
Abstract
Purpose
Severe community-acquired pneumonia (SCAP) is still associated with substantial morbidity and mortality. In this point-of-view review paper, a group of experts discuss the main controversies in SCAP: the role of severity scores to guide patient settings of care and empiric antibiotic therapy; the emergence of pathogens outside the core microorganisms of CAP; viral SCAP; the best empirical treatment; septic shock as the most lethal complication; and the need for new antibiotics.
Methods
For all topics, the authors describe current controversies and evidence and provide recommendations and suggestions for future research. Evidence was based on meta-analyses, most recent RCTs and recent interventional or observational studies. Recommendations were reached by consensus of all the authors.
Results and conclusions
The IDSA/ATS criteria remain the most pragmatic tool to predict ICU admission. The authors recommend a combination of a beta-lactam/beta-lactamase inhibitor or a third G cephalosporin plus a macrolide in most SCAP patients, and to empirically cover PES (P. aeruginosa, extended spectrum beta-lactamase producing Enterobacteriaceae, methicillin-resistant S. aureus) pathogens when at least two specific risk factors are present. In patients with influenza CAP, the authors recommend the use of oseltamivir and avoidance of the use of steroids. Corticosteroids can be used in case of refractory shock and high systemic inflammatory response.
Similar content being viewed by others

A group of experts discuss current controversies regarding severe community-acquired pneumonia and provide a summary of recommendations. |
Background
During recent decades, the number of patients requiring intensive care management due to severe community-acquired pneumonia (SCAP) has increased globally, especially among the elderly, patients with comorbidities and the immunocompromised [1]. A large population-based surveillance study on hospitalized CAP patients found that 21% of patients required intensive care unit (ICU) admission, with 26% of them needing mechanical ventilation [2]. SCAP hospital mortality is still high, ranging from 25% to more than 50% [3, 4]. Since delays from hospitalization to ICU admission have been related to increased mortality [5], several scoring systems have been evaluated in order to promptly identify patients requiring intensive care management and to guide empiric antibiotic therapy [6].
Streptococcus pneumoniae remains the main pathogen responsible of CAP, regardless of age and comorbidities [7]. However, approximately 6% of CAP are caused by antibiotic-resistant pathogens [8]. Furthermore, the implementation of multiplex polymerase chain reaction (PCR) techniques has identified respiratory viruses, mainly influenza virus and rhinovirus, as important CAP causative pathogens [2].
Early adequate antibiotic administration is crucial in SCAP management [9]; however, the optimal strategy is still far from being established. Initial antimicrobial therapy lacking activity against the offending pathogens has been associated with greater mortality [10]. The cluster RCT from Postma et al. [11] showed the same efficacy when comparing beta-lactam monotherapy with beta-lactam plus macrolide or quinolone. The constant debate regarding the superiority of β-lactam plus macrolide compared to β-lactam plus fluoroquinolones in SCAP is still open [12].
Septic shock is the most lethal complication of SCAP. Corticosteroids are recommended in refractory septic shock, although some controversies still remain. Due to the emergence of pathogens outside the core microorganisms of CAP [13], new antibiotics are urgently needed.
In this point-of-view review paper, a group of experts discuss the current main controversies regarding SCAP: severity scores, pathogens outside the core microorganisms of CAP (PES pathogens), viral SCAP, empirical treatment, septic shock and the potential role of new antibiotics. All the topics include four sections: the current controversy, the evidence, suggested recommendations and suggestions for future research. The evidence was based on meta-analyses, most recent RCTs and recent interventional or observational studies that the panel considered important for the question. Recommendations were reached by consensus of all the authors and are summarized in Table 1.
Identifying severe CAP
Current controversy
Severity assessment is an essential component of the initial evaluation of CAP patients [14]. To date, there is no consensus on the optimal assessment tool or how it should be applied in clinical practice [15, 16].
Some “real-world” problems may complicate the interpretation of studies that investigate scores for ICU admission prediction [15]. In one study, 1/3 of patients presenting to hospital had advanced directives or do not attempt resuscitation (DNAR) orders in place that made ICU admission inappropriate [17]. Second, many studies include patients who require mechanical ventilation or vasopressor treatment at admission in “prediction” studies, making a prediction score moot [18]. Third, the number of adult ICU beds [19], the threshold for ICU admission and the characteristics of patients admitted to ICU are highly variable across different healthcare systems. Finally, there is still relatively little evidence that implementation of severity tools into clinical practice results in improved outcomes [20].
The evidence
The two most widely used severity assessment tools in CAP, the pneumonia severity index (PSI) and the CURB65 score, perform well to predict 30-day mortality, but are less useful in identifying SCAP requiring ICU admission [15]. This reflects the strong influence of age on both scoring systems, and the low value provided to respiratory failure and other organ dysfunctions which are often a major driver of ICU admission.
Alternative scoring systems have been proposed that are more focused on organ dysfunction. The IDSA/ATS 2007 criteria (Table 2) predict both mortality and future requirements for mechanical ventilation and vasopressor support as a surrogate of ICU admission [21]. Simplification of these criteria with the removal of less common organ dysfunctions is possible without losing prognostic accuracy. Lim et al. [20] conducted a before and after implementation study in which the IDSA/ATS criteria were used to triage patients. This resulted in a reduced mortality (from 23.8 to 5.7%), an increased use of ICU resources (52.9% of patients admitted to the ICU vs.. 38.6% previously) and reduced delayed ICU admissions. Similar criteria are included in the SMART-COP tool [22]. Recently, it has been shown that Sepsis-3 criteria can also help to identify patients at risk of ICU admission, although disease-specific tools still have the best discrimination for mortality [6].
Suggested recommendations
The IDSA/ATS 2007 criteria remain the most pragmatic and robust tools for predicting patients requiring ICU admission. Major criteria identify patients requiring immediate ICU care, while minor criteria (either the simplified or standard version) identify patients with a higher likelihood of requiring ICU care and benefiting from more aggressive therapy or closer observation [15, 20, 21]. PSI and CURB65 should not be used to guide ICU care as they can be misleading. Biomarkers such as C reactive protein, proadrenomedullin, procalcitonin and others have been suggested to provide additional information about CAP prognosis [23, 24]. None are currently fully validated and ready for implementation in clinical practice.
Suggestions for future research
We need data demonstrating the utility of severity scores to predict a complicated course of CAP, to help improving patient allocation (need for ICU admission) and to identify patients likely to respond to specific therapies, including corticosteroids or macrolides [23–25]. Finally, we need data demonstrating a lower mortality rate when these scoring systems are used.
Risk factors for pathogens outside the core microorganisms of CAP: the PES (P. aeruginosa, extended spectrum beta-lactamase producing Enterobacteriaceae and methicillin-resistant S. aureus) pathogens
Current controversy
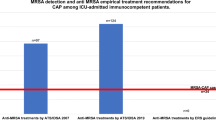
Guidelines for CAP recommend empiric therapy for pathogens outside the core microorganisms of CAP, including methicillin-resistant S. aureus (MRSA), P. aeruginosa and other drug-resistant Gram-negatives, in selected patients with severe illness [26]. However, the incidence of these pathogens in CAP is low and often varies with geography and patient characteristics. The healthcare-associated pneumonia (HCAP) definition is not a good predictor of these pathogens [27]. Identifying patients at higher risk could avoid the overuse of broad-spectrum empiric therapy.
The evidence
In one study of 267 ICU-admitted CAP patients, one in six Pseudomonas were resistant to third-generation cephalosporins with antipseudomonal activity. Common pathogens included E. coli (8.2%), P. aeruginosa (8.2%), Klebsiella pneumoniae (5.6%), MRSA (1.1%), Stenotrophomas maltophilia (0.7%) and Acinetobacter baumannii (0.3%) [28]. In one review, the incidence of Gram-negative CAP was estimated to be between 5 and 30%, but not all these organisms were resistant and not all patients were in the ICU [29]. Shindo et al. reported 8.6% of CAP and 26.6% of HCAP caused by drug-resistant pathogens [30]; however, the number of patients treated in ICU was not stated. Similarly, in another study, 5.2% of CAP and 10.9% of HCAP were caused by pathogens outside the core microorganisms of CAP, but only 57 of 889 were treated in ICU [31].
One recent development is the concept of PES (P. aeruginosa, extended-spectrum beta-lactamase producing Enterobacteriaceae and MRSA) pathogens. PES pathogens have been identified in 6% of CAP patients with an etiologic diagnosis, with P. aeruginosa being the most common; 20–30% of patients with PES pathogens required ICU admission, more often than those without these pathogens [13]. In another study of 705 CAP patients, PES pathogens were found in 7.2% patients but ICU admission was needed in only 5.9% cases, a rate similar to those without PES pathogens [32].
Risk factors for PES pathogens have been identified, although most studies are not specific to ICU patients (Table 3). Webb et al. divided risk factors into therapy-related (extrinsic factors), patient-related (intrinsic factors) and those related to selective antibiotic pressure [27]. In one study, risk factors were prior antibiotic therapy, gastric acid-suppressive therapy, tube feeding and non-ambulatory status [30], while in another study were CAP severity, prior antibiotic therapy, recent hospitalization, poor functional status, dialysis and immune suppression [31]. In a study of bacteremic CAP due to PES pathogens, risk factors for these pathogens were prior antibiotic therapy, low C-reactive protein (CRP) and the absence of pleuritic chest pain [33].
Some studies have focused on risks for specific pathogens. A multinational study of 3193 patients found P. aeruginosa in 4.2% and antibiotic-resistant P. aeruginosa in 2% [34]. Risk factors for P. aeruginosa were prior P. aeruginosa infection/colonization, need for mechanical ventilation or vasoactive drugs and chronic airways diseases. However, chronic airways diseases were not a risk for antibiotic-resistant P. aeruginosa. In another study, risk factors for P. aeruginosa CAP included male sex, chronic respiratory diseases, lower CRP and higher PSI. However, the only risk factor for antibiotic-resistant P. aeruginosa was prior antibiotic therapy [8]. Risk factors for MRSA included many of the above plus chronic dialysis, prior MRSA infection/colonization, recurrent skin infections and severe comorbidities [30, 35]. The studies that investigate risk factors for PES pathogens often use the term "multidrug resistent" (MDR), although they include indistinctly MDR and non-MDR microorganisms, mainly P. aeruginosa. In this manuscript we decided to use the acronym PES because we believe it reflects better the need for a different antibiotic treatment covering these pathogens (carbapenems +/- linezolid) compared to the standard one required for the “core” CAP pathogens.
Suggested recommendations
We recommend covering PES pathogens when specific risk factors are present, including prior antibiotic therapy, recent hospitalization, recent P. aeruginosa or MRSA infection or colonization, poor functional status and immune suppression. When patients have at least 2 risk factors, the frequency of PES pathogens can exceed 25%, thus requiring empiric therapy against these pathogens. [30, 31].
Suggestions for future research
We need prospective studies using invasive sampling methods and new molecular diagnostic tests in a population of CAP patients treated exclusively in ICU. We need to identify patients at higher risk of PES pathogens through accurate scoring systems and to determine a threshold above which empiric therapy for these pathogens is justified. Finally, we need to be aware of SCAP microbiology future changes induced by influenza and pneumococcal vaccination, in both adults and children.
Viral SCAP
Current controversy
Before the appearance of influenza pandemics, respiratory viruses were uncommonly diagnosed and affected essentially patients with comorbidities [36]. In fact, influenza virus A is the most frequent respiratory virus identified, followed by human rhinovirus, human respiratory syncytial virus (RSV) and influenza B virus. RSV is now recognized as a significant problem in the elderly, persons with cardiopulmonary diseases and immunocompromised hosts [37]. A major controversy in patients with suspected severe viral CAP (svCAP) is twofold: the use of unnecessary antibiotics when the primary cause of pneumonia is viral without co-infection, and possible treatments with antiviral agents.
The evidence
Currently, recommendations for patients with svCAP are focused on rapid recognition of the pathogen and antiviral treatment with Neuraminidase Inhibitors (NAIs). Recommendations regarding NAIs administration are controversial. The Cochrane review of the topic in 2014 concluded that oseltamivir did not reduce hospitalizations and complications due to influenza [38]. Two systematic reviews and meta-analyses found that benefits in patients who were otherwise healthy did not outweigh its risks [39, 40]. However, another meta-analysis found that oseltamivir was effective in the prevention of influenza at individual and household levels. In critically ill patients, observational studies have found a benefit to a prompt use of oseltamivir [41]. On the other hand, zanamivir has been proposed by different guidelines, especially in immunosuppressed patients, based on a potential antiviral resistance to oseltamivir among circulating influenza viruses that is currently low [42]. Inhaled zanamivir is not recommended because of the lack of data regarding its use in patients with severe influenza disease.
The use of corticosteroids has re-emerged in patients with SCAP based on recent randomized control trials (RCT) and systematic review and meta-analysis [43, 44]. In patients with svCAP, the use of corticosteroids has not been associated with survival benefit but with an increased risk of nosocomial infections [45]. A recent observational study found that corticosteroid administration as adjuvant therapy to standard antiviral treatment in critically ill patients with severe influenza pneumonia was associated with increased ICU mortality [46].
Regarding RSV, not many treatment options are available, while a phase 2b RCT of presatovir for the treatment of RSV in lung transplant recipients has been recently published with no positive results.
Suggested recommendations
We suggest maintaining an active communication with sentinel national and continental centers, and a local routine surveillance program in hospital settings [47]. We advocate diagnosing svCAP in accordance with a seasonal activity pattern. We encourage prompt treatment with oseltamivir in patients with svCAP within the first 48 h from influenza diagnosis. We recommend not using zanamivir regularly and only on the basis of treatment failure and confirmed oseltamivir mutations. A RCT has not demonstrated a superior effect of zanamivir compared to oseltamivir; all treatments had a similar safety profile in hospitalised patients with severe influenza [48]. We recommend avoiding the use of steroids in patients with svCAP due to futile effect and an increased risk of super-infections in all subgroups of patients including the immunosuppressed. In cases of RSV, there is no available treatment at the present time.
Suggestions for future research
The best preferable evidence to determine the effect of NAIs should come from RCTs. Currently, only very few patients with high severity rates and a PSI above 90 have been enrolled in RCTs for SCAP [49]. In addition, in patients with infections, performing a RCT with or without antibiotics will foremost be inappropriate and unethical. Although there is sufficient evidence that antivirals decrease viral loads, their use in SCAP is still a matter of controversy [50]. Studies analyzing the timing of NAIs administration could provide further positive results. Regarding the use of corticosteroids, a RCT could be conducted in svCAP patients with high inflammation and severity.
Empirical treatment of SCAP
Current controversy
No RCT has specifically targeted SCAP. Only one allowed enrollment of mechanically ventilated patients, while the rest specifically excluded SCAP patients [51]. Conversely, epidemiologic data suggest that SCAP patients may have a different etiologic spectrum than patients hospitalized outside the ICU [2, 52], including a high incidence of viral infection. Therefore, whether antibiotics appropriate for non-ICU patients are safe and efficacious in SCAP is unclear. Moreover, rapid diagnostic tests offer the possibility for specific treatment. If they demonstrate high sensitivity for atypical pathogens, fluoroquinolone monotherapy may even be superior to macrolides. Whether other effects of macrolides are beneficial in cases other than S. pneumoniae is debatable, and beta-lactams are clearly not needed for atypicals.
The controversy is threefold: (1) is beta-lactam/macrolide combination therapy superior to other beta-lactam treatments? (2) Are additional antibiotics required for PES pathogens? And (3) is prolonged antibiotic therapy needed for all patients with only positive viral testing?
The evidence
Non-interventional trials suggest that beta-lactam/macrolide combination therapy is associated with lower mortality, especially in patients with pneumococcal bacteremia [53].
However, the study by Postma et al. [11] found no difference in 90-day mortality when comparing beta-lactam alone with beta-lactam/macrolide or quinolones. The study exhibits two important limitations: first, 25% of patients had no chest X-ray confirmation; second, most patients had a low-grade severity pneumonia, as measured by the PSI scale. Another RCT study [54] found a lower rate of readmissions and a higher rate of clinical cure only in patients with PSI categories IV and V pneumonia receiving beta-lactam plus macrolide.
Observational studies of beta-lactam/quinolone combination therapy for SCAP suggest better outcome than beta-lactam monotherapy. One prospective study found combination therapy with an early quinolone was slightly superior to a cephalosporin alone [51]. Three theories support the benefit of empirical macrolide combination: (1) better coverage of atypical pathogens, including Legionella, (2) suppression of exotoxin production from S. pneumoniae [55], and (3) host immunomodulatory effects. The latter two clearly differentiate between macrolides and quinolones, although both are effective against atypical pathogens. The underlying assumption that most of these culture-negative cases are S. pneumoniae is questionable with greater use of the highly-effective conjugate pneumococcal vaccines [56]. Some data support the use of quinolones for proven severe Legionella [57]. Methicillin-sensitive strains are likely covered adequately with standard empirical therapy. However, empirical coverage of MRSA for all SCAP patients does not improve outcomes [58]. Gross hemoptysis, leukopenia, skin rashes, and rapidly progressive or necrotizing infiltrates are relatively distinctive for the toxigenic community-acquired strain [59]. Observational studies suggest a better outcome with the use of antibiotics that interfere with ribosomal synthesis, such as linezolid or clindamycin [60]. Whether more rapid killing associated with the cephalosporin ceftaroline obviates the need for toxin suppression is unknown [61].
Patients with SCAP who are at risk for pathogens usually considered nosocomial represent a therapeutic dilemma. Unfortunately, piperacillin/tazobactam, the most commonly prescribed antibiotic for suspected drug-resistant pathogens, has recently been shown to have adverse outcomes in patients with E. coli and K. pneumoniae bloodstream infection and ceftriaxone resistance [62].
In cases of svCAP, the overwhelming majority of patients receive empirical antibiotics despite infrequently documented bacterial superinfection. Short-course prophylactic antibiotics may prevent bacterial superinfection while prolonged courses predispose to nosocomial infections, disrupting gut and lung microbiomes.
It is worth pointing out that some SCAP cases require longer antibiotic administration. These include SCAP caused by S. aureus, patients with pleural effusions, pulmonary abscess and, patients with initial inadequate antibiotic treatment.
Suggested recommendations
We recommend a combination of a beta-lactam/beta-lactamase inhibitor or a third G cephalosporin plus a macrolide for most SCAP patients. Legionella, if documented, should be treated with a quinolone. Empirical linezolid should be reserved to patients with risk factors for community-acquired MRSA. Empirical broader spectrum therapy for Gram-negative pathogens should be limited to patients with several risk factors for PES pathogens.
Suggestions for future research
We need a RCT of usual treatment (cephalosporin/macrolide) with additional empirical coverage for PES pathogens versus pathogen-specific therapy based on rapid diagnostic testing. We need interventional studies investigating the duration of SCAP antibiotic treatment according to procalcitonin and rapid molecular diagnostic techniques. Finally, we need a RCT of short-course antibiotic therapy for SCAP patients with only viral detection on molecular testing.
Septic shock and corticosteroids in SCAP
Current controversy
Pneumonia is the most common cause of septic shock [63]. Despite improvements in the overall survival from severe sepsis, mortality from SCAP remains high—up to 50% in some studies [64]. Reasons for this discrepancy remain unclear, but it suggests the possibility that SCAP represents a unique subset of septic shock that deserves a unique set of guidelines for management. The high mortality in SCAP, despite early and adequate antibiotic treatment, may be a result of inadequate infection control and/or dysregulated inflammatory responses. The latter possibility raises the perennial question in the management of SCAP of whether or not to employ systemic corticosteroid therapy.
The evidence
Current strategies to manage patients with SCAP and shock include the identification of pathogens using available diagnostics [65], early and appropriate (including combination) antimicrobial administration [66], hemodynamic resuscitation [67], and, for some patients, appropriate management of acute respiratory failure or ARDS [68].
Two recent RCTs, the ADRENAL and the APPROCCHSS, supported the use of adjunct corticosteroid therapy in septic shock (Table 4), both studies demonstrating a reduction in the number of vasopressor- and ventilator-dependent days [69, 70]. In these studies, 34% and 59% of patients had pulmonary infections, respectively. The APPROCCHSS demonstrated a small mortality benefit, a feature some authors attributed to the inclusion of mineralocorticoids in the treatment protocol. However, this finding may be better explained by the higher baseline mortality in the latter trial, which would fit with the general trend in steroid trials dating back to 2002 (including the French Trial, HYPRESS, and CORTICUS), which showed the greatest benefit of therapy in the sickest populations [71–73]. A recent network meta-analysis of 23 septic shock studies supported with strong evidence the role of corticosteroids in shock reversal [74].
The use of steroids in SCAP (with or without shock) remains controversial [43, 44, 75,76,77,78,79,80,81,82,83], although many studies have shown significant reductions in length of stay and time to clinical stability. Increasing evidence suggests that patients with strong inflammatory responses, such as those with highly elevated CRP, may represent a subset of SCAP patients who would benefit from such corticosteroid treatment [43]. Conversely, corticosteroid use in patients with versus CAP has been related to increased mortality [84]. There is currently insufficient evidence to support other adjuvant therapies in SCAP, such as immunoglobulins, G-CSF or statins [85].
Suggested recommendations
Patients with SCAP and shock should be managed according to current practice guidelines. Adjunctive therapy, including systemic corticosteroids, should be reserved for SCAP patients with refractory septic shock or with high systemic inflammatory response (as measured by CRP).
Suggestions for future research
Studies are still needed to clarify why SCAP mortality remains high despite improvements in overall sepsis outcomes. Host inflammatory responses (both of the lung and systemic) require better characterization to determine the potential role of immune modulators in SCAP. Finally, additional studies are needed to better assess patients’ immune phenotype and to determine who should receive steroids and other immunosuppressive therapies.
New antibiotics
Current controversy
Treatment success in SCAP rests on prompt delivery of antibiotics targeting the likely causative organisms. An important controversy is whether existing antibiotics are adequate therapies or whether new antimicrobials are needed.
The evidence
Initial inappropriate empiric therapy in SCAP is primarily driven by the failure to cover a specific pathogen (e.g., MRSA) or the presence of a resistant bacterial pathogen (e.g., macrolide-resistant S. pneumoniae) [86]. The need to empirically cover both “typical” bacterial pathogens (S. pneumonia, Haemophilus influenza, MMSA) and “atypical” pathogens (Mycoplasma pneumoniae, Legionella pneumophilia, Chlamydophila pneumoniae) is controversial, with some studies showing no benefit when atypical coverage is provided and others suggesting outcome benefits [87, 88].
Based on the available data, it appears that new antibiotics providing coverage for the currently existing limitations in empiric therapy are needed (Table 5).
Lefamulin is a novel semisynthetic pleuromutilin that inhibits bacterial growth by binding to the peptidyl transferase center of the 50S ribosomal subunit [89]. Pleuromutilins are not typically affected by resistance to other antibiotic classes (including macrolides, fluoroquinolones, and tetracyclines). Two phase 3 trials (LEAP 1—intravenous to oral lefamulin; LEAP 2—oral only) have demonstrated comparable (non-inferior) outcomes to moxifloxacin (https://investors.nabriva.com/static-files/5c34b447-99cc-4739-b9d6-d4ea4c7d13b9 (Accessed 12 July 2018).
Omadacycline is from the aminomethylcycline class created by chemical modification of minocycline. It inhibits protein synthesis by binding to the 30S ribosomal subunit. Chemical modifications enable it to be active against the two main forms of bacterial resistance to the tetracyclines: efflux and ribosomal protection. Results from the phase 3 OPTIC trial comparing once-daily oral and intravenous omadacycline to oral and intravenous moxifloxacin demonstrated non-inferiority (https://globenewswire.com/news-release/2017/04/03/953801/0/en/Paratek-Announces-Positive-Phase-3-Study-of-Omadacycline-in-Community-Acquired-Bacterial-Pneumonia.html (Accessed 12 July 2018).
Delafloxacin (Baxdela™) is a potent fluoroquinolone with structural differences allowing it to move better than other fluoroquinolones through an acidic medium facilitating transmembrane passage into bacteria. Delafloxacin has a high affinity for both topoisomerase IV and DNA gyrase targets, giving it activity against Gram-positive and Gram-negative bacteria, as well as anaerobes and intracellular microorganisms [90]. The results of a phase 3 trial comparing delafloxacin to moxifloxacin for hospitalized patients with CAP are awaited.
Solithromycin (Solithera™) is a fourth-generation macrolide and the first fluoroketolide in clinical development. Solithromycin has potent in vitro activity against the most common CAP pathogens, including fluoroquinolone-resistant isolates of S. pneumoniae. Two phase 3 trials of oral and intravenous to oral therapy for CAP demonstrated comparable results to moxifloxacin [91]. However, due to concerns over potential liver toxicity, the FDA recommended that the company initiate a new clinical study to better evaluate the drug’s safety profile in 9000 patients.
Nemonoxacin is a novel nonfluorinated quinolone with a wide antimicrobial spectrum covering Gram-positive cocci and Gram-negative bacilli, including the common CAP pathogens. One published phase 2 trial and two unpublished phase 3 trials suggest that Nemonoxacin is non-inferior to levofloxacin for the treatment of CAP [92, 93].
Ceftaroline fosamil (Teflaro™) is an N-phosphonoamino water-soluble prodrug cephalosporin with the active form, ceftaroline, possessing broad-spectrum in vitro antimicrobial activity. The spectrum of activity includes typical CAP bacterial pathogens and its high affinity for PBP2a allows coverage of MRSA [94]. The high superiority of ceftaroline compared to ceftriaxone in bacterial pneumonia was demonstrated in the FOCUS 1 and 2 trials [61].
Suggested recommendations
The current role of the new antibiotics in SCAP is almost unknown, since the majority of them have not been studied in this specific subgroup of patients. Ceftaroline could be added to the list of beta-lactams for the empirical or targeted treatment of SCAP.
Suggestions for future research
We need observational and/or RCT studies of new antibiotics in the specific SCAP population. Non-traditional agents, such as monoclonal antibodies, that may minimize or avoid the emergence of resistance should also be explored.
Conclusions and summary
SCAP is a major challenge in ICU due to its high mortality, complications, short and long-term consequences. However, the optimal care is still not well standardized. SCAP remains a small section of general CAP recommendations, and performing interventional and RCTs in this subgroup of patients may be difficult. In this point-of-view review paper, we provide literature evidence, suggested recommendations and suggestions for future research regarding six seminal questions of SCAP management: (1) who needs to be admitted to ICU? (2) When should PES pathogens be suspected? (3) How should severe viral CAP be managed? (4) What is the optimal empirical antibiotic treatment for SCAP? (5) When should corticosteroids in SCAP with septic shock be used? And (6) what is the current evidence regarding new antibiotics and the pipe-line for coming years?
References
Laporte L, Hermetet C, Jouan Y, Gaborit C, Rouve E, Shea KM, Si-Tahar M, Dequin PF, Grammatico-Guillon L, Guillon A (2018) Ten-year trends in intensive care admissions for respiratory infections in the elderly. Ann Intensive Care 8:84
Jain S, Self WH, Wunderink RG, Fakhran S, Balk R, Bramley AM, Reed C, Grijalva CG, Anderson EJ, Courtney DM, Chappell JD, Qi C, Hart EM, Carroll F, Trabue C, Donnelly HK, Williams DJ, Zhu Y, Arnold SR, Ampofo K, Waterer GW, Levine M, Lindstrom S, Winchell JM, Katz JM, Erdman D, Schneider E, Hicks LA, McCullers JA, Pavia AT, Edwards KM, Finelli L (2015) Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 373:415–427
Cilloniz C, Dominedo C, Garcia-Vidal C, Torres A (2018) Community-acquired pneumonia as an emergency condition. Curr Opin Crit Care 24:531–539
Montull B, Menendez R, Torres A, Reyes S, Mendez R, Zalacain R, Capelastegui A, Rajas O, Borderias L, Martin-Villasclaras J, Bello S, Alfageme I, Rodriguez de Castro F, Rello J, Molinos L, Ruiz-Manzano J (2016) Predictors of severe sepsis among patients hospitalized for community-acquired pneumonia. PLoS ONE 11:e0145929
Woodhead M, Welch CA, Harrison DA, Bellingan G, Ayres JG (2006) Community-acquired pneumonia on the intensive care unit: secondary analysis of 17,869 cases in the ICNARC Case Mix Programme Database. Crit Care 10(Suppl 2):S1
Ranzani OT, Prina E, Menendez R, Ceccato A, Cilloniz C, Mendez R, Gabarrus A, Barbeta E, Bassi GL, Ferrer M, Torres A (2017) New sepsis definition (sepsis-3) and community-acquired pneumonia mortality. A validation and clinical decision-making study. Am J Respir Crit Care Med 196:1287–1297
Said MA, Johnson HL, Nonyane BA, Deloria-Knoll M, O’Brien KL, Andreo F, Beovic B, Blanco S, Boersma WG, Boulware DR, Butler JC, Carratala J, Chang FY, Charles PG, Diaz AA, Dominguez J, Ehara N, Endeman H, Falco V, Falguera M, Fukushima K, Garcia-Vidal C, Genne D, Guchev IA, Gutierrez F, Hernes SS, Hoepelman AI, Hohenthal U, Johansson N, Kolek V, Kozlov RS, Lauderdale TL, Marekovic I, Masia M, Matta MA, Miro O, Murdoch DR, Nuermberger E, Paolini R, Perello R, Snijders D, Plecko V, Sorde R, Stralin K, van der Eerden MM, Vila-Corcoles A, Watt JP (2013) Estimating the burden of pneumococcal pneumonia among adults: a systematic review and meta-analysis of diagnostic techniques. PLoS ONE 8:e60273
Cilloniz C, Gabarrus A, Ferrer M, Puig de la Bellacasa J, Rinaudo M, Mensa J, Niederman MS, Torres A (2016) Community-acquired pneumonia due to multidrug- and non-multidrug-resistant pseudomonas aeruginosa. Chest 150:415–425
Garnacho-Montero J, Barrero-Garcia I, Gomez-Prieto MG, Martin-Loeches I (2018) Severe community-acquired pneumonia: current management and future therapeutic alternatives. Expert Rev Anti Infect Ther 16:667–677
Pereira JM, Goncalves-Pereira J, Ribeiro O, Baptista JP, Froes F, Paiva JA (2018) Impact of antibiotic therapy in severe community-acquired pneumonia: data from the Infauci study. J Crit Care 43:183–189
Postma DF, van Werkhoven CH, van Elden LJ, Thijsen SF, Hoepelman AI, Kluytmans JA, Boersma WG, Compaijen CJ, van der Wall E, Prins JM, Oosterheert JJ, Bonten MJ (2015) Antibiotic treatment strategies for community-acquired pneumonia in adults. N Engl J Med 372:1312–1323
Lee JH, Kim HJ, Kim YH (2017) Is beta-lactam plus macrolide more effective than beta-lactam plus fluoroquinolone among patients with severe community-acquired pneumonia?: a systemic review and meta-analysis. J Korean Med Sci 32:77–84
Prina E, Ranzani OT, Polverino E, Cilloniz C, Ferrer M, Fernandez L, Puig de la Bellacasa J, Menendez R, Mensa J, Torres A (2015) Risk factors associated with potentially antibiotic-resistant pathogens in community-acquired pneumonia. Ann Am Thorac Soc 12:153–160
Waterer G (2017) Severity scores and community-acquired pneumonia. Time to move forward. Am J Respir Crit Care Med 196:1236–1238
Chalmers JD, Mandal P, Singanayagam A, Akram AR, Choudhury G, Short PM, Hill AT (2011) Severity assessment tools to guide ICU admission in community-acquired pneumonia: systematic review and meta-analysis. Intensive Care Med 37:1409–1420
Waterer GW, Self WH, Courtney DM, Grijalva CG, Balk RA, Girard TD, Fakhran SS, Trabue C, McNabb P, Anderson EJ, Williams DJ, Bramley AM, Jain S, Edwards KM, Wunderink RG (2018) In-hospital deaths among adults with community-acquired pneumonia. Chest 154:628–635
Chalmers JD, Taylor JK, Mandal P, Choudhury G, Singanayagam A, Akram AR, Hill AT (2011) Validation of the Infectious Diseases Society of America/American Thoratic Society minor criteria for intensive care unit admission in community-acquired pneumonia patients without major criteria or contraindications to intensive care unit care. Clin Infect Dis 53:503–511
Charles PG, Davis JS, Grayson ML (2009) Rocket science and the Infectious Diseases Society of America/American Thoracic Society (IDSA/ATS) guidelines for severe community-acquired pneumonia. Clin Infect Dis 48:1796 (author reply 1796–1797)
Wunsch H, Angus DC, Harrison DA, Linde-Zwirble WT, Rowan KM (2011) Comparison of medical admissions to intensive care units in the United States and United Kingdom. Am J Respir Crit Care Med 183:1666–1673
Lim HF, Phua J, Mukhopadhyay A, Ngerng WJ, Chew MY, Sim TB, Kuan WS, Mahadevan M, Lim TK (2014) IDSA/ATS minor criteria aid pre-intensive care unit resuscitation in severe community-acquired pneumonia. Eur Respir J 43:852–862
Salih W, Schembri S, Chalmers JD (2014) Simplification of the IDSA/ATS criteria for severe CAP using meta-analysis and observational data. Eur Respir J 43:842–851
Charles PG, Wolfe R, Whitby M, Fine MJ, Fuller AJ, Stirling R, Wright AA, Ramirez JA, Christiansen KJ, Waterer GW, Pierce RJ, Armstrong JG, Korman TM, Holmes P, Obrosky DS, Peyrani P, Johnson B, Hooy M, Grayson ML (2008) SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis 47:375–384
Ebrahimi F, Giaglis S, Hahn S, Blum CA, Baumgartner C, Kutz A, van Breda SV, Mueller B, Schuetz P, Christ-Crain M, Hasler P (2018) Markers of neutrophil extracellular traps predict adverse outcome in community-acquired pneumonia: secondary analysis of a randomised controlled trial. Eur Respir J 51:1701389
Mendez R, Menendez R, Cilloniz C, Amara-Elori I, Amaro R, Gonzalez P, Posadas T, Gimeno A, Espana PP, Almirall J, Torres A (2018) Initial inflammatory profile in community-acquired pneumonia depends on time since onset of symptoms. Am J Respir Crit Care Med 198:370–378
Singanayagam A, Chalmers JD (2013) Severity assessment scores to guide empirical use of antibiotics in community acquired pneumonia. Lancet Respir Med 1:653–662
Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG (2007) Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 44(Suppl 2):S27–S72
Webb BJ, Dascomb K, Stenehjem E, Dean N (2015) Predicting risk of drug-resistant organisms in pneumonia: moving beyond the HCAP model. Respir Med 109:1–10
Hariri G, Tankovic J, Boelle PY, Dubee V, Leblanc G, Pichereau C, Bourcier S, Bige N, Baudel JL, Galbois A, Ait-Oufella H, Maury E (2017) Are third-generation cephalosporins unavoidable for empirical therapy of community-acquired pneumonia in adult patients who require ICU admission? A retrospective study. Ann Intensive Care 7:35
Rodrigo-Troyano A, Sibila O (2017) The respiratory threat posed by multidrug resistant Gram-negative bacteria. Respirology (Carlton, Vic) 22:1288–1299
Shindo Y, Ito R, Kobayashi D, Ando M, Ichikawa M, Shiraki A, Goto Y, Fukui Y, Iwaki M, Okumura J, Yamaguchi I, Yagi T, Tanikawa Y, Sugino Y, Shindoh J, Ogasawara T, Nomura F, Saka H, Yamamoto M, Taniguchi H, Suzuki R, Saito H, Kawamura T, Hasegawa Y (2013) Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med 188:985–995
Maruyama T, Fujisawa T, Ishida T, Ito A, Oyamada Y, Fujimoto K, Yoshida M, Maeda H, Miyashita N, Nagai H, Imamura Y, Shime N, Suzuki S, Amishima M, Higa F, Kobayashi H, Suga S, Tsutsui K, Kohno S, Brito V, Niederman MS (2018) A therapeutic strategy for all pneumonia patients: a 3-year prospective multicenter- cohort study using risk factors for multidrug resistant pathogens to select initial empiric therapy. Clin Infect Dis
Ishida T, Ito A, Washio Y, Yamazaki A, Noyama M, Tokioka F, Arita M (2017) Risk factors for drug-resistant pathogens in immunocompetent patients with pneumonia: evaluation of PES pathogens. J Infect Chemother 23:23–28
Torres A, Cilloniz C, Ferrer M, Gabarrus A, Polverino E, Villegas S, Marco F, Mensa J, Menendez R, Niederman M (2015) Bacteraemia and antibiotic-resistant pathogens in community acquired pneumonia: risk and prognosis. Eur Respir J 45:1353–1363
Restrepo MI, Babu BL, Reyes LF, Chalmers JD, Soni NJ, Sibila O, Faverio P, Cilloniz C, Rodriguez-Cintron W, Aliberti S (2018) Burdenand risk factors for Pseudomonas aeruginosa community-acquired pneumonia: a multinational point prevalence study of hospitalised patients. Eur Respir J 52:1701190
Aliberti S, Reyes LF, Faverio P, Sotgiu G, Dore S, Rodriguez AH, Soni NJ, Restrepo MI (2016) Global initiative for meticillin-resistant Staphylococcus aureus pneumonia (GLIMP): an international, observational cohort study. Lancet Infect Dis 16:1364–1376
Martin-Loeches I, Schultz MJ, Vincent JL, Alvarez-Lerma F, Bos LD, Sole-Violan J, Torres A, Rodriguez A (2017) Increased incidence of co-infection in critically ill patients with influenza. Intensive Care Med 43:48–58
Piralla A, Rovida F, Girello A, Premoli M, Mojoli F, Belliato M, Braschi A, Iotti G, Pariani E, Bubba L, Zanetti AR, Baldanti F (2017) Frequency of respiratory virus infections and next-generation analysis of influenza A/H1N1pdm09 dynamics in the lower respiratory tract of patients admitted to the ICU. PLoS ONE 12:e0178926
Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, Spencer EA, Onakpoya I, Mahtani KR, Nunan D, Howick J, Heneghan CJ (2014) Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev 132:Cd008965
Jefferson T, Jones M, Doshi P, Spencer EA, Onakpoya I, Heneghan CJ (2014) Oseltamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ 348:g2545
Heneghan CJ, Onakpoya I, Thompson M, Spencer EA, Jones M, Jefferson T (2014) Zanamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ 348:g2547
Dobson J, Whitley RJ, Pocock S, Monto AS (2015) Oseltamivir treatment for influenza in adults: a meta-analysis of randomised controlled trials. Lancet (London, England) 385:1729–1737
Lackenby A, Besselaar TG, Daniels RS, Fry A, Gregory V, Gubareva LV, Huang W, Hurt AC, Leang SK, Lee RTC, Lo J, Lollis L, Maurer-Stroh S, Odagiri T, Pereyaslov D, Takashita E, Wang D, Zhang W, Meijer A (2018) Global update on the susceptibility of human influenza viruses to neuraminidase inhibitors and status of novel antivirals, 2016–2017. Antiviral Res 157:38–46
Torres A, Sibila O, Ferrer M, Polverino E, Menendez R, Mensa J, Gabarrus A, Sellares J, Restrepo MI, Anzueto A, Niederman MS, Agusti C (2015) Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA 313:677–686
Stern A, Skalsky K, Avni T, Carrara E, Leibovici L, Paul M (2017) Corticosteroids for pneumonia. Cochrane Database Syst Rev 12:Cd007720
Mc Mahon A, Martin-Loeches I (2017) The pharmacological management of severe influenza infection—’existing and emerging therapies’. Expert Rev Clin Pharmacol 10:81–95
Moreno G, Rodriguez A, Reyes LF, Gomez J, Sole-Violan J, Diaz E, Bodi M, Trefler S, Guardiola J, Yebenes JC, Soriano A, Garnacho-Montero J, Socias L, Del Valle Ortiz M, Correig E, Marin-Corral J, Vallverdu-Vidal M, Restrepo MI, Torres A, Martin-Loeches I (2018) Corticosteroid treatment in critically ill patients with severe influenza pneumonia: a propensity score matching study. Intensive Care Med 44:1470–1482
Martin-Loeches I, Soares M, Torres A (2016) Neces-SARI-ly? Intensive Care Med 42:928–930
Marty FM, Vidal-Puigserver J, Clark C, Gupta SK, Merino E, Garot D, Chapman MJ, Jacobs F, Rodriguez-Noriega E, Husa P, Shortino D, Watson HA, Yates PJ, Peppercorn AF (2017) Intravenous zanamivir or oral oseltamivir for hospitalised patients with influenza: an international, randomised, double-blind, double-dummy, phase 3 trial. Lancet Respir Med 5:135–146
Murphy TF (2008) Placebo-controlled trials of treatments for community-acquired pneumonia: review of the literature and discussion of feasibility and potential value. Clin Infect Dis 47(Suppl 3):S145–S149
Kmietowicz Z (2014) Critics attack chief medical officer’s advice to use antivirals for flu. BMJ 348:g1496
Leroy O, Saux P, Bedos JP, Caulin E (2005) Comparison of levofloxacin and cefotaxime combined with ofloxacin for ICU patients with community-acquired pneumonia who do not require vasopressors. Chest 128:172–183
Ferrer M, Travierso C, Cilloniz C, Gabarrus A, Ranzani OT, Polverino E, Liapikou A, Blasi F, Torres A (2018) Severe community-acquired pneumonia: characteristics and prognostic factors in ventilated and non-ventilated patients. PLoS ONE 13:e0191721
De la Calle C, Ternavasio-de la Vega HG, Morata L, Marco F, Cardozo C, Garcia-Vidal C, Del Rio A, Cilloniz C, Torres A, Martinez JA, Mensa J, Soriano A (2018) Effectiveness of combination therapy versus monotherapy with a third-generation cephalosporin in bacteraemic pneumococcal pneumonia: a propensity score analysis. J Infect 76:342–347
Garin N, Genne D, Carballo S, Chuard C, Eich G, Hugli O, Lamy O, Nendaz M, Petignat PA, Perneger T, Rutschmann O, Seravalli L, Harbarth S, Perrier A (2014) beta-Lactam monotherapy vs. beta-lactam-macrolide combination treatment in moderately severe community-acquired pneumonia: a randomized noninferiority trial. JAMA Internal Med 174:1894–1901
Anderson R, Steel HC, Cockeran R, Smith AM, von Gottberg A, de Gouveia L, Brink A, Klugman KP, Mitchell TJ, Feldman C (2007) Clarithromycin alone and in combination with ceftriaxone inhibits the production of pneumolysin by both macrolide-susceptible and macrolide-resistant strains of Streptococcus pneumoniae. J Antimicrob Chemother 59:224–229
Bonten MJ, Huijts SM, Bolkenbaas M, Webber C, Patterson S, Gault S, van Werkhoven CH, van Deursen AM, Sanders EA, Verheij TJ, Patton M, McDonough A, Moradoghli-Haftvani A, Smith H, Mellelieu T, Pride MW, Crowther G, Schmoele-Thoma B, Scott DA, Jansen KU, Lobatto R, Oosterman B, Visser N, Caspers E, Smorenburg A, Emini EA, Gruber WC, Grobbee DE (2015) Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 372:1114–1125
Gershengorn HB, Keene A, Dzierba AL, Wunsch H (2015) The association of antibiotic treatment regimen and hospital mortality in patients hospitalized with Legionella pneumonia. Clin Infect Dis 60:e66–e79
Griffin AT, Peyrani P, Wiemken TL, Ramirez JA, Arnold FW (2013) Empiric therapy directed against MRSA in patients admitted to the intensive care unit does not improve outcomes in community-acquired pneumonia. Infection 41:517–523
Gillet Y, Vanhems P, Lina G, Bes M, Vandenesch F, Floret D, Etienne J (2007) Factors predicting mortality in necrotizing community-acquired pneumonia caused by Staphylococcus aureus containing Panton-Valentine leukocidin. Clin Infect Dis 45:315–321
Sicot N, Khanafer N, Meyssonnier V, Dumitrescu O, Tristan A, Bes M, Lina G, Vandenesch F, Vanhems P, Etienne J, Gillet Y (2013) Methicillin resistance is not a predictor of severity in community-acquired Staphylococcus aureus necrotizing pneumonia–results of a prospective observational study. Clin Microb Infect 19:E142–E148
File TM Jr, Low DE, Eckburg PB, Talbot GH, Friedland HD, Lee J, Llorens L, Critchley I, Thye D (2010) Integrated analysis of FOCUS 1 and FOCUS 2: randomized, doubled-blinded, multicenter phase 3 trials of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in patients with community-acquired pneumonia. Clin Infect Dis 51:1395–1405
Harris PNA, Tambyah PA, Lye DC, Mo Y, Lee TH, Yilmaz M, Alenazi TH, Arabi Y, Falcone M, Bassetti M, Righi E, Rogers BA, Kanj S, Bhally H, Iredell J, Mendelson M, Boyles TH, Looke D, Miyakis S, Walls G, Al Khamis M, Zikri A, Crowe A, Ingram P, Daneman N, Griffin P, Athan E, Lorenc P, Baker P, Roberts L, Beatson SA, Peleg AY, Harris-Brown T, Paterson DL (2018) Effect of piperacillin-tazobactam vs. meropenem on 30-day mortality for patients with e coli or klebsiella pneumoniae bloodstream infection and ceftriaxone resistance: a randomized clinical trial. JAMA 320:984–994
Walden AP, Clarke GM, McKechnie S, Hutton P, Gordon AC, Rello J, Chiche JD, Stueber F, Garrard CS, Hinds CJ (2014) Patients with community acquired pneumonia admitted to European intensive care units: an epidemiological survey of the GenOSept cohort. Crit Care 18:R58
Hadfield J, Bennett L (2018) Determining best outcomes from community-acquired pneumonia and how to achieve them. Respirology (Carlton, Vic) 23:138–147
Siow WT, Koay ES, Lee CK, Lee HK, Ong V, Ngerng WJ, Lim HF, Tan A, Tang JW, Phua J (2016) The use of polymerase chain reaction amplification for the detection of viruses and bacteria in severe community-acquired pneumonia. Respir Int Rev Thorac Dis 92:286–294
Seymour CW, Kahn JM, Martin-Gill C, Callaway CW, Yealy DM, Scales D, Angus DC (2017) Delays from first medical contact to antibiotic administration for sepsis. Crit Care Med 45:759–765
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP (2017) Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 43:304–377
Howell MD, Davis AM (2018) Management of ARDS in adults. JAMA 319:711–712
Venkatesh B, Finfer S, Cohen J, Rajbhandari D, Arabi Y, Bellomo R, Billot L, Correa M, Glass P, Harward M, Joyce C, Li Q, McArthur C, Perner A, Rhodes A, Thompson K, Webb S, Myburgh J (2018) Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 378:797–808
Annane D, Renault A, Brun-Buisson C, Megarbane B, Quenot JP, Siami S, Cariou A, Forceville X, Schwebel C, Martin C, Timsit JF, Misset B, Ali Benali M, Colin G, Souweine B, Asehnoune K, Mercier E, Chimot L, Charpentier C, Francois B, Boulain T, Petitpas F, Constantin JM, Dhonneur G, Baudin F, Combes A, Bohe J, Loriferne JF, Amathieu R, Cook F, Slama M, Leroy O, Capellier G, Dargent A, Hissem T, Maxime V, Bellissant E (2018) Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med 378:809–818
Sprung CL, Annane D, Keh D, Moreno R, Singer M, Freivogel K, Weiss YG, Benbenishty J, Kalenka A, Forst H, Laterre PF, Reinhart K, Cuthbertson BH, Payen D, Briegel J (2008) Hydrocortisone therapy for patients with septic shock. N Engl J Med 358:111–124
Annane D, Sebille V, Charpentier C, Bollaert PE, Francois B, Korach JM, Capellier G, Cohen Y, Azoulay E, Troche G, Chaumet-Riffaud P, Bellissant E (2002) Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 288:862–871
Keh D, Trips E, Marx G, Wirtz SP, Abduljawwad E, Bercker S, Bogatsch H, Briegel J, Engel C, Gerlach H, Goldmann A, Kuhn SO, Huter L, Meier-Hellmann A, Nierhaus A, Kluge S, Lehmke J, Loeffler M, Oppert M, Resener K, Schadler D, Schuerholz T, Simon P, Weiler N, Weyland A, Reinhart K, Brunkhorst FM, SepNet-Critical Care Trials G (2016) Effect of hydrocortisone on development of shock among patients with severe sepsis: the HYPRESS randomized clinical trial. JAMA 316:1775–1785
Gibbison B, Lopez-Lopez JA, Higgins JP, Miller T, Angelini GD, Lightman SL, Annane D (2017) Corticosteroids in septic shock: a systematic review and network meta-analysis. Crit Care 21:78
Cheng M, Pan ZY, Yang J, Gao YD (2014) Corticosteroid therapy for severe community-acquired pneumonia: a meta-analysis. Respir Care 59:557–563
Briel M, Spoorenberg SMC, Snijders D, Torres A, Fernandez-Serrano S, Meduri GU, Gabarrus A, Blum CA, Confalonieri M, Kasenda B, Siemieniuk RAC, Boersma W, Bos WJW, Christ-Crain M (2018) Corticosteroids in Patients hospitalized with community-acquired pneumonia: systematic review and individual patient data metaanalysis. Clin Infect Dis 66:346–354
Wu WF, Fang Q, He GJ (2018) Efficacy of corticosteroid treatment for severe community-acquired pneumonia: a meta-analysis. Am J Emerg Med 36:179–184
Siempos II, Vardakas KZ, Kopterides P, Falagas ME (2008) Adjunctive therapies for community-acquired pneumonia: a systematic review. J Antimicrob Chemother 62:661–668
Nie W, Zhang Y, Cheng J, Xiu Q (2012) Corticosteroids in the treatment of community-acquired pneumonia in adults: a meta-analysis. PLoS ONE 7:e47926
Siemieniuk RA, Meade MO, Alonso-Coello P, Briel M, Evaniew N, Prasad M, Alexander PE, Fei Y, Vandvik PO, Loeb M, Guyatt GH (2015) Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med 163:519–528
Horita N, Otsuka T, Haranaga S, Namkoong H, Miki M, Miyashita N, Higa F, Takahashi H, Yoshida M, Kohno S, Kaneko T (2015) Adjunctive systemic corticosteroids for hospitalized community-acquired pneumonia: systematic review and meta-analysis 2015 update. Sci Rep 5:14061
Marti C, Grosgurin O, Harbarth S, Combescure C, Abbas M, Rutschmann O, Perrier A, Garin N (2015) Adjunctive corticotherapy for community acquired pneumonia: a systematic review and meta-analysis. PLoS ONE 10:e0144032
Wan YD, Sun TW, Liu ZQ, Zhang SG, Wang LX, Kan QC (2016) Efficacy and safety of corticosteroids for community-acquired pneumonia: a systematic review and meta-analysis. Chest 149:209–219
Rodrigo C, Leonardi-Bee J, Nguyen-Van-Tam J, Lim WS (2016) Corticosteroids as adjunctive therapy in the treatment of influenza. Cochrane Database Syst Rev 3:Cd010406
Sibila O, Rodrigo-Troyano A, Torres A (2016) Nonantibiotic adjunctive therapies for community-acquired pneumonia (corticosteroids and beyond): where are we with them? Semin Respir Crit Care Med 37:913–922
Iannini PB, Paladino JA, Lavin B, Singer ME, Schentag JJ (2007) A case series of macrolide treatment failures in community acquired pneumonia. J Chemother (Florence, Italy) 19:536–545
Cilloniz C, Albert RK, Liapikou A, Gabarrus A, Rangel E, Bello S, Marco F, Mensa J, Torres A (2015) The effect of macrolide resistance on the presentation and outcome of patients hospitalized for Streptococcus pneumoniae pneumonia. Am J Respir Crit Care Med 191:1265–1272
Yin YD, Wang R, Zhuo C, Wang H, Wang MG, Xie CM, She DY, Yuan X, Wang RT, Cao B, Liu YN (2017) Macrolide-resistant Mycoplasma pneumoniae prevalence and clinical aspects in adult patients with community-acquired pneumonia in China: a prospective multicenter surveillance study. J Thorac Dis 9:3774–3781
Mendes RE, Farrell DJ, Flamm RK, Talbot GH, Ivezic-Schoenfeld Z, Paukner S, Sader HS (2016) In vitro activity of lefamulin tested against Streptococcus pneumoniae with defined serotypes, including multidrug-resistant isolates causing lower respiratory tract infections in the united states. Antimicrob Agents Chemother 60:4407–4411
Pfaller MA, Sader HS, Rhomberg PR, Flamm RK (2017) In vitro activity of delafloxacin against contemporary bacterial pathogens from the United States and Europe, 2014. Antimicrob Agents Chemother 61:AAC-02609
Donald BJ, Surani S, Deol HS, Mbadugha UJ, Udeani G (2017) Spotlight on solithromycin in the treatment of community-acquired bacterial pneumonia: design, development, and potential place in therapy. Drug Des Dev Ther 11:3559–3566
Liu Y, Zhang Y, Wu J, Zhu D, Sun S, Zhao L, Wang X, Liu H, Ren Z, Wang C, Xiu Q, Xiao Z, Cao Z, Cui S, Yang H, Liang Y, Chen P, Lv Y, Hu C, Lv X, Liu S, Kuang J, Li J, Wang D, Chang L (2017) A randomized, double-blind, multicenter Phase II study comparing the efficacy and safety of oral nemonoxacin with oral levofloxacin in the treatment of community-acquired pneumonia. J Microbiol Immunol Infect Wei mian yu gan ran za zhi 50:811–820
Amalakuhan B, Echevarria KL, Restrepo MI (2017) Managing community acquired pneumonia in the elderly—the next generation of pharmacotherapy on the horizon. Expert Opin Pharmacother 18:1039–1048
Carreno JJ, Lodise TP (2014) Ceftaroline fosamil for the treatment of community-acquired pneumonia: from FOCUS to CAPTURE. Infect Dis Ther 3:123–132
Author information
Authors and Affiliations
Author notes
Antoni Torres, James D. Chalmers, Charles S. Dela Cruz, Cristina Dominedò, Marin Kollef, Ignacio Martin-Loeches, Michael Niederman and Richard G. Wunderink contributed equally to this manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
Professor Torres is consultant for Pfizer, Bayer, Roche, MSD, Polyphor. Professor Chalmers reports grants and personal fees from Glaxosmithkline, grants and personal fees from Boehringer-Ingelheim, grants from Astrazeneca, grants and personal fees from Pfizer, grants and personal fees from Bayer Healthcare, grants and personal fees from Grifols, personal fees from Napp, personal fees from Aradigm corporation, grants and personal fees from Insmed, outside the submitted work. Professor Dela Cruz declares no conflict of interest. Doctor Dominedò declares no conflict of interest. Professor Kollef was supported by the Barnes-Jewish Hospital Foundation. Doctor Martin-Loeches declares no conflict of interest. Professor Niederman is consultant for Pfizer, Merck, Paratek and Melinta. Professor Wunderink is consultant for Nabriva, Melinta, bioMerieux, Curetis, Genmark, Accelerate.
Ethical approval
An approval by an ethics committee was not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Torres, A., Chalmers, J.D., Dela Cruz, C.S. et al. Challenges in severe community-acquired pneumonia: a point-of-view review. Intensive Care Med 45, 159–171 (2019). https://doi.org/10.1007/s00134-019-05519-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-019-05519-y