
Abstract
Aim/hypothesis
Postpandrial hyperglycaemia is a significant risk factor for the development of macrovascular diseases. There is no clear agreement in the field whether these alterations result from hyperglycaemic episodes or from exaggerated alterations (‘glycaemic swings’) in blood glucose. We compared the effect of stable high glucose with a model of poorly maintained insulin-controlled diabetes (on average lower glucose, but with large glycaemic swings) on the development of endothelial dysfunction in rats.
Methods
Intermediate- or long-acting insulin was used to reduce mean blood glucose levels. One group of animals had stable low glucose levels, while animals in the other group exhibited rapid changes (‘swings’) in their blood glucose concentration. Acetylcholine-induced endothelium-dependent vascular relaxation of the thoracic aorta was measured. Immunohistochemistry, western blot analysis and flow cytometry were used to determine nitrotyrosine formation and poly(ADP-ribose) accumulation in the aorta, in circulating leucocytes and in bone marrow cells.
Results
Steady normalisation of blood glucose levels (a model of well-controlled diabetes) protected against the development of endothelial dysfunction, poly(ADP-ribose) polymerase (PARP) activation and nitrotyrosine production. However, impairment of endothelium-dependent relaxation was found in the animals undergoing glycaemic swings, even though the fructosamine levels in these animals were lower than in the untreated diabetic rats. This was associated with elevated PARP activation in the aorta and in bone marrow cells that was similar to or even more pronounced than that seen in the untreated diabetic animals.
Conclusions/interpretation
Large glycaemic swings exert deleterious cardiovascular effects in diabetes mellitus, in part via enhanced activation of the PARP pathway.
Similar content being viewed by others


Introduction
Micro- and macrovascular disease remains a worldwide problem responsible for the higher morbidity and mortality of type 1 and type 2 diabetic patients. Postprandial hyperglycaemia is a strong and independent risk factor for the development of macrovascular diseases, not only in diabetic patients but also in individuals with impaired glucose tolerance, and even in healthy individuals [1–5]. Although marked postprandial hyperglycaemia is a typical feature of diabetes, it is not necessarily reflected in plasma fructosamine or HbA1c levels [6–9]. While it is known that postprandial plasma glucose spikes are important factors in the development of vascular complications and reduced beta cell function in diabetes [8], the underlying cellular and molecular mechanisms are incompletely understood.
Reactive oxygen and nitrogen species contribute to the development of various complications of diabetes mellitus (DM), among others, macrovascular diseases [10–16]. In response to hyperglycaemia or diabetes, or its in vitro model (high glucose concentration in endothelial cells) the generation of multiple reactive oxygen and nitrogen species occurs. Superoxide reacts with nitric oxide (NO) to form the toxic oxidant peroxynitrite. A characteristic reaction of peroxynitrite and related reactive nitrogen species is the nitration of protein tyrosine residues [11, 13, 17]. Peroxynitrite and hydroxyl radicals are potent inducers of DNA single-strand breakage. DNA single-strand breakage is the obligatory trigger of the activation of the nuclear enzyme poly(ADP-ribose) polymerase (PARP). PARP uses NAD+ as a substrate to form poly(ADP-ribose) (PAR), and plays a role in numerous physiological mechanisms such as DNA repair, regulation of genomic stability, gene expression etc. The enzyme also PARylates itself in an automodification reaction; auto-PARylation of PARP-1 represents a major regulatory mechanism. While auto-PARylation is necessary for the recruitment of DNA repair enzymes [18], by electrostatic repulsion it inhibits DNA binding [19] and downregulates enzyme activity [20]. As PARP uses NAD+ as substrate, overactivation may result in rapid depletion of intracellular NAD+ and ATP, leading to cell dysfunction and necrotic cell death [11, 13, 17, 20]. Peroxynitrite formation and PARP activation play important roles in the pathogenesis of diabetic complications [11–13, 21].
In cultured human umbilical endothelial cells, oscillating glucose triggers a higher degree of peroxynitrite generation than stable high glucose [22]. In the present study we compared stable high glucose with on the average lower, but rapidly changing, blood glucose (modelled by inducing insulin-mediated rapid ‘glycaemic swings’) with respect to their ability to induce endothelial dysfunction in diabetic rats. We have examined whether correlation exists between the dynamics of blood glucose level, arterial dysfunction and oxidative–nitrosative stress and PARP activation in the vessel wall. We have also tested whether there are signs of nitrosative stress and PARP activation in circulating leucocytes and bone marrow cells. The results of the current study are consistent with the notion that in the current experimental model large glycaemic swings associated with insulin therapy are more deleterious than steadily elevated glucose levels, and these deleterious effects are a consequence of increased PARP activation.
Methods
All investigations conformed to the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health (NIH Publication No. 85-23, Revised 1985), and were approved by the local Animal Use Committee.
Animals
Nineteen age-matched male Wistar rats (Toxicoop, Budapest, Hungary) weighing 380-480 g were administered 70 mg/kg streptozotocin (STZ) i.v. From the 14th day we started insulin therapy: the first group received 60 U/kg of intermediate-acting (lente) glargine insulin (Sanofi Aventis, Paris, France) s.c. daily, every afternoon at 17:00 hours (DM with good glycaemic control [DM-GGC] animals, n = 6). The second group was treated with 60 U/kg long-acting (ultralente) insulin (Novo Nordisk, Bagsvaerd, Denmark) s.c. on every second day at 17:00 hours (DM with poor glycaemic control [DM-PGC] animals, n = 7). Six diabetic animals were left untreated (DM group). The age-matched control group received the vehicle of the drugs (control, n = 7; Fig. 1).

Experimental protocol. The control group received only the vehicle of the drugs. In order to induce DM, male Wistar rats were administered a single dose of 70 mg/kg STZ i.v., followed by repeated vehicle injections. The DM group in which GGC was simulated (DM-GGC), received 60 U/kg of lente insulin s.c., daily, starting on the 14th day. In the DM group in which PGC of diabetes was simulated (DM-PGC), animals received ultralente insulin at 60 U/kg s.c., every second day. Two weeks after the start of insulin treatment (or corresponding vehicle), all rats were anaesthetised with i.p. injections of thiopental sodium and killed
After 10 days of insulin treatment, blood glucose levels of every rat were monitored for 48 h; the collection of samples started immediately before insulin dosage and was repeated every 6 h. The total glucose AUC was computed using the trapezoidal rule. After 2 weeks of insulin treatment, the rats were anaesthetised with i.p. thiopental sodium and were killed between 08:00 and 10:00 hours. (The DM-PGC rats were killed 1 day after insulin injection.) Thoracic aorta, blood and bone marrow were harvested for further measurements. Serum fructosamine concentration was determined by an enzymatic colorimetric assay (Boehringer Mannheim, Philadelphia, PA, USA). PARP activation was measured using methods based on the immunohistochemical detection of PAR.
Measurement of isometric force on aortic rings of rats
The method to determine endothelium-dependent vascular relaxation in thoracic aortic rings has been described previously [11]. Briefly, the thoracic aorta was cleared from periadventitial fat and cut into 2–3 mm width rings, mounted in organ baths filled with warmed (37°C) and oxygenated (95% O2, 5% CO2) Krebs solution (CaCl2 1.6 mmol/l; MgSO4 1.17 mmol/l; EDTA 0.026 mmol/l; NaCl 130 mmol/l; NaHCO3 14.9 mmol/l; KCl 4.7 mmol/l; KH2PO4 1.18 mmol/l; glucose 11 mmol/l). Isometric tension was measured with isometric transducers and registered (Kipp & Zonen BD300, Bohemia, NY, USA). A tension of 1 g was applied and the rings were equilibrated for 60 min. Fresh Krebs solution was provided at 20 min intervals. After equilibration the contractile response of arterial rings to a depolarising solution of a modified Krebs solution enriched in K+ was first tested to evaluate their functional integrity. Increasing doses of phenylephrine (10−8–3 × 10−5 mol/l) were used to determine contraction capability. For the measurement of endothelial functionality, rings were pre-contracted with phenylephrine (10−6 mol/l) and then dose–response curves to acetylcholine (1 × 10−8–3 × 10−5 mol/l) were constructed. Increasing doses of sodium nitroprusside (1 × 10−8–1 × 10−5 mol/l) were used to check NO-dependent vasodilatation. Experiments were conducted in eight to ten rings (four or five animals) in each experimental group. Contractile responses to phenylephrine were expressed as a percentage of K+-induced contractions. Relaxations were expressed as a percentage relative to the pre-contraction achieved by phenylephrine.
Flow cytometry
PARP activation in circulating cells was measured using a flow cytometric method based on the immunohistochemical detection of PAR, as described previously [23]. Briefly, circulating leucocytes were isolated from whole blood using Histopaque-1083 (Sigma, Saint Louis, MO, USA) according to the Users’ Manual. After the fixation and permeabilisation of the cells with a Cytofix/Cytoperm Fixation/Permeabilization Solution Kit (Becton Dickinson, San Jose, CA, USA), monoclonal mouse anti-PAR antibody (1:100, 30 min, 4°C; Tulip Biolabs, West Point, PA, USA) was used as primary antibody. After the fixation, all procedures were performed in Cytoperm solution (Becton Dickinson). Purified mouse IgG3κ isotype control (anti-keyhole limpet haemocyanin) antibody (Beckton Dickinson) served as isotype control. FITC-conjugated anti-mouse immunoglobulin specific polyclonal antibody (multiple absorptions) (1:500, 30 min, 4°C; Beckton Dickinson) was used as secondary antibody. Flow cytometry was performed on single-cell suspensions of rat leucocytes using a FACSCalibur (Becton Dickinson).
Region 1 (R1) was defined as containing cells having typical forward scatter and side scatter properties of lymphocytes. Isotype control-stained cells served as a negative control for each sample. Fluorescence data were collected using logarithmic amplification until we reached 10,000 counts of R1 cells. On the PAR histograms the gate was R1.
Western blot analysis
The aortas of the rats were dissected and homogenised using a Teflon homogeniser in protein lysis buffer containing 20 mmol/l TRIS–HCl (pH 7.5) and 1 mmol/l EGTA and 1 μl/ml protein inhibitor mix (Sigma). The homogenates were centrifuged at 700 g for 10 min at 4°C. The supernatant fraction was removed and used for western blot analysis. The same amount of protein (20 μg) was applied to each lane and confirmed with Ponceau-BS (Sigma) staining. Proteins were separated by 10–15% SDS-PAGE according to the manufacturers’ protocol (Invitrogen, Carlsbad, CA, USA). Following electrophoresis, proteins were transferred to an immobilon polyvinylidine fluoride (PVDF) membrane for 2 h at a constant 200 V, using an Xcell II blot module system (Invitrogen). After transfer, PVDF membranes were incubated with a blocking buffer consisting of TRIS-buffered saline (TBS) and 3% (wt/vol.) non-fat dry milk for 1 h at room temperature (RT), then washed with washing buffer (TBS/0.05% [vol./vol.] Tween 20). The membrane was incubated with primary antibody against PAR (monoclonal antibody; Calbiochem, San Diego, CA, USA, 1:2,000, overnight at 4°C). The membranes were then incubated with horseradish peroxidase-conjugated anti-mouse secondary antibodies at a dilution of 1:2,000 for 1 h at RT. The blots were then developed using the enhanced chemiluminescence method (Amersham, Arlington Heights, IL, USA). Densitometry was performed by ImageJ software (National Institutes of Health, Bethesda, MD, USA).
Immunohistochemistry
Anti-nitrotyrosine (NT) rabbit polyclonal antibody (Upstate Biotechnology, Lake Placid, NY, USA; 1:80, 4°C, overnight) was used to stain 3-nitrotyrosine, the marker of tyrosine nitration. The level of lipid peroxidation was estimated by using anti-4-hydroxy-2-noneal (HNE) rabbit polyclonal antibody (Calbiochem; 1:200, 4°C, overnight). The detection of PAR was performed by using mouse monoclonal anti-PAR antibody (Tulip Biolabs; 1:100, 4°C, overnight) after antigen retrieval (0.1 mol/l citrate buffer, pH 3, cooking in a microwave oven for 15 min). Non-specific labelling was avoided by incubating the sections in 15% normal goat/horse serum for 1 h at RT. Secondary labelling was achieved by using biotinylated anti-mouse horse or anti-rabbit goat antibody (Vector Laboratories, Burlingame, CA, USA; 30 min, RT). Horseradish peroxidase conjugated avidin (30 min, RT) and diaminobenzidine (6 min, RT) were used to visualise the labelling (Vector Laboratories). The enzymatic reaction was enhanced with nickel–cobalt to give a black precipitate, and the sections were counterstained with Nuclear Fast Red.
Bone marrow smears were fixed in methanol. After rehydration NT and PAR immunohistochemistry was performed as described above.
The degree of HNE and NT staining (scale of 1–10) was determined by an investigator blinded to the experimental groups. To count the percentage of NT-positive cells, at least 300 cells were counted on each smear. To measure the level of PAR accumulation, a semi-quantitative PAR score was established on a scale of 1–10 and the sections and smears were evaluated by a blinded experimenter. Score 1 was defined as no staining, 2 as light cytoplasmic staining, 3 as strong cytoplasmic staining, 4 as cytoplasmic staining with a few positive nuclei, 5 as approximately 50% positive nuclei, 6 as approximately 75% positive nuclei, 7 as general nuclear staining with a few negative cells, 8 as all the nuclei positive, 9 as a strong nuclear staining in all cells, 10 as a very strong general nuclear staining in all cells.
Results
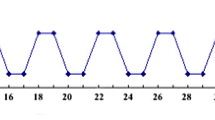
The blood glucose levels of the untreated control rats showed only a very slight circadian rhythm between 7.2 ± 0.8 mmol/l and 8.5 ± 0.3 mmol/l. The animals in the untreated DM group were markedly hyperglycaemic; their blood glucose levels fluctuated between 28.8 ± 5.6 mmol/l and 46.4 ± 4.2 mmol/l. DM-GGC animals, similarly to untreated control rats, showed only slight circadian changes between 5.6 ± 1.1 mmol/l and 11.5 ± 8.4 mmol/l. Although this fluctuation due to insulin treatment does not follow the circadian changes of healthy animals, the blood glucose levels of these animals never exceeded the normal levels. In the DM-PGC group, blood glucose levels changed between 11.3 ± 1.5 and 43.4 ± 3.1 mmol/l (Fig. 2). In the DM group, the glucose AUC was significantly higher than in the other three groups (1,856 ± 44 vs control: 382 ± 8, DM-GGC: 399 ± 62, DM-PGC: 1,323 ± 73, p < 0.001). In addition, glucose AUC was significantly higher in the DM-PGC group than in the control and DM-GGC group (p < 0.001; Fig. 2). Fructosamine levels in the DM group were significantly higher than in the control group (204 ± 63 μmol/l vs 709 ± 162 μmol/l, p < 0.05). Fructosamine levels of DM-GGC and DM-PGC groups were similar to the control group and were significantly lower than in the DM group (709 ± 162 μmol/l vs 95 ± 45 μmol/l, p < 0.01 and 166 ± 49 μmol/l, p < 0.01, respectively) (Fig. 2). The Pearson coefficient between AUC and fructosamine was 0.72, p < 0.001.

Blood glucose profiles of control rats and DM rats with PGC or GGC. a After 10 days of insulin treatment, the blood glucose levels of the animals were monitored for 48 h; the collection of samples started immediately before insulin dosage and was repeated every 6 h. Black diamonds, control (non-diabetic) rats; black squares, DM rats; white triangles, DM-GGC rats; white circles, DM-PGC rats. Values are means±SEM. b Total glucose AUC in the four animal groups. Values are means±SEM. ***p < 0.001 vs control; † p < 0.001 vs DM; ‡ p < 0.001 vs DM-GGC. c Fructosamine levels of the four experimental groups. Values are means±SEM. *p < 0.05 vs control; **p < 0.01 vs DM
Experiments conducted on vascular rings showed a marked impairment in the phenylephrine-induced contractions and in the acetylcholine-induced, endothelium-dependent relaxations in the DM-PGC group (Fig. 3). The latter effect is probably related to a reduced ability of the vascular endothelium to produce NO in response to acetylcholine, and not due to a reduced ability of the vascular smooth muscle to relax to NO, because the relaxant effect of the NO donor sodium nitroprusside was not attenuated (data not shown).

Effects of insulin treatment on contractile and endothelium-dependent relaxant function of the thoracic aorta. Phenylephrine-induced contractions (10 nmol/l–30 μmol/l) were obtained in resting vascular rings (a), whereas endothelium-dependent relaxations to acetylcholine (1 nmol/l–30 μmol/l) were obtained in rings pre-contracted with phenylephrine (1 µmol/l) (b). Black diamonds, control (non-diabetic) rats; black squares, DM rats; white triangles, DM-GGC rats; white circles, DM-PGC rats. Values are means±SEM. *p < 0.05 DM-PGC vs control
Immunohistochemical analysis showed that the most pronounced PARP activity was localised in the endothelium of the DM-PGC animals (4.8 ± 0.7 vs DM-GGC: 2.0 ± 0.3; Fig. 4). Similarly a tendency for a stronger HNE staining was seen in the DM-PGC group, although the differences did not reach the level of significance (control: 3.4 ± 0.3, DM: 5.1 ± 1.3, DM-GCC: 4.3 ± 1.2, DM-PGC: 5.5 ± 1.3). NT immunohistochemistry did not reveal any significant difference between the experimental groups. When western blots involving whole aortic homogenates were tested, the amount of poly(ADP-ribosyl)ated proteins was highest in the untreated diabetic group, and was lower in the diabetic animals treated with short- or long-lasting insulin. However, there was a 50 kDa poly(ADP-ribosyl)ated band that was more pronounced in the poorly insulin controlled diabetic animals than in the diabetic animals without insulin treatment (Fig. 4).

PARP activation in the aortic wall. Effect of DM with GGC or PGC on PARP activation in the different layers of the aortic wall. a PAR score of the aortic wall. The strongest PAR staining in the endothelial layer of the aorta was observable in DM-PGC rats. ‡ p < 0.01 for DM-GGC vs DM-PGC rats. b Representative immunohistochemical aorta sections stained with anti-PAR antibody. Positive staining is represented in black; red coloured Nuclear Fast Red was used as counterstain. Scale bar, 50 μm. Arrows show positive nuclei. c Densitometric analysis of the PAR western blots of aortic walls. ID, relative image density (% of untreated control, which is considered 100%). White columns, control rats; black columns, DM rats; hatched columns, DM-GGC rats, grey columns, DM-PGC rats. The highest amount of poly(ADP-ribosyl)-ated proteins can be seen in the diabetes group. PARP hyper-PARylation was similar in all experimental groups. However, the degree of PARylation of proteins about 50 kDa was the highest in the DM-PGC animals. Values are means±SEM. *p < 0.05 vs control, † p < 0.05 vs DM. d, e Representative PAR western blots of aortic walls
There was a marked increase in PARP activity in the circulating leucocytes in the DM rats, as evidenced by flow cytometry (Fig. 5). This effect was reversed with insulin treatment in the DM-GGC group. Interestingly, the severely fluctuating hyperglycaemia in DM-PGC animals did not attenuate PARP activity compared with DM-GGC animals or with the control rats (Fig. 5).

Flow cytometric analysis of circulating leucocytes. Effect of diabetes and insulin treatment with lente and ultralente insulin on PARP activation in circulating leucocytes of control rats and DM rats with GGC or PGC. a Mean fluorescence intensity of R1 cells (lymphocytes) stained with anti-PAR antibody. Diabetes caused a significant increase in the PAR content of these cells. Insulin treatment significantly reduced this effect. Values are means±SEM. *p < 0.05, **p < 0.01 between the appropriate experimental groups, as indicated. b Representative flow cytometric measurement of PAR-stained circulating lymphocytes. FL1-H shows the fluorescence intensity of cells. ‘Counts’ means the number of cells having certain fluorescence intensities. Black, control non-diabetic animals; red, DM animals without insulin treatment; blue, DM-GGC (achieved with lente insulin); green: DM-PGC (achieved with ultralente insulin)
The immunohistochemical analysis of bone marrow smears showed increased numbers of NT-positive cells in DM and DM-PGC groups compared with the control group (8.9 ± 0.6% and 8.4 ± 0.6% vs 3.7 ± 0.9%, respectively, p < 0.01). The strongest PAR staining was found in the DM group. Although in diabetic animals insulin treatment in DM-GGC decreased PAR positivity, in DM-PGC it did not exert a similar effect (Fig. 6).

a Per cent of NT-positive bone marrow cells. Increased numbers of NT-positive cells were observed in DM animals and in the DM-PGC animals (treated with ultralente insulin). Values are means±SEM. **p < 0.01 vs control. b PAR positivity scores of bone marrow cells. The strongest PAR staining was found in the DM group (without insulin treatment). GGC with lente insulin treatment reduced PAR positivity, while PGC with ultralente insulin treatment failed to have a similar effect. Values are means±SEM. **p < 0.01 vs control, † p < 0.01 vs DM. c Representative NT and PAR immunohistochemisty of bone marrow smears. Black represents positive labelling. Red coloured Nuclear Fast Red served as counterstain. Scale bar, 50 μm. Arrows show the NT-positive bone marrow cells
Discussion
Endothelial dysfunction plays an important role in the development of macro- and microvascular complications of diabetes. In various models of diabetes, increased blood glucose level is strongly linked to the pathophysiological changes leading to vascular dysfunction [12, 13]. In the case of human studies, determination of intima–media thickness of the common carotid artery is a generally accepted marker of early atherosclerosis. In addition to correlating with high fasting blood glucose levels and plasma HbA1c levels, this marker is also shown to be related to postprandial plasma glucose swings [8, 9]. Postprandial glucose swings are shown to be an independent factor of atherosclerosis not only in diabetic patients but also in individuals with impaired glucose tolerance and even in healthy individuals [1]. This observation suggests that even short hyperglycaemic episodes may induce the early steps of pathophysiological events in the vasculature [24]. In vitro studies suggest that glucose swings induce more severe renal fibrogenesis than stable high glucose [25]. In non-obese type 2 diabetic (Goto–Kakisaki) rats, repetitive fluctuations in blood glucose induced by fractionated feeding was shown to enhance monocyte adhesion to the endothelium of the thoracic aorta, even if these animals had lower HbA1c levels than their litter mates fed ad libitum. This increase is inhibitable by reducing postpandrial hyperglycaemia with phloridzin (sodium–glucose co-transporter inhibitor), nateglinide (insulin secretagogue) or insulin [26, 27]. Similar effects of glucose swings were observed in apolipoprotein E-deficient mice, which was inhibited by the α-glucosidase inhibitor miglitol [28]. In type 2 diabetic patients having similar HbA1c levels, the 24 h urinary excretions rates of unbound 8-iso-prostaglandin F2α correlates with the mean amplitude of glycaemic excursions but not with HbA1c or fasting glucose levels [29]. In healthy individuals and type 2 diabetic patients, oscillating glucose, over a period of 24 h, was found to be more damaging to endothelial function than stable, constant high glucose. At peak glucose values, this is true not only when an individual is exposed to the same total amount of glucose for 24 h, but also even when the total amount is higher. Oxidative stress was shown to play a key role in this phenomenon [30]. Although significant work has been conducted to address the questions, whether the short hyperglycaemia itself or the exaggerated changes (‘swings’) in blood glucose level are more important as risk factors for endothelial dysfunction and how oxidative stress is involved, remained unanswered and were, therefore, investigated in the present study.
In our experiments endothelium-dependent relaxation was measured at about average blood glucose levels of each experimental group. The results demonstrated that diabetic rats that received insulin every 2 days (resulting in large fluctuations in blood glucose levels, to mimic a ‘poor glycaemic control’ type situation), exhibited the most impairment in their acetylcholine-induced endothelium-dependent vascular relaxation of the thoracic aorta. This endothelial dysfunction developed, even though, on average, these animals had significantly lower mean blood glucose level than the diabetic rodents without any insulin treatment (rings from animals that belonged to this latter group exhibited a relaxant capability similar to those of the non-diabetic control rats). These results suggest that the oscillation of blood glucose level itself is a more important contributor to the loss of endothelial function in diabetes than the average level of mean blood glucose level per se.
Aggressive glycaemic control of diabetic patients is known to reduce the risk of the development of late complications [31]. HbA1c, one of the most frequently used clinical markers of glucose homeostasis, correlates with the average of blood glucose levels of 6–8 weeks prior testing (i.e. it correlates with the ‘area under the curve’, and is not sensitive to the spikes and swings that occur in these patients). Based on data in the literature, as well as from the results of the current study, it appears that fructosamine behaves in a similar fashion. It is interesting to note in this context that recent studies showed that pre-breakfast blood glucose level has the closest correlation to HbA1c, and the relative contribution of postprandial blood glucose concentrations to HbA1c decreases in patients with PGC [32]. Boland et al., using a continuous glucose monitoring system, revealed profound postpandrial hyperglycaemia in paediatric patients with type 1 diabetes despite excellent HbA1c levels [33]. With frequent, or even continuous monitoring of blood glucose levels and frequent administration of insulin (or by ‘insulin clamping’ using insulin pumps), postprandial glucose spikes can be prevented. Based on the current results, we speculate that a potentially more effective way of preventing diabetic complications would be by the use of a continuous glucose-monitoring/insulin-supply system.
In various models of diabetes, oxidative, nitrosative stress and PARP activation have been shown to play important roles in the pathogenesis of diabetic complications [10–17, 21, 34]. In diabetic rats, pharmacological inhibition of PARP not only prevents, but also reverses endothelial dysfunction [12]. There are in vitro findings showing that oscillations in blood glucose concentration, themselves, can provoke increased free radical formation and consequent PARP activation, culminating in pathological changes in the vascular endothelium, leading to endothelial dysfunction [19, 35, 36]. Our in vivo findings are consistent with in vitro studies in cultured human umbilical vein endothelial cells, in demonstrating that rapid glycaemic swings result in the most substantial increase in vascular PARP activation. In the in vitro studies, the endothelial PARP activation was generally attributed to increased formation of reactive oxygen and nitrogen species. However, in the current study, the extent of vascular PARP activation did not show any correlation with vascular NT staining (a marker of peroxynitrite formation), and only a slight and non-significant correlation with changes of vascular HNE (an index of reactive oxidant formation). It is possible that the reactive species responsible for vascular PARP activation are not generated in the vascular wall itself, but may be derived from other sources, for instance circulating cells (see below). It is also possible that PARP activation in the vasculature of the DM-PGC group is not driven by reactive species formation, but by other mechanisms. In this context it is relevant to note that there are many endogenous factors (from kinases to intracellular calcium to various hormones) that can modulate PARP activity independently of DNA breakage and reactive oxygen and nitrogen species [37, 38].
Interestingly, when western blots involving whole aortic homogenates were tested, the overall amount of poly(ADP-ribosyl)ated proteins was lower in the diabetic animals treated with either short- or long-lasting insulin. These assays involve homogenates that include a limited amount of endothelial cells, together with significant amounts of vascular smooth muscle cells. Therefore, this assay is unable to detect endothelial-specific PARylation. Nevertheless, it was interesting to note that there was an 50 kDa poly(ADP-ribosyl)ated band that was more pronounced in DM-PGC animals than in the DM animals without insulin treatment (Fig. 4). The identity of this particular protein would be of significant interest, and is the subject of current investigations.
In diabetic patients, oxidative and nitrosative stress is not restricted to various regions or organs: it is a systemic phenomenon. Elevated levels of NT can be observed in the plasma of diabetic patients [39, 40]. Thus, not only endothelial cells, but also circulating leucocytes can be sources and targets of reactive species. Glucose-induced free radical formation in circulating leucocytes has been proposed to contribute to the development of atherosclerosis [41]. Adaikalakoteswari et al. showed that PARP activity in peripheral blood lymphocytes is elevated in patients with type 2 diabetes compared with healthy controls [42]. On the contrary, Tempera et al. reported the opposite [43]. Although they observed increased PARP-1 mRNA content in circulating mononuclear cells of type 2 diabetic patients, they measured decreased PARP-1 activity in these cells [42]. In our experimental conditions we found an increase in PARP activation of circulating leucocytes in a rat model of type 1 diabetes. The highest PAR content of isolated lymphocytes was found in the untreated diabetic group. In contrast to the endothelial PARP activation, which was only normalised in the diabetic rats with GGC, PARP activation in circulating leucocytes was normalised by insulin treatment, in both the GGC and PGC rats. On the other hand, in the case of bone marrow cells, similarly to the endothelial cells, the degree of nitrosative stress and PARP activation was only reduced in the rats with GGC, but not in the rats with PGC. One possibility to explain these findings is that leucocytes with the highest degree of PARP activation die and are eliminated from the circulation, and hence are absent from our analysis.
A recent study by our group investigating the effect of insulin in the context of stress-induced hyperglycaemia in a rat model [44] may be relevant in the context of the current study. In that study, systemic lipopolysaccharide treatment caused hyperglycaemia and PARP activation in circulating leucocytes. Insulin administration prevented the elevation of blood glucose level and also PARP activation [44]. We also confirmed in vitro that insulin does not have any major direct effects on PARP activity in cultured cells in vitro [42], suggesting that the effects of insulin on PARP activation in the current study are indirect, most likely the consequences of the modulation of reactive oxygen and nitrogen species production in the vasculature.
As HbA1c and fructosamine measurements do not reflect the frequency and severity of glycaemic swings (see above), the clinical introduction of a plasma or blood marker for such swings may be of potential diagnostic and predictive value. Currently, no such marker is available. As shown in the current study, circulating leucocyte PARP activation may not be suitable for such purpose. In fact, we have previously conducted PAR staining in skin biopsies in humans, and they, indeed, correlate with the degree of endothelial dysfunction in the patients [45]. However, skin biopsies are unlikely to be useful for routine diagnosis in patients with diabetes. Additional studies are needed to identify markers suitable to detect glycaemic swings, preferably ones that are simple and can be conducted through blood-sample analysis.
Our findings indicate that exaggeratedly changing blood glucose levels, regardless of their effect on average blood glucose levels, cause a significant impairment of vascular function. Such changes may contribute to the development of diabetic macrovascular complications. Based on the current findings, we propose that systemic increases in free radical formation and PARP activation induced by oscillating blood glucose level may be involved in this phenomenon.
Abbreviations
- DM:
-
Diabetes mellitus
- GGC:
-
Good glycaemic control
- HNE:
-
4-Hydroxy-2-noneal
- NO:
-
Nitric oxide
- NT:
-
Nitrotyrosine
- PAR:
-
Poly(ADP-ribose)
- PARP:
-
Poly(ADP-ribose) polymerase
- PGC:
-
Poor glycaemic control
- R1:
-
Region 1 on flow cytometry
- RT:
-
Room temperature
- STZ:
-
Streptozotocin
References
Hanefeld M, Koehler C, Schaper F, Fuecker K, Henkel E, Temelkova-Kurktschiev T (1999) Postprandial plasma glucose is an independent risk factor for increased carotid intima-media thickness in non-diabetic individuals. Atherosclerosis 144:229–235
Hanefeld M, Koehler C, Fuecker K et al (2003) Insulin secretion and insulin sensitivity pattern is different in isolated impaired glucose tolerance and impaired fasting glucose: the Risk Factor in Impaired Glucose Tolerance for Atherosclerosis and Diabetes study. Diabetes Care 26:868–874
Balkau B, Shipley M, Jarrett RJ et al (1998) High blood glucose concentration is a risk factor for mortality in middle-aged nondiabetic men. 20-year follow-up in the Whitehall Study, the Paris Prospective Study, and the Helsinki Policemen Study. Diabetes Care 21:360–367
Ceriello A, Davidson J, Hanefeld M et al (2006) Postprandial hyperglycaemia and cardiovascular complications of diabetes: An update. Nutr Metab Cardiovasc Dis 16:453–456
Ceriello A (2003) The possible role of postprandial hyperglycaemia in the pathogenesis of diabetic complications. Diabetologia 46(Suppl 1):M9–M16
Temelkova-Kurktschiev TS, Koehler C, Henkel E, Leonhardt W, Fuecker K, Hanefeld M (2000) Postchallenge plasma glucose and glycemic spikes are more strongly associated with atherosclerosis than fasting glucose or HbA1c level. Diabetes Care 23:1830–1834
Hanefeld M, Schmechel H, Schwanebeck U, Lindner J (1997) Predictors of coronary heart disease and death in NIDDM: the Diabetes Intervention Study experience. Diabetologia 40(Suppl 2):S123–S124
Hanefeld M, Fischer S, Julius U et al (1996) Risk factors for myocardial infarction and death in newly detected NIDDM: the Diabetes Intervention Study, 11-year follow-up. Diabetologia 39:1577–1583
Hanefeld M, Temelkova-Kurktschiev T (1997) The postprandial state and the risk of atherosclerosis. Diabet Med 14(Suppl 3):S6–S11
Obrosova IG, Mabley JG, Zsengeller Z et al (2005) Role for nitrosative stress in diabetic neuropathy: evidence from studies with a peroxynitrite decomposition catalyst. FASEB J 19:401–403
Pacher P, Liaudet L, Soriano FG, Mabley JG, Szabo E, Szabo C (2002) The role of poly(ADP-ribose) polymerase activation in the development of myocardial and endothelial dysfunction in diabetes. Diabetes 51:514–521
Soriano FG, Pacher P, Mabley J, Liaudet L, Szabo C (2001) Rapid reversal of the diabetic endothelial dysfunction by pharmacological inhibition of poly(ADP-ribose) polymerase. Circ Res 89:684–691
Soriano FG, Virag L, Szabo C (2001) Diabetic endothelial dysfunction: role of reactive oxygen and nitrogen species production and poly(ADP-ribose) polymerase activation. J Mol Med 79:437–448
Susztak K, Bottinger EP (2006) Diabetic nephropathy: a frontier for personalized medicine. J Am Soc Nephrol 17:361–367
Susztak K, Raff AC, Schiffer M, Bottinger EP (2006) Glucose-induced reactive oxygen species cause apoptosis of podocytes and podocyte depletion at the onset of diabetic nephropathy. Diabetes 55:225–233
Zheng L, Szabo C, Kern TS (2004) Poly(ADP-ribose) polymerase is involved in the development of diabetic retinopathy via regulation of nuclear factor-kappaB. Diabetes 53:2960–2967
Brownlee M (2001) Biochemistry and molecular cell biology of diabetic complications. Nature 414:813–820
Masson M, Niedergang C, Schreiber V, Muller S, Menissier-de Murcia J, de Murcia G (1998) XRCC1 is specifically associated with poly(ADP-ribose) polymerase and negatively regulates its activity following DNA damage. Mol Cell Biol 18:3563–3571
Buki KG, Bauer PI, Hakam A, Kun E (1995) Identification of domains of poly(ADP-ribose) polymerase for protein binding and self-association. J Biol Chem 270:3370–3377
Virag L, Szabo C (2002) The therapeutic potential of poly(ADP-ribose) polymerase inhibitors. Pharmacol Rev 54:375–429
Szabo C (2009) Role of nitrosative stress in the pathogenesis of diabetic vascular dysfunction. Br J Pharmacol doi:10.1111/j.1476-5381.2008.00086.x
Piconi L, Quagliaro L, Da Ros R et al (2004) Intermittent high glucose enhances ICAM-1, VCAM-1, E-selectin and interleukin-6 expression in human umbilical endothelial cells in culture: the role of poly(ADP-ribose) polymerase. J Thromb Haemost 2:1453–1459
Mabley JG, Horvath EM, Murthy KG et al (2005) Gender differences in the endotoxin-induced inflammatory and vascular responses: potential role of poly(ADP-ribose) polymerase activation. J Pharmacol Exp Ther 315:812–820
Ceriello A (1997) Acute hyperglycaemia and oxidative stress generation. Diabet Med 14(Suppl 3):S45–S49
Polhill TS, Saad S, Pronnik P et al (2004) Short-term peaks in glucose promote renal fibrogenesis independently of total glucose exposure. Am J Physiol Renal Physiol 287:F268–F273
Azuma K, Kavamori R, Toyokufu Y et al (2006) Repetitive fluctuations in blood glucose enhance monocyte adhesion to the endothelium of rat thoracic aorta. Arterioscler Thromb Vasc Biol 26:2275–2280
Tanaka A, Azuma K, Toyofuku Y et al (2006) Insulin and nateglidine reduce monocyte adhesion to endothelial cells in Goto-Kakizaki rats exhibiting repetitive blood glucose fluctuation. Biochem Biophys Res Commun 350:195–201
Mita T, Otsuka A, Azumura K et al (2007) Swings in blood glucose levels accelerate atherogenesis in apolipoprotein E-deficient mice. Biochem Biophys Res Commun 358:679–685
Monnier L, Mas E, Ginet C et al (2006) Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 295:1681–1687
Ceriello A, Esposito K, Piconi L et al (2008) Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes 57:1349–1354
Robertson C (2006) Physiologic insulin replacement in type 2 diabetes: optimizing postprandial glucose control. Diabetes Educ 32:423–432
Pistrosch F, Koehler C, Wildbrett J, Hanefeld M (2006) Relationship between diurnal glucose levels and HbA1c in type 2 diabetes. Horm Metab Res 38:455–459
Boland E, Monsod T, Delucia M, Brandt CA, Fernando S, Tamborlane WV (2001) Limitations of conventional methods of self-monitoring of blood glucose: lessons learned from 3 days of continuous glucose sensing in pediatric patients with type 1 diabetes. Diabetes Care 24:1858–1862
Du X, Matsumura T, Edelstein D et al (2003) Inhibition of GAPDH activity by poly(ADP-ribose) polymerase activates three major pathways of hyperglycemic damage in endothelial cells. J Clin Invest 112:1049–1057
Piconi L, Quagliaro L, Assaloni R et al (2006) Constant and intermittent high glucose enhances endothelial cell apoptosis through mitochondrial superoxide overproduction. Diabetes Metab Res Rev 22:198–203
Risso A, Mercuri F, Quagliaro L, Damante G, Ceriello A (2001) Intermittent high glucose enhances apoptosis in human umbilical vein endothelial cells in culture. Am J Physiol Endocrinol Metab 281:E924–E930
Szabo C, Pacher P, Swanson RA (2006) Novel modulators of poly(ADP-ribose) polymerase. Trends Pharmacol Sci 27:626–630
Hegedus C, Lakatos P, Olah G, Toth et al (2008) Protein kinase C protects from DNA damage-induced necrotic cell death by inhibiting poly(ADP-ribose) polymerase-1. FEBS Lett 582:1672–1678
Ceriello A, Mercuri F, Quagliaro L et al (2001) Detection of nitrotyrosine in the diabetic plasma: evidence of oxidative stress. Diabetologia 44:834–838
Ceriello A (2003) New insights on oxidative stress and diabetic complications may lead to a ‘causal’ antioxidant therapy. Diabetes Care 26:1589–1596
Goldin A, Beckman JA, Schmidt AM, Creager MA (2006) Advanced glycation end products: sparking the development of diabetic vascular injury. Circulation 114:597–605
Adaikalakoteswari A, Rema M, Mohan V, Balasubramanyam M (2007) Oxidative DNA damage and augmentation of poly(ADP-ribose) polymerase/nuclear factor-kappa B signaling in patients with type 2 diabetes and microangiopathy. Int J Biochem Cell Biol 39:1673–1684
Tempera I, Cipriani R, Campagna G et al (2005) Poly(ADP-ribose)polymerase activity is reduced in circulating mononuclear cells from type 2 diabetic patients. J Cell Physiol 205:387–392
Horváth EM, Benkő R, Gerő D, Kiss L, Szabó C (2008) Treatment with insulin inhibits poly(ADP-ribose)polymerase activation in a rat model of endotoxemia. Life Sci 82:205–209
Szabó C, Zanchi A, Komjáti K et al (2002) Poly(ADP-ribose) polymerase is activated in subjects at risk of developing type 2 diabetes and is associated with impaired vascular reactivity. Circulation 106:2680–2686
Acknowledgements
This work was supported by the National Institutes of Health (NIH R01 GM060915), the OTKA (Hungarian Scientific Research Fund, Budapest, Hungary) and the Zsigmond Diabetes Foundation (Budapest, Hungary).
Duality of interest
C. Szabo is a founder and stockholder of Inotek Pharmaceuticals Corporation, a pharmaceutical organisation involved in the development of PARP inhibitors and catalytic antioxidants. All other authors declare that there is no duality of interest associated with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Horváth, E.M., Benkő, R., Kiss, L. et al. Rapid ‘glycaemic swings’ induce nitrosative stress, activate poly(ADP-ribose) polymerase and impair endothelial function in a rat model of diabetes mellitus. Diabetologia 52, 952–961 (2009). https://doi.org/10.1007/s00125-009-1304-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-009-1304-0