
Abstract
Purpose
The purpose of the present study is to describe the use of tracheostomy, specifically frequency, timing (in relation to initiation of mechanical ventilation), and associated factors, in a large cohort of children admitted to North American pediatric intensive care units (PICUs) and requiring prolonged mechanical ventilation.
Methods
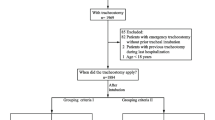
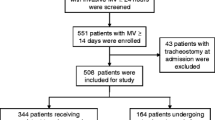
This was a retrospective cohort study. De-identified data were obtained from the VPSLLC database, a multi-site, clinical PICU database. Admissions between 1 July 2009 and 30 June 2011 were enrolled in the study if the patient required mechanical ventilation for at least 72 h and did not have a tracheostomy tube at initiation of mechanical ventilation.
Results
A total of 13,232 PICU admissions from 82 PICUs were analyzed in the study; of these, 872 (6.6 %) had a tracheostomy tube inserted after initiation of mechanical ventilation. The rate varied significantly (0–13.4 %, p < 0.001) among the 45 PICUs that had 100 or more admissions included in the study. The median time to insertion of a tracheostomy tube was 14.4 days (IQR 7.4–25.7), and it also varied significantly by unit (4.3–30.4 days, p < 0.001) among those that performed at least ten tracheostomies included in the study.
Conclusions
There is significant variation in both the frequency and time to tracheostomy between the studied PICUs for patients requiring prolonged mechanical ventilation; among those who received a tracheostomy, the majority did so after two or more weeks of mechanical ventilation. Future studies examining tracheostomy benefits, disadvantages, outcomes, and resource utilization of this patient subgroup are indicated.



Similar content being viewed by others

References
Esteban A, Anzueto A, Alia I et al (2000) How is mechanical ventilation employed in the intensive care unit? Am J Respir Crit Care Med 161:1450–1458. doi:10.1164/ajrccm.161.5.9902018
Nathens AB, Rivara FP, Mack CD et al (2006) Variations in rates of tracheostomy in the critically ill trauma patient. Crit Care Med 34:2919–2924. doi:10.1097/01.CCM.0000243800.28251.AE
Blot F, Similowski T, Trouillet JL et al (2008) Early tracheotomy versus prolonged endotracheal intubation in unselected severely ill ICU patients. Intensive Care Med 34:1779–1787. doi:10.1007/s00134-008-1195-4
Nieszkowska A, Combes A, Luyt CE et al (2005) Impact of tracheotomy on sedative administration, sedation level, and comfort of mechanically ventilated intensive care unit patients. Crit Care Med 33:2527–2533. doi:10.1097/01.CCM.0000186898.58709.AA
Combes A, Luyt CE, Nieszkowska A et al (2007) Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation? Crit Care Med 35:802–807. doi:10.1097/01.CCM.0000256721.60517.B1
Young D, Harrison DA, Cuthbertson BH, Rowan K, TracMan Collaborators (2013) Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA 309:2121–2129. doi:10.1001/jama.2013.5154
Durbin CG Jr (2010) Tracheostomy: why, when, and how? Respir Care 55:1056–1068
Durbin CG Jr, Perkins MP, Moores LK (2010) Should tracheostomy be performed as early as 72 hours in patients requiring prolonged mechanical ventilation? Respir Care 55:76–87
Scales DC (2013) What’s new with tracheostomy? Intensive Care Med 39:1005–1008. doi:10.1007/s00134-013-2904-1
Freeman BD, Morris PE (2012) Tracheostomy practice in adults with acute respiratory failure. Crit Care Med 40:2890–2896. doi:10.1097/CCM.0b013e31825bc948
Freeman BD, Borecki IB, Coopersmith CM, Buchman TG (2005) Relationship between tracheostomy timing and duration of mechanical ventilation in critically ill patients. Crit Care Med 33:2513–2520. doi:10.1097/01.CCM.0000186369.91799.44
Clec’h C, Alberti C, Vincent F et al (2007) Tracheostomy does not improve the outcome of patients requiring prolonged mechanical ventilation: a propensity analysis. Crit Care Med 35:132–138. doi:10.1097/01.CCM.0000251134.96055.A6
Berry JG, Graham RJ, Roberson DW et al (2010) Patient characteristics associated with in-hospital mortality in children following tracheotomy. Arch Dis Child 95:703–710. doi:10.1136/adc.2009.180836
Mahadevan M, Barber C, Salkeld L, Douglas G, Mills N (2007) Pediatric tracheotomy: 17-year review. Int J Pediatr Otorhinolaryngol 71:1829–1835. doi:10.1016/j.ijporl.2007.08.007
Dursen O, Ozel D (2011) Early and long-term outcome after tracheostomy in children. Pediatr Int 53:202–206. doi:10.1111/j.1442-200X.2010.03208.x
Lee W, Koltai P, Harrison AM et al (2002) Indications for tracheotomy in the pediatric intensive care unit population. Arch Otolaryngal Head Neck Surg 128:1249–1252. doi:10.1001/archotol.128.11.12
Zenk J, Fyrmpas G, Zimmerman T, Koch M, Contantinidis J, Iro H (2009) Tracheostomy in young patients: indications and long-term outcome. Eur Arch Otorhinolaryngol 266:705–711. doi:10.1007/s00405-008-0796-4
Graf JM, Montagnino BA, Hueckel R, McPherson ML (2008) Pediatric tracheostomies: a recent experience from one academic center. Pediatr Crit Care Med 9:96–100. doi:10.1097/01.PCC.0000298641.84257.53
Lewis CW, Carron JD, Perkins JA, Sie KCY, Feudtner C (2003) Tracheotomy in pediatric patients. Arch Otolaryngol Head Neck Sur 129:523–529. doi:10.1001/archotol.129.5.523
Wood D, McShane P, Davis P (2012) Tracheostomy in children admitted to paediatric intensive care. Arch Dis Child 97:866–869. doi:10.1136/archdischild-2011-301494
Principi T, Morrison GC, Matsui DM et al (2008) Elective tracheostomy in mechanically ventilated children in Canada. Instensive Care Med 34:1498–1502. doi:10.1007/s00134-008-1104-x
Berry JG, Graham DA, Graham RJ et al (2009) Predictors of clinical outcomes and hospital resource use of children after tracheotomy. Pediatrics 124:563–572. doi:10.1542/peds.2008-3491
Acknowledgments
VPS data was provided by the VPSLLC. No endorsement or editorial restriction of the interpretation of these data or opinions of the authors has been implied or stated. The authors have no financial relationships relevant to this article to disclose. The only potential financial relationship is the clinical consultation that Dr. Scanlon has performed in the development of the VPS database. Dr. Scanlon, a salaried employee of the non-profit Medical College of Wisconsin, received no direct compensation for his work. The Medical College of Wisconsin was directly compensated for Dr. Scanlon’s efforts by the VPSLLC.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Take-home message: Demographic and clinical characteristics are associated with the frequency and timing of tracheostomy among PICU patients requiring prolonged mechanical ventilation. Independent of these characteristics, there is significant variation among the studied PICUs. These findings are important because decreasing non-value-added variability of practice represents a potential opportunity for quality improvement; however, in order to drive the direction of such efforts, studies examining tracheostomy benefits, disadvantages, and outcomes, including quality of life and resource utilization of this patient subgroup, are needed.
Rights and permissions
About this article

Cite this article
Wakeham, M.K., Kuhn, E.M., Lee, K.J. et al. Use of tracheostomy in the PICU among patients requiring prolonged mechanical ventilation. Intensive Care Med 40, 863–870 (2014). https://doi.org/10.1007/s00134-014-3298-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-014-3298-4