weak mandate sample. As in panel A, descriptive statistics for the mandate sample and weak mandate sample are comparable.
Conditional upon college completion, approximately 3.8 % of American women have a professional degree, and 3.3 % have a doctoral degree. 2.2 % of college-educated women report working in a professional occupation. Given the small fraction of women who complete a professional degree or work in a professional occupation, even a modest effect of a mandate to cover IVF would be meaningful. The sample size for the occupational choice analysis is 196,489 and includes survey data from 1977 to 2012. The sample for analysis of educational choice contains 128,044 women, and spans 1992 to 2012.Footnote 22 Roughly 84 % of our sample is white, 89 % have been married at least once, and the mean age at the time of survey is 46.8 years.
There is a difference in the rate of treatment for the occupation sample (panel A) and the degree sample (panel B). 9.6 % of the occupation sample were treated with a mandate to cover by age 35. Due to the data restrictions mentioned above, only 1.2 % of the CPS degree sample were treated by age 35.Footnote 23 As an alternative to the degree sample in panel B, we also analyze women’s education outcomes using a combination of US Census and the American Community Survey (ACS) samples: these data are summarized in panel C and reflect a treatment rate of 9.8 %. In terms of race and age characteristics, the Census/ACS sample is very similar to CPS samples. However, the professional degree rate is slightly higher in the Census/ACS than in the CPS. This is due in part to a difference of definition, which is described in detail in Section 6.
5 Empirical strategy
Our empirical specification is a triple difference equation, where the outcome of interest is the probability that a woman is a professional. The treatment effect is measured by the triple difference coefficient: the interaction of the treatment group indicator, the post-mandate period indicator, and the relevant cohort indicator. This section explains the details of our strategy.
5.1 Identification of the treatment effect
One option for estimating policy treatment effects is a difference-in-differences strategy that compares outcomes of women across states and years. However, for this estimation strategy to be valid, the outcomes of interest in mandate and non-mandate states should exhibit parallel trends prior to the enactment of the mandates. Figure 6 displays the weighted average of the fraction of women in professional occupations in states with a mandate to cover ART and in control states: years are normalized such that year zero reflects the period in which a mandate was passed. The broadest normalized timeline available for all mandate events is t=-8 to t = +7.Footnote 24 The graph shows an increase in the rate of women in professional occupations that begins several years after the mandate was passed (t=4). The rate keeps increasing in the subsequent years. This is consistent with an effect of the mandate as it takes at least 4 years for women to apply to graduate school, enroll, and graduate with a professional degree. However, there is also evidence of a smaller increase in women working in professional careers at the time of the mandate (year zero). This increase cannot be due to the laws as it takes some time for changes in women’s investment behavior to be reflected by changes in degrees. One plausible source of the year zero effect is increased migration of professional women into states with ART coverage. In Section 6.1, we examine the migration effect of the mandate further.

Increase in the rate of professional careers. Notes: Share of college-educated women aged 35–64 working in a professional occupation. Data from the March Supplement of the Current Population Survey, 1977–2012
A central concern for identification purposes is the possibility that states that passed an ART coverage mandate and states that did not pass such a law were following different trends before the legislation. In particular, the treatment states’ trend is generally more erratic, especially prior to t=-5. If it is the case that the treatment and control groups do not exhibit parallel trends prior to the mandate period, then in using a difference-in-differences analysis one could wrongly interpret differences in pre-existing trends as a causal effect of the law.Footnote 25
To overcome this concern, we estimate the effect of mandates to cover infertility treatments using a triple difference specification (DDD). Since the mandates should only affect career choices of women who are relatively young when the laws are enacted, we can exploit the inter-cohort variation to identify the causal effect of the mandates. We can estimate the impact of insurance mandates by comparing the outcomes of women across states, calendar years, and birth cohorts.Footnote 26 Specifically, women who were older than 35 when the mandate was passed are used as a within-state control group.Footnote 27 We assume that most women over the age of 35 will not be facing the decision of whether or not to invest in a professional degree or career (recall Fig. 5). Importantly, we observe the occupations and education of women in the CPS even if they are not currently in the labor force.Footnote 28
The choice of age 35 as the investment decision cutoff point is approximate and may be considered to be somewhat subjective. According to the National Survey of College Graduates (2003 and 2010 waves), 50 % of women with a professional degree had completed their schooling by age 27, 75 % had completed by age 32, and 90 % had completed by age 39. The mean age at graduation was 29.Footnote 29 Data from the 2000 Census are shown in Fig. 5 and corroborate these statistics, showing that the share of college-educated women between ages 22 and 64 rises steeply between ages 24 and 30, then increases from 7 to 7.9 % between ages 30 and 35, but only rises by about one percentage point further between ages 35 and 64 (these data cannot account separately for cohort effects). While age 35 seems to be a reasonable choice for the point at which the majority of women have completed their career investment decisions, this point varies considerably from individual to individual. In order to investigate the sensitivity of our results to the choice of age cutoff, we also use age 30 as the cutoff as a robustness check (discussed in Section 7).
5.2 Endogeneity and omitted variable bias
The triple difference specification is still susceptible to potential sources of estimation bias. First and foremost, there may be a concern that states’ decisions to pass a mandate are a function of state-level economic and cultural characteristics that are correlated with women’s career decisions. For example, a state that has a high proportion of women working as attorneys and physicians might subsequently have a greater propensity to pass an ART coverage mandate. Buckles (2007) argues that the mandates were not the result of lobbying efforts by professional women who wanted to delay fertility. To explore this issue further, we use data from the 1980 Census—since West Virginia is excluded, 1980 is prior to the passage of any mandates.
Table 3 shows the difference in means for a set of state-level characteristics between the treatment group and the control group in 1980.Footnote 30 The treatment and control groups display statistically different means for completed fertility and percentage working in agriculture: women in the treatment states have 0.2 fewer children than women in the control states, and a lower fraction of the population is employed in agriculture in treatment states compared to control states. However, the majority of measurable state-level characteristics do not vary significantly between mandate and non-mandate states. In general, these two groups are not obviously differentiated.
Additionally, we test whether state-level characteristics observed before the mandates can predict the policy changes using multivariate regression analysis. We regress the probability that a state passed a mandate to cover on various state-level indicators obtained from the 1980 Census. We find that lower completed fertility and older age at first marriage of women aged 35 to 44 are correlated with passing a mandate to cover. The results are reported in the Appendix (Table 9). In light of these two factors, we always include state fixed effects to control for unobservable, time-invariant, state-level factors that might affect completed fertility as well as a woman’s choice to invest in professional degrees.
In addition to state-level confounding factors, our sample covers a time period during which women’s rates of both professional occupations and professional degrees were increasing strongly at the national level (see Goldin and Katz (2002)). In order to ensure that we are identifying the change in occupational choice due specifically to the mandate changes rather than underlying national or cohort level trends, it is necessary to control for national events that affected all women (survey year dummies), cohort level trends common to all states (birth year dummies), or national events that affected specific age groups (year-cohort interaction effects). The interactions between year fixed effects and cohort fixed effects account for time-varying omitted factors such as national policy changes with effects that vary across women depending on their age. In other words, these year-cohort interactions separately identify shifts in occupational choice differentials between young and old women that are not specific to particular states. Finally, we are particularly concerned about policy or cultural changes that raised rates of professionals among younger women in the 1970s and had a larger effect within states that eventually passed an infertility insurance mandate in the 1980s and 1990s. Such omitted factors would confound our results and bias our estimated treatment effect upward. To account for these factors we include interactions of a mandate state indicator and the birth year cohorts.
5.3 Specification
We consider an individual woman to be treated if her state of residence enacts legislation mandating ART coverage by the time she turns 35. Although age 35 also coincides with the age at which fertility starts to decline dramatically, our focus is on the timing of the investment decision rather than the timing of fertility. We estimate the following regression using a linear probability model:
EverMandate s is equal to 1 if state s enacted a law requiring ART at any time during the span of our dataset. PostMandate s t takes value 1 if the survey year is at least 4 years after the mandate year in a mandate state, and defined as 0 for all years for all control states. 35orYoungerMandate s k is equal to 1 if cohort k in state s experienced a mandate by the time they turned 35; it is defined as 0 for all cohorts older than 35 at the time of a mandate and for all cohorts living in a control state. d s is a vector of state fixed effects that account for time-invariant unobservable factors at the state level. t t denotes year fixed effects that control for macroeconomic conditions or changes in federal law that are common to all states. ? k represents cohort fixed effects that account for time-invariant factors that affect all women born in the same year. EverMandate s ×? k is an interaction of EverMandate s and cohort fixed effects. This interaction term controls for the cohort-specific changes within states that passed a mandate to cover infertility treatments, that is, any state-specific omitted factors that impacted the occupational choices of young and old women in a different way.
\({\sum }_{kt}\mu _{kt}\) are cohort-year fixed effects that control for any time-varying policy or shocks that have differential effects on women by birth year.Footnote 31
We also control for individual race, age (at survey year), and marital status characteristics: although these characteristics are unlikely to be correlated with the presence of a mandate, they are certainly correlated with the outcomes of interest and including them improves the efficiency of the estimation.Footnote 32 Finally, to address the concern that the mandates may be endogenous, we include state-specific linear time trends: \(({\sum }_{s}\delta _{s}\times t)\).Footnote 33 Throughout our analysis, we cluster the standard errors at the state level to account for within group serial correlation in the error terms (Bertrand et al. 2004).
ß 4 measures the DDD effect of the mandates on relative outcomes for women 35 or younger at the time of the mandate, before and after the mandates were enacted, in states that passed the mandates compared to control states. The identifying assumption requires that, in the absence of the mandate, differences in outcomes between older women and younger women would have evolved similarly in states that passed a mandate and states that did not pass a mandate (Gruber 1994). Although this assumption is virtually untestable, we can attempt to verify it indirectly by comparing pre-policy trends in treatment and control states. Figure 7 and 8 show the cohort group differences in professional occupations for the treatment and control states, respectively. In Fig. 6, the relatively young cohort is so defined as all women in a mandate state who were 35 or younger at the time the mandate was enacted, and the relatively older cohort comprises women aged 36 or older in the mandate year. Before the policy (represented as the period for which t<0), the difference in outcomes between young and old cohorts is broadly constant over time in both treatment and control states, especially starting from t=-5. In both treatment and controls states, outcomes for the young cohort group are noisier relative to the old cohort group before t=-5, possibly due to the small number of observations. Starting in t=-5, the discrepancy in outcomes between young and old cohorts differs in level but stays constant over time in treatment and control states, supporting the hypothesis of parallel trends. The divergence between old and young that begins at t=4 is much more distinct than any divergence among the old and young cohorts in control states, as depicted in Fig. 7.Footnote 34 The difference in divergence between Fig. 7 and 8 is exactly the treatment effect we estimate in Eq. 1.

Increase in professional careers: treated states by cohort group. Notes: Share of college-educated women aged 35–64 working in a professional occupation. Data from the March Supplement of the Current Population Survey, 1977–2012. Residents of ART mandate states only. Young cohort comprised of women living in a mandate state who were 35 or younger at the passage of a mandate. Old cohort members were already 36 or older at the time of mandate

Increase in professional careers: control states by cohort group. Notes: Share of college-educated women aged 35–64 who are working in a professional occupation. Data from the March Supplement of the Current Population Survey, 1977–2012. Residents of the control group states only. Young cohort defined as women who were 35 or younger in 1995 (midpoint year of mandates in the treatment states). Old cohort members were 36 or older in 1995
6 Results
Table 4 displays the results of the analysis pertaining to the mandate to cover treatment effect on the probability that a woman works in a professional occupation. In Column 1, the variable (EverMandate)X(PostMandate) is the interaction of the treatment group indicator (EverMandate) and a binary variable (PostMandate) that equals one when the woman is observed after the legislation has been enacted in her state. This specification is the difference in differences result across states and time. The mandates increased professional occupation rates among women in treatment states by 0.5 percentage points more than professional rates increased within control states during the sample period.
In columns 2 through 4, we examine the triple difference effect in order to account for the variation across state, time, and birth cohorts simultaneously. The treatment should only affect women who are relatively young at the time of the mandate. Hence, we look at variation between birth cohorts who were 35 or younger at the time of the mandate and those birth cohorts who were already at least 36 years old. The triple difference effect is the coefficient on the variable (EverMandate)X(PostMandate)X(35orYounger). The estimated triple difference effect in column 2 is 0.010 and significant at the 1 % level. The effect is robust to the inclusion of a full set of fixed effects: state, survey year, birth cohort, and the interactions (Cohort)X(Survey Year) and (Cohort)X(Ever Mandate).
In column 3, we add demographic controls for race and marital status to the regression model used in column 2. The inclusion of these additional factors does not change the coefficient of interest. This strengthens the result in column 2, as it implies no correlation between treatment and individual level demographic characteristics beyond the state, year, and cohort level trends. The signs of the demographic controls are as expected. There is a significant and negative sign on the Black indicator and a positive sign for Other Race—primarily due to the greater tendency of Asian Americans to work in professional occupations. Ever Married is negative and significant, which is consistent with the fact that never married women are more attached to the labor force than married women, and tend to have greater levels of human capital. As an additional control, in column 4, we examine the impact of state-specific linear time trends: including state time trend controls increases the estimated treatment effect slightly to 0.012 (still significant at the 1 % level). All together, these findings are consistent with our hypothesis that the mandates to cover infertility treatments appreciably increase the probability that women enter a professional occupation.
The estimated coefficient of 0.010 to 0.012 implies that introduction of a mandate to cover ART increases the probability of being in a professional occupation by 1 to 1.2 percentage points.Footnote 35 Within the context of only 2.1 % of women in the sample working in a professional occupation for the whole sample, this effect is equal to approximately one half of the sample mean. Alternatively, we can interpret the coefficient through its contribution to the change in outcomes in the treatment group over time. Given that womens professional occupation rate in mandate states increased by 1.4 percentage points between 1985 and 2012, and that the share of women in our sample exposed to a mandate increased to 11.9 %, the ART mandates account for roughly 10 % of the increase in professional occupations among women in mandate states during this time period.Footnote 36
As a point of comparison, Goldin and Katz (2002) found that early legal access (ELA) to oral contraceptives contributed to 94% of the overall increase in women’s professional occupation rate between 1970 and 1990.Footnote 37 The dramatically large contribution of ELA underscores our argument that woman are more likely to invest heavily in professional careers when they are confident in their ability to delay fertility.
A second important empirical benchmark comes from Buckles (2007). Buckles finds an overall increase in participation rates of approximately 10 % for 29-year-old women as a direct result of IVF mandates, and a similarly sized decrease in participation rate of 39-year-old women. These results suggest a reallocation of labor supply in about 10 % of working women. Moreover, the effect is larger for women with a college degree. Our estimate that 10 % of the observed change in professional career choice can be attributed to IVF mandates appears quite consistent with Buckles’ conclusion.
Our second outcome of interest is completed education. We apply the triple difference model to examine the effect of the mandates to cover ART on the probability that a woman completes a professional degree. The results from the CPS sample are displayed in Table 5: column 1 shows the difference in differences across states and time, columns 2–3 show the triple difference effect with and without demographic controls, and column 4 additionally controls for state-specific linear time trends.
As with the occupation analysis, we see that the most meaningful variation in the outcome is due to variation across three dimensions—state, year, and cohort—rather than simply across states and time. This underlines the critical difference in the treatment of women who still face a human capital investment decision and those who are past the investment period of their lives. The state-time variation in column 1 is positive but insignificant (0.003). However, we do observe a positive and significant triple difference effect across treatment groups, survey years, and age cohorts. The triple difference specification is presented in columns 2–4, and all of these specifications include the pairwise interactions of (CohortXYear) and (CohortXEverMandate), as well as state, survey year, and birth cohort fixed effects. The triple difference treatment effect is robust to the inclusion of demographic controls (column 3) and state level linear time trends (columns 4).Footnote 38 In column 3, the effect of the mandate is 0.021 and significant at the 5 % level; the coefficient in column 4 is very similar. At face value, this parameter indicates that the difference in professional degree completion between relatively young cohorts and relatively older cohorts is 2.1 percentage points wider in the treated states than in the control states.
The large and significant effect of the mandate in Table 5 must be interpreted with caution. Because data on professional degrees are not available in the CPS before 1992, the identification of the treatment effect on professional degrees using CPS data relies only on two states that passed a mandate to cover after 1992 (New Jersey and Connecticut). Given these extreme limitations of the CPS education data, we use supplemental data from the decennial US Census and the American Community Survey (ACS) to examine the impact of the mandates on degree outcomes. We combine the 5 % public use samples from 1980, 1990, and 2000 Censuses and the 2010 ACS.Footnote 39 For comparability with the CPS results, the Census/ACS sample is also made up of all college-educated women aged 35 to 64 at the time of the survey for whom we can observe a three-digit occupation code (this is conditional on having worked in the past 5 years). Despite the lack of yearly observations, the Census/ACS data adds considerable value to the analysis because of the increased sample size and the ability to measure education data starting in 1980. Consequently, the treatment group includes all eight states that passed a mandate to cover between 1980 and 2000 (excluding Montana). The drawback to the Census is the fact that education data from 1980 is not completely comparable with the more recent years. We can identify professional degrees and doctoral degrees in the 1990 and 2000 Census and in the ACS samples, but the education information for the 1980 sample is less detailed. In 1980, post-secondary education is specified only as the number of years of college completed by the individual. Hence, within the 1980 Census sample, we use an outcome that combines professional degrees and doctoral degrees, defined as having completed at least 7 years of college. While this is not ideal, the alternative is to forgo the 1980 sample from the analysis. Given that five states enacted a mandate to cover IVF between 1980 and 1990, the advantage of including this pre-treatment time period outweighs the disadvantage of an imperfect definition for professional degree.
The Census/ACS results for education are displayed in Table 6. A mandate has a positive and significant effect on the probability of obtaining a professional degree in the Census sample, although the magnitude of the effect (0.8 percentage points) is smaller than the analogous result in the CPS sample (2.1 percentage points). The magnitude of this effect is similar with or without state-specific linear time trends.Footnote 40 This coefficient implies that if a mandate to cover IVF raises the probability of completing a professional degree by 0.8 percentage points, this is a 13 % increase for the given sample mean of 0.065.
Within mandate states, we can compare the coefficient 0.008 to the observed increase in the professional degree rate from 1990 to 2000. This rate cannot be directly compared to the professional degree rate in the 1980 Census, or the rate measured in the ACS data, due to differences in sampling weight methodology over ACS samples.Footnote 41 During the 1990s, the strong mandate treatment rate increased by 8.7 percentage points (going from 0.015 to 0.102), and the rate of professional degrees among women in treatment states increased from .059 in 1990 to .064 in 2000 (change of 0.005 over the decade). Given an estimated mandate treatment effect, the increase in mandates over this period predicts a change in professional degrees of 0.087×0.008=0.0007, approximately 15 % of the observed increase in professional degree rate. Again, when compared to the findings in the Buckles (2007) paper, a predicted effect of the mandates on professional degree choice of 15 % of observed change is quite consistent.
Taken as a whole, these results do provide evidence that legislation which mandates that group health insurance plans cover ART (specifically, IVF procedures) has a significant impact on the human capital stock of women within a mandate state. Passage of such a mandate increases both the likelihood that female residents of the state have a professional degree and that they work in professional careers. This treatment effect is observed specifically in women who were relatively young at the time of legislation, suggesting that women are forward looking in their human capital investments and are meaningfully influenced by fertility-related costs. These findings are consistent with a conceptual framework that predicts that the ability to reallocate fertility from early in the life cycle to later in the life cycle increases the benefits to women of pursuing a professional career. There are two distinct channels through which this may occur. Firstly, young women may become more likely to pursue a career in law or medicine when their state of residence mandates ART coverage. A second possibility is that women from other states who have already completed a professional degree decide to move into a mandate state to optimize their career trajectory. Either of these channels may be viewed as an investment decision by young women, and the migration decision is examined more closely in Section 6.1.
In Table 7, we consider the difference in the effect of a mandate to cover ART and simply a mandate to offer plans that include ART coverage. We use the CPS dataset for occupation (columns 1–3), and both the CPS dataset (columns 4–6) and the Census/ACS dataset (columns 7–9) for education. We expand the set of states in the treatment group to include states that passed a mandate to offer insurance for infertility treatments. The effect of a mandate to cover is estimated as the triple difference effect (EverMandate)X(PostMandate)X(35orYoungerMandate), while the effect of the weaker laws are measured as the triple difference effect (EverWeakMandate)X(PostWeakMandate)X(35orYoungerWeakMandate) (recall that states that passed a mandate to cover or a mandate to offer are referred to collectively as the weak mandate treatment group). Pooled regression of professional occupation on both types of treatment yields results that show the strong mandate effect is significantly larger than that of a weak mandate (testing for equality between the two coefficients produces a p value less than 0.01). The same result holds for the effect of the mandates on professional degree. In fact, the weak mandate has a negative effect on investment in professional education in columns 5 and 6.
In terms of the coefficient on (EverMandate)X(PostMandate) and (EverWeakMandate)X(PostWeakMandate), these parameters can be interpreted as the difference in difference coefficients of the control group in each respective regression (women older than age 35 in the relevant treatment states). In both columns 6 and 9 of Table 7, we see a positive and significant DD coefficient on weak mandates, but not on mandates to cover. Importantly, since a difference in differences specification does not identify the treatment effect of the mandates, these DD coefficients may not be considered a treatment effect of the mandates in this context. Rather, they imply a steeper average increase in professional degree rates for women in weak mandate states compared to mandate states, but should not be interpreted as any causal effect of the weak mandates. To confirm a difference in differences specification is not valid, we use 1970 and 1980 Census data to show that the parallel trends assumption for difference in differences is not satisfied for weak mandates.Footnote 42
6.1 Migration as a potential mechanism
One plausible component of the positive effect of the mandates is an inflow of professional women from non-mandate states. Ideally, we would be able to observe a woman’s state of residence at the time she undertakes her career investment decision, in her early 20s or immediately following college graduation. Unfortunately, this data is not available, and we use state of residence at the time of an individual’s survey instead. As an alternative—but still imperfect—proxy for a woman’s state at the time of college completion, we consider the mandate status of each woman’s birth state and use this to define treatment. The CPS does not contain information on an individual’s birth state. To investigate the potential role of migration, we use the Census/ACS dataset that we employed for our main degree outcome results (Table 6). These data are summarized in Table 2, panel C. As discussed previously, in spite of the birth state advantage, the Census data is limited both by its decennial frequency and its inconsistent definition of degree outcomes. Although we consider the CPS spot estimates for the mandate effect on occupation (found in Table 4) to be superior to the estimates from the Census/ACS, the latter can still be informative about the role of migration in driving the mandate effect.
In evaluating the role of migration, we first compare the effect of a mandate in a woman’s state of birth with the effect based on state of residence. Secondly, we test whether excluding foreign-born women alters the results. We hypothesize that foreign-born professional women may be more inclined to migrate from one state to another than native-born professionals, because they already demonstrated a willingness to relocate from another country. If migration is a substantial channel for the mandate effect, restricting the sample to only native-born women should reduce the estimated effect. Panels A and B of Table 8 display the key parameter estimates for the mandate effects on professional occupation and professional degree, respectively. The explanatory variable of interest remains our triple difference indicator, which takes the value of 1 if a mandate to cover IVF was passed by the time the woman turned 35. The specification controls for state fixed effects, cohort fixed effects, demographic controls, and state-specific cohort trends (linear and quadratic). In column 1, treatment is assigned based on state of residence at the time of the survey and the sample includes both native-born and foreign-born women. In column 2, treatment is still assigned based on state of residence but the sample excludes foreign-born women. In column 3, treatment is assigned based on state of birth, necessarily excluding foreign-born women.
For professional occupations, the results in panel A fail to show a significant impact of the mandate for either a treatment by state of residency or treatment by state of birth. However, the spot estimate based on state of residence in columns 1 and 2 is 0.003, which is larger than the vanishingly small state of birth treatment effect found in column 3.Footnote 43 Notably, removing foreign-born women has no discernible effect on the mandate coefficient.
In panel B, the impact of a mandate to cover ART is positive and statistically significant for professional degrees when state of residence is used to determine treatment, but smaller and insignificant when the treatment is assigned by state of birth. This lack of a significant result when birth state is substituted for residence state suggests that the mandate effect is driven in part by emigration of women with professional degrees already in hand. However, as in panel A, there is no difference in the results with or without foreign-born women. In these results, the contrast between birth state mandates and residence state mandates offers some support for a migration mechanism, but this support is not found in the difference between the full sample and the native-born only sample.
Analysis using the CPS supports the hypothesis that migration may be partially driving the results, but it likely is not the only operating channel. In the CPS, we focus on recent internal migration, and these results can be found in the Appendix. Columns 1 and 2 of Table 10 in the Appendix report estimates for the determinants of being a “recent migrants.” Recent migrants are defined as women who were living outside the state 1 year before the survey.Footnote 44 We apply both the difference in differences and triple difference specifications to estimate the effect of the mandates on the state’s proportion of new migrants. The mandates are associated with increased rates of new migrants in the population, and the effect is largest for women who were 35 or younger at the time of the mandates. The cohort effects are relevant in the migration channel as well as in the education channel, since younger women will have a longer time horizon in which to reap the benefits of a migration decision.
However, dropping new migrants from the sample does not dampen our main results. For comparison, columns 3 and 5 report the main result (DDD) for occupational and educational outcomes using the survey years in which the migration variable is available. The estimates are very similar to those in Tables 4 and 5. In columns 4 and 6, we drop new migrants. The point estimate increases and remains significant when migrants are excluded, suggesting that both migration and career choice are channels through which a mandate to cover ART increases the number of female professionals in a state.
7 Robustness checks
7.1 Inference
The triple differences empirical strategy exploits changes in insurance coverage enacted by eight states (strong mandate) or 13 states (weak mandates). However, when we analyze the effect of a mandate to cover IVF on professional degrees using CPS data, the number of groups for which the policy changes is reduced to two (New Jersey in 2001 and Connecticut in 2005). Conley and Taber (2011) argue that inference based on clustering at the state level is incorrect when the number of states affected by the policy change is small and the number of time periods is fixed. They show that, under this circumstance, the difference in differences estimator is unbiased but inconsistent, and propose a new method to construct confidence intervals using information from the control states.
In results not reported, we experimented with confidence intervals based on Conley and Taber (2011) for a difference in difference specification across states and cohorts using post-mandate ACS data. The confidence intervals consistently include zero even when the clustered standard errors indicate statistical significance, suggesting that the results should be interpreted with caution. However, inconsistency may not be a great concern in our triple difference strategy because of the relatively high number of time periods and cohorts under study. Reassuringly, replication within the US Census, which is based on a larger number of treatment states, provides smaller yet statistically significant estimates for the analysis of professional degrees.
7.2 Refined control group
In order to improve the comparability of the treatment group’s outcomes with the outcomes of the control group, we refine the control group for each policy change by utilizing the synth programming package developed by Abadie et al. (2010). The synth program generates a synthetic control group that is a weighted average of all non-treatment states during the treatment time period. The weights are chosen to match observable characteristics of the treatment group during the relevant period. We use the synthetic control group vector of weights to determine which states are the least similar to each of our treatment states—these states are dropped from the control group.Footnote 45 The regression results using the refined control group are shown in Table 13 in the ?? Appendix. Refining the control group increases the magnitude and precision of the mandate effect for professional occupation: these results also indicate that the mandate to cover ART will increase the probability that relatively young women will invest in a professional career. For professional degree, the coefficients are similar in magnitude but imprecisely estimated.
7.3 Placebo tests
We also conduct various placebo tests on our results, both with respect to the outcome that we defined and the timing of the mandates. In our primary analysis, we focus on a very narrow group of occupations which are known for intense investment during a worker’s early career. If the effect of the mandates on career choice is not due to the impact on the investment decision, testing the result of the mandates on groups of occupation that are less investment intense early in the life cycle should reveal little or no influence of the policy changes. We test a broad range of occupation categories that require at least a college degree, within the same CPS sample as our original results.
Table 14 in the appendix reports DDD coefficients from Eq. 1 on various alternative outcomes. The table lists the 13 categories that we consider as placebo outcomes, as well as our outcome of interests for comparison.Footnote 46 The only categories that experience a positive and significant effect apart from our outcome of interest are the two subcategories that make up our category “Professional Occupations.” The effect of the mandate on physicians is positive and significant (0.004*), as is the effect for lawyers and judges (0.008***). It is notable that the impact for “other health professionals,” a group that includes RNs, pharmacists, nutritionists, therapists, and physician assistants, is significantly negative, and quite large in magnitude (-0.016**). Although we do not have sufficient data to conclude anything definitive, these results are consistent with a mechanism that changes the outcome for marginal women away from a career in the “other health professionals” category (traditionally dominated by pink collar occupations that require relatively highly skilled workers) and into a professional career in law or medicine.Footnote 47
We also control for the 5-year period prior to treatment to test for endogeneity, and do not find significant evidence of endogeneity. In addition, we conduct a placebo test in which we assign false mandate events among the control states and use the true mandate states as the control group (ignoring the actual mandates).There is virtually zero effect of these false mandates.
As a test of mandate timing, we also construct false mandate variables that set each of the legislation years 3 years before the true year of enactment; since the law is not yet enacted, we would not expect these placebo mandates to exhibit the same treatment effect. However, because the treatment group in the placebo mandate will contain some of the women influenced by the true mandates, a muted estimated effect of this placebo is reasonable. Since this analysis requires yearly data, we run this analysis using CPS data for both occupational and educational outcomes. Of course, the disadvantage in using the CPS data is the fact that they only contain two mandate events. The placebo coefficients were insignificant for professional occupation and significant but greatly reduced in magnitude for professional degree.
Finally, we exclude each of the mandate states from the sample individually to determine if our results are driven by any one state in particular. The triple difference coefficients for both occupation and degree remain statistically significant, and the magnitudes are not altered by dropping any specific mandate state from the sample. All of the placebo test results described above are available upon request.
7.4 Alternative age cutoff for treatment
To test the robustness of our results, we alternatively define women as treated if there was a mandate in their state of residence by the time they turned 30. When using this definition of treatment, we exclude women who were aged 31 to 35 when a mandate was passed. This group could be affected by the mandate and thus does not belong to the control group.Footnote 48 Columns 1–4 in Table 11 in the appendix display the results. For professional occupation, the results are similar to those presented in Table 4 in terms of magnitude and significance; for professional degree, the coefficient is double in magnitude relative to Table 5 but it is imprecisely estimated.
7.5 Effect of mandates on men
As an alternative placebo check, we perform a falsification test using men as an additional control group. Men’s decisions to invest in human capital and migration could also be indirectly affected by the mandates through the marriage market and capital formation. However, we expect this effect to be smaller than the impact of mandates on women. Columns 5–8 in Table 11 in the appendix show that the mandates had no significant effect on the number of male professionals in the state.
7.6 Differential effects by race
Because education and occupation profiles differ dramatically by race, we consider whether the mandates have a heterogenous impact by race. We address this question by separating our sample into white women, black women, and women of other races; results are presented in Table 12 in the appendix. The effects on professional occupation (based on CPS data) are consistent with the rest of the literature: the positive mandate effect that we observed in the pooled sample is clearly driven by white women; the coefficient for the white sample is 0.015 and significant at the 1 % level. In contrast, the effect on occupations is zero for black women and negative (though insignificant) for women of other races. However, the set of results for professional degrees (based on the pooled Census-ACS sample) provide a different picture of the mandate treatment heterogeneity. The coefficients are positive and statistically significant for both white and black women, and they are positive, extremely large, and marginally significant for women of other races.Footnote 49 These results intimate that while IVF mandates may have comparable results across races for education, this does not appear to be a significant factor in propelling non-white women into professional occupations. However, although growth in women’s overall rate of professional degrees has stagnated, the IVF mandates may be meaningfully increasing the rates among minority women.
7.7 Family background and wealth
We also consider the importance of family background in determining both education and occupation outcomes. Ideally, we would control for parental wealth; however, this information is not observable in the CPS. For a subset of our sample, we can observe various forms of non-wage income. In particular, we consider the importance of interest, dividend, and rental income. The sum of these variables serves as a reasonably good proxy for wealth, and intergenerational asset wealth tends to be highly correlated. Again, we find that including a control for non-wage income does not meaningfully change the mandate effect for either occupation or degree: results are shown in the Appendix (Table 15).
8 Conclusion
In this paper, we measure the impact on women’s occupational choice of access to assisted reproductive technology, measured as an exogenous cost reduction due to state level mandates for health insurance plans. The empirical findings show evidence that mandates to cover IVF and other ART treatments do increase the number of women with a professional degree or working in a professional occupation. In contrast, the mandates that only require insurance companies to offer ART coverage plans, but lack universal coverage among group sponsored plans, do not have a significant effect on the number of female professionals in the state. This is consistent with our expectation that lack of universal coverage for high-cost procedures does not allow for sufficient risk sharing to reduce costs for individuals. Our results are robust to the inclusion of state-specific time trends, key robustness checks, and are replicable to a reasonable degree in both the CPS and the Census/ACS.
The analysis presented in this paper suggest that policies that help women to push back motherhood until later in their careers may help increase women’s participation in professional occupations. Recently, a number of high-tech companies started offering fertility preservation to their employees (Miller 2014).Footnote 50 Our study suggests that these type of benefits could increase women’s investment in highly skilled professional occupations.
The analysis has some limitations. First, because of the lack of information on women’s migration history, we cannot fully distinguish between the human capital and migration channels, but can only evaluate the total effect of both mechanisms. Secondly, due to a relatively small number of policy events, we cannot currently investigate whether the mandate effects are heterogenous by state characteristics; this may be an interesting area for future research if more states pass ART coverage mandates in the coming years. Finally, although the replication within Census and ACS data confirms the results obtained using CPS, these data do not show the year to year changes in professional degrees. Therefore, the findings on degrees should be interpreted with caution. Nevertheless, this study presents the most precise estimate of the impact of ART on women’s labor market choices that is currently available.
In particular, it is possible that the ability to delay fertility can encourage highly capable women to substitute away from traditionally pink collar careers in nursing, professional therapist jobs, and physician assistant jobs, and into the male-dominated occupations in law and medicine. We provide evidence that indicates this may be the case and believe that this is an important avenue for future research. We also show how the results may be partially driven by migration, as women with a professional degree might choose to live in states that passed a mandate. This is an important mechanism because it implies that offering coverage for infertility treatments could be an effective policy for states interested in increasing the stock of human capital.
Notes
For example, women received only 5 % of law degrees conferred in the USA in 1970, but 47 % of new law degrees in 2010. (National Center for Education Statistics 2011)
Other types of medical treatment included in ART are gamete intrafallopian transfer (GIFT), zygote intrafallopian transfer (ZIFT), embryo cryopreservation, egg or embryo donation, and gestational carriers (http://www.resolve.org/family-building-options/ivf-art/).
For example: Clomid.
http://www.resolve.org/family-building-options/insurance_coverage/the-costs-of-infertility-treatment.html. This figure does not appear to include the costs of ovulation medication and pre-cycle procedures.
Resolve provides information about individual state specifications for insurance coverage for ART procedures, stating also that “Since most assisted reproductive technologies (ART) are not covered by insurance, the patient has to pay ‘out-of-pocket,’ often leading to increased stress as well as long-term financial burdens.” On the insurance coverage page at Resolve.org, infertile couples are told, “If the state you live in is not in the above list, there is no law in your state requiring insurance coverage for infertility treatment. Contact your local representative and ask them to introduce legislation to require infertility treatment coverage.” The website provides a link to www.contactingthecongress.org. In the absence of a mandate, there is no incentive for most for-profit insurance companies to cover ART procedures. A few firms now reimburse employees for egg freezing (and possibly ART) as an in-kind benefit, but this is not through insurance.
Montana passed an ART coverage mandate in 1987; However, as noted in Hamilton and McManus (2012) there were no fertility clinics in the state during our study period. For this reason, we removed Montana from our study completely.
Our coding of the mandate states is identical to the coding of Bitler and Schmidt (2012) for all states but Connecticut and Ohio. Connecticut passed a law on 2005 which replaces the preexisting law from 1989. Our coding reflects this change. According to Bitler and Schmidt, Ohio had a mandate to cover between 1990 and 1997; after 1997, this law was converted into a mandate to offer. Since we were unable to find other supporting documents for this statement, here we consider Ohio as having a mandate to offer IVF coverage since 1990.
As a robustness check, we also check the results when all “weak mandate” states are included in the treatment group; these results are discussed in Section 6.
Women with a higher socioeconomic status and more education are more likely to hold employer-based health insurance (Bitler and Schmidt 2012), and be able to afford the high out-of-pocket expenditure associated with the use of infertility treatments even with insurance coverage.
The New York Times article can be found at http://www.nytimes.com/2015/07/23/upshot/more-than-their-mothers-young-women-plan-career-pauses.html. The original HBS study can be found at http://www.hbs.edu/women50/docs/L_and_L_Survey_2Findings_12final.pdf.
A few articles that discuss these expectations can be found at: http://jezebel.com/5883016/young-people-totally-think-theyre-infertile; https://www.guttmacher.org/about/journals/psrh/2012/02/missed-conceptions-or-misconceptions-perceived-infertility-among; http://jezebel.com/5859741/the-fertility-denial-complex; http://www.today.com/id/45262603.
National Longitudinal Survey of Youth 1979
This is a strongly simplified model of reality in which we ignore all other costs of delayed fertility other than the cost of lost earnings. These ignored costs certainly include personal preferences for fertility timing.
We exclude survey years before 1977 because prior to 1977 not all the states are identified individually.
Prior to 1992, post-high school degrees cannot be differentiated in the CPS. For survey years 1977–1991, we define an individual as having a college degree if she has completed 4 years of college. From 1992 onwards, a respondent is said to have a college degree only if she has a bachelor’s degree or higher.
A degree in veterinary sciences is an exception. However, most of those who apply for veterinary school have a bachelor’s degree.
Most traditional students will have completed college by age 25. See Goldin et al. (2006).
Following the IPUMS documentation, we weight each observation by the variable wtsupp.
This less restrictive treatment group is made up of both states that enacted legislation to mandate IVF coverage and also those passing mandates to offer ART coverage, or mandates to cover infertility treatments but explicitly excluding IVF-related procedures.
This sample excludes all states that passed a mandate before 1992.
The occupation sample includes eight mandate states (Arkansas, Connecticut, Hawaii, Illinois, Maryland, Massachusetts, New Jersey, and Rhode Island) and the CPS education sample includes two mandate states (Connecticut and New Jersey). This is because between 1992 and 2012, only Connecticut and New Jersey passed an insurance mandate to cover infertility treatments. The CPS education sample does not include states that passed a mandate before 1992 because there would be no pre-treatment period for these states.
To clarify the timeline range: the starting point of t=-8 is because the first mandate event was in 1985 and our earliest data are from the 1977 CPS. The latest data from the 2012 CPS correspond to t=7 for the latest mandate event in 2005. The Treatment States value at t = 0 is the mean of the professional rate for Maryland in 1985, Arkansas in 1987, Hawaii in 1987, Massachusetts in 1987, Illinois in 1991, New Jersey in 2001, and Connecticut in 2005 (recall that Montana was dropped from our dataset). The subsequent value at t=1 is the mean professional rate 1 year after the mandate in each of these respective states. To construct the value for the Control States series, the variable on the vertical axis in a mandate year is given by the average of the value in the years in which treatment states passed a mandate. That is, the value at t=0 is the mean of the control group professional rate across the following years: 1985, 1987, 1987, 1987, 1980, 2001, and 2005. Notice that the 1987 rate is triple weighted since three states passed a strong mandate that year: Arkansas, Hawaii, and Massachusetts. In constructing the control group series, we follow the method used by Ayres and Levitt (1998).
We test for pre-mandate differential trends using a difference in differences specification and data from the 1970 and 1980 Censuses. The data is limited but the results suggest there may be a pre-existing trend for degree outcomes. These results provide further support for the triple difference model and are available upon request.
Our identification strategy is close to Schmidt (2007), with two main differences. First, she uses older women as a treatment group and younger women as a control group. Second, Schmidt (2007) exploits variation across women’s age in the calendar year. Instead, here, we exploit variation across women’s age at the time of the mandates.
This is conditional on having worked in the past 5 years. This is a necessary condition in order for us to use older women as a control group. If we only observed the data for working women, older women would form a poor control group given that the ART mandates have a negative effect on their labor supply, as shown by Buckles (2007).
NSFG, 2003 and 2010. These statistics are for native-born women only.
When choosing which controls to add, we followed previous research on the effect of the availability of the pill on women’s career. We include most of the controls in Table 2 of Bailey (2006).
Our specification could be also written as: \(Pr(Y_{iskt}=1)=\alpha +\beta _{1}\text {Mandate}_{t} \times \text {35orYoungerMandate}_{sk} + \beta _{2}\text {Mandate}_{t}\\ + \beta _{3}\text {EverMandate}_{s}\times \gamma _{k}+ \beta _{4}X_{iskt} + \sum \limits _{kt} \mu _{kt}\\ + \sum \limits _{s}\delta _{s}\times t +\delta _{s}+\gamma _{k}+\tau _{t}+\epsilon _{iskt} \)where Mandate t is an indicator that takes value one after the mandate was passed in a mandate state. This notation is similar to the one used by Schmidt (2007).
Controlling for quadratic time trends, \(({\sum }_{s}\delta _{s}\times t^{2})\) produced identical results.
Since there is no mandate year defined for states in the control group, we approximate the mandate year by defining t=0 in control group states as 1995, which is the midpoint of all the true mandate years.
This coefficient is represented by ß 1 in Eq. 1.
The professional occupation rate among mandate state women rose from 0.0203 in 1985 to 0.0346 in 2012, an increase of 1.4 percentage points. A mandate effect of 0.012 and a change in exposure of 11.9 % would imply a predicted change of 0.012×0.119=.00143, or 0.14 percentage points. This accounts for 10 % of the observed increase.
Goldin and Katz use two key occupation outcomes, and it is important to clarify that here we reference their results for a narrow group of occupations that matches our professional occupations outcome: lawyers, doctors, veterinarians, and dentists. See Goldin and Katz (2002) Table 5, column 4, row 3.
As an alternative to state-specific linear trends, we also estimated the model controlling for state-specific quadratic trends. When including the full quadratic expression, STATA drops the squared term; the linear and squared term appear to be colinear.
The 2010 ACS is a reweighted combination of the ACS surveys conducted in 2009, 2010, and 2011 (IPUMS ACS 2009-2011 3-year sample).
As additional robustness checks, we replicate our results for both occupation and education within the unweighted CPS dataset. The unweighted CPS regression results are qualitatively very similar to the main results in Tables 4 and 5 although the magnitude of the mandate coefficients is a bit smaller. These results are available upon request.
Documentation from the US Census urges caution in comparing rates, ratios, and distributions between Census and ACS, and between ACS samples of different years (guide available at: http://www.census.gov/programs-surveys/acs/guidance/comparing-acs-data/2010.html). Furthermore, professional degrees are not identified in the 1980 Census and therefore we defined them as having at least 7 years of education. While the triple difference estimate is still valid from this patch-worked sample (year fixed effects are included), we cannot accurately measure the change in the rate over the full time period.
This is similar to the placebo test mentioned in footnote 25 and the results are available upon request.
This difference is marginally significant at the 10% level, with a z-statistic of 1.36
This variable is available for only a subset of years in our study period; these years are specified in the table note.
We drop states that are assigned a weight equal to zero. The states included in the refined control group are Alabama, Delaware, District of Columbia, Michigan, Minnesota, Mississippi, Oklahoma, Pennsylvania, Utah, Vermont, Virginia, and Wisconsin.
The category “non-traditional occupations” is taken from Bailey et al. (2012).
Alternative outcomes that warrant consideration include MBAs and PhDs. MBAs satisfy the three requirements described above: high up-front educational investment, a demanding and inflexible schedule, and high earnings. The typical educational investment of an MBA—2 years—is shorter than the one required by professional degrees, but still carries a hefty tuition price tag, generally paid out of pocket. Careers in finance or consulting, which are a common placement for MBAs, require long working hours and pay high salaries. Unfortunately, looking at the effect of mandates on the probability of obtaining an MBA is not possible because neither the CPS nor the Census allow distinguishing MBAs from other Master degrees. Combining MBA and MA outcomes showed no impact of the mandates. The data do allow looking at PhDs separately. However, although a doctoral degree is a long investment, PhDs often have a flexible schedule and on average earn lower earnings relative to professionals. Analysis of PhD outcomes yields a coefficient on the triple interaction term that is small, negative, and statistically insignificant, suggesting that the mandates do not affect the probability that women obtain a PhD. These results are available upon request.
For consistency, we exclude women aged 31 to 35 in 1995 in control states. 1995 is the midpoint of the years in which mandates were adopted in treatment states.
Less precision is expected given the particularly small size of the “other race” sample.
This practice is likely to grow more common with widely publicized announcements of such employee benefits by Facebook and Apple. http://www.nbcnews.com/news/us-news/perk-facebook-apple-now-pay-women-freeze-eggs-n225011
References
Abadie A, Diamond A, Hainmueller J (2010) Synthetic control methods for comparative case studies: estimating the effect of California’s tobacco control program. J Am Stat Assoc 105:490
Abramowitz J (2012) Assisted reproductive technology and women’s marriage and birth timing: duration and competing risks analyses.Unpublished manuscript
Abramowitz J (2014) Turning back the ticking clock: the effect of increased affordability of assisted reproductive technology on women’s marriage timing. J Popul Econ 27(2):603–633
Adashi EY, Cohen J, Hamberger L, Jones HW Jr, De Kretser DM, Lunenfeld B, Rosenwaks Z, Van Steirteghem A (2000) Public perception on infertility and its treatment: an international survey. The Bertarelli Foundation Scientific Board. Hum Reprod, (Oxford, England) 15(2):330–334
Aleccia J (2011) Fertility math? Most women flunk, survey finds. Today. November 15
Ayres I, Levitt SD (1998) Measuring positive externalities from unobservable victim precaution: an empirical analysis of Lojack. Q J Econ 113(1):43–77
Bailey MJ (2006) More power to the pill: The impact of contraceptive freedom on women’s life cycle labor supply. Q J Econ 21(1):289–320
Bailey MJ, Hershbein B, Miller AR (2012) The opt-in revolution? Contraception and the gender gap in wages. American Economic Journal: Applied Economics 4(3):225–54
Becker GS (1975) Human capital: a theoretical and empirical analysis, with special reference to education. National Bureau of Economic Research: distributed by Columbia University Press
Bertrand M, Duflo E, Mullainathan S (2004) How much should we trust differences-in-differences estimates?. Q J Econ 119(1):249–275
Bitler MP, Schmidt L (2012) Utilization of infertility treatments: the effects of insurance mandates. Demography 49(1):125–149
Buckles KS (2007) Stopping the biological clock: infertility treatments and the career-family trade-off. Boston University, Unpublished manuscript
Buckles KS (2013) Infertility insurance mandates and multiple births. Health Econ 22(7):775–789
Centers for Disease Control and Prevention (CDC) (2014) Infertility FAQs. Last accessed June 4, 2014. http://www.cdc.gov/reproductivehealth/Infertility/Index.htm
Conley TG, Taber CR (2011) Inference with “difference in differences” with a small number of policy changes. Rev Econ Stat 93(1):113–125
Goldin C, Katz LF (2002) The power of the pill: oral contraceptives and women’s career and marriage decisions. J Polit Econ 110(4):730–770
Goldin C, Katz LF, Kuziemko I (2006) The homecoming of American college women: the reversal of the college gender gap. J Econ Perspect 20(4):133–156
Gruber J (1994) The incidence of mandated maternity benefits. Am Econ Rev 84(3):622–641
Hamilton BH, McManus B (2012) The effects of insurance mandates on choices and outcomes in infertility treatment markets. Health Econ 21(8):994–1016
Hewlett SA (2002) Executive women and the myth of having it all. Harvard Business Review. http://hbr.org/2002/04/executive-women-and-the-myth-of-having-it-all
King M, Ruggles S, Alexander JT, Flood S, Genadek K, Schroeder MB, Trampe B, Vick R (2010) Integrated public use microdata series, current population survey: version 3.0 [Machine-readable database]. University of Minnesota, Minneapolis
Leung MYM, Groes F, Santaeulalia-Llopis R (2016) The relationship between age at first birth and mother’s lifetime earnings: evidence from danish data. PloS one 11(1):e0146989
Machado MP, Sanz-de-Galdeano A (2015) Coverage of infertility treatment and fertility outcomes. SERIEs 6(4):407–439
Miller AR (2011) The effects of motherhood timing on career path. J Popul Econ 24(3):1071–1100
Miller CC (2014) Freezing eggs as part of employee benefits: some women see darker message. New York Times. October 14
Miller CC (2015) More than their mothers, young women plan career pauses? New York Times. July 22
National Center for Education Statistics (2011) Digest of Education Statistics
North A (2012) Young people totally think they’re infertile? Jezebel. February 7
Ohinata A (2011) Did the US infertility health insurance mandates affect the timing of first birth?. Unpublished manuscript
Polis CB, Zabin LS (2012) Missed conceptions or misconceptions: perceived infertility among unmarried young adults in the United States. Perspect Sex Reprod Health 44(1):30–38
RESOLVE (2014) RESOLVE Insurance Coverage in Your State. Last accessed June 4, 2014. http://www.resolve.org/family-building-options/insurance_coverage/state-coverage.html
Ruggles S, Genadek K, Goeken R, Grover J, Sobek M (2015) Integrated Public Use Microdata Series: Version 6.0 [Machine-readable database]. Minneapolis: University of Minnesota, 2015
Ryan EG (2011) The fertility denial complex? Jezebel. November 15
Schmidt L (2007) Effects of infertility insurance mandates on fertility. J Health Econ 26(3):431–446
William M, Mercer Company (1997) Women’s health issues: infertility as a covered benefit
Acknowledgments
The authors would like to thank Daniele Paserman, Claudia Olivetti, Lucie Schmidt, Mark Herander, Kevin Mumford, Osea Giuntella, Maria Navarro Paniagua, Colin Greene, Amalia Miller, Melanie Guldi, Joshua Wilde, Lisa Kahn, David Slusky, two anonymous referees, and numerous seminar and conference participants for helpful comments and suggestions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Junsen Zhang
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Kroeger, S., La Mattina, G. Assisted reproductive technology and women’s choice to pursue professional careers. J Popul Econ 30, 723–769 (2017). https://doi.org/10.1007/s00148-016-0630-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00148-016-0630-z
Keywords
- Occupational choice
- Insurance mandates
- Fertility
- Professional careers
- Professional degrees
- Assisted reproductive technology