
Abstract
Aim
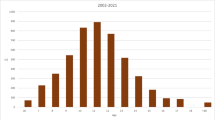
The aim of the present study was to analyze whether there were changes in the severity of malocclusions of patients treated at the Department of Orthodontics, University of Giessen, Germany over a period of 20 years (1992–2012) and if the implementation of the KIG system (German index of treatment need) in 2001 had any effect on the patient cohort. Furthermore, the study aimed to analyze the influence of the severity of malocclusion on treatment quality and economic efficiency (relation payment per case/treatment effort).
Materials and methods
The files of all 5385 patients admitted to the orthodontic department between 1992 and 2012 were screened and the following information was recorded: patient characteristics, treatment duration, KIG, treatment outcome, and costs.
Results
In the KIG period, patients were older, pretreatment malocclusions were more severe, treatment took longer, required more appointments, and did not achieve the same degree of perfection as in the pre-KIG period. Patients with a higher pretreatment KIG category had longer treatments and did not achieve the same degree of perfection as patients with lower KIG categories. Although total payment was slightly higher for the more severe cases, their cost-per-appointment ratio was significantly lower.
Conclusion
In the present university department, a shift of the orthodontic care task towards more complex cases has occurred over the last 20 years. Generally the quality of orthodontic treatment was good, but it has been demonstrated that the higher KIG cases did not end up at the same level of excellence as the lower KIG cases. Furthermore, KIG 5 patients had a longer treatment duration, and required more appointments than lower KIG cases.
Zusammenfassung
Ziel
Ziel der vorliegenden Arbeit war es zu untersuchen, ob sich der Schweregrad der Malokklusionen von Patienten der Poliklinik für Kieferorthopädie der Justus-Liebig-Universität Gießen über einen Zeitraum von 20 Jahren (1992–2012) verändert hat und ob die Einführung des KIG(Kieferorthopädische Indikationsgruppen)-Systems Einfluss auf die Patientenkohorte der Abteilung hatte. Des Weiteren wurde der Einfluss des Schweregrads der Malokklusion auf das Behandlungsergebnis und auf die Wirtschaftlichkeit der Abteilung (Verhältnis Einnahmen/Behandlungsaufwand) analysiert.
Material und Methoden
Die Akten von allen 5385 zwischen 1992 und 2012 aufgenommenen gesetzlich versicherten Patienten wurden untersucht. Analysiert wurden die Parameter Patientencharakteristika, Behandlungsdauer, KIG, Behandlungsergebnis und Kosten.
Ergebnisse
Nach Einführung des KIG-Systems waren die Patienten im Durchschnitt ein Jahr älter, hatten ausgeprägtere Malokklusionen und erreichten nicht die gleiche Perfektion im Behandlungsergebnis wie vor Einführung des KIG-Systems. Ferner fiel auf, dass Patienten mit hohem KIG (5) durchschnittlich eine 7 Monate längere Behandlungsdauer und 6 Kontrolltermine mehr hatten als KIG-3-Patienten. Generell waren die Behandlungsergebnisse gut, jedoch zeigte sich ein Zusammenhang zwischen dem Schweregrad der Malokklusion und der Ergebnisqualität. So erreichten beispielweise nur 51,4% der KIG-5-Fälle ein ausgezeichnetes oder gutes Ergebnis, während dies bei 65,6% der KIG-3-Patienten der Fall war. Zwar wurde die Behandlung von ausgeprägten Malokklusionen (KIG 5) durchschnittlich etwas höher vergütet, jedoch waren auch mehr Kontrolltermine nötig, sodass die Einnahmen-pro-Termin-Bilanz bei KIG-5-Fällen ungünstiger war als bei KIG-3-Patienten (74,92 vs. 82,21€/Termin).
Schlussfolgerung
In den vergangenen 20 Jahren hat eine Verschiebung des Patientengutes hin zu komplexeren Fällen stattgefunden. Patienten mit hohem Ausgangs-KIG-Wert erreichten nicht den gleichen Grad an Perfektion wie weniger komplexe Fälle, und ihre Therapie wurde in Relation zum Behandlungsaufwand geringer vergütet. Nach Einführung des KIG-Systems sind somit am untersuchten Standort negative Auswirkungen auf die Wirtschaftlichkeit der Abteilung entstanden.





Similar content being viewed by others


References
Ahlgren J (1988) Tiorårig utvärderin av ortodontiska behandlingsresultat. Tandlakartidningen 80:208–216
Allareddy V, Rampa S, Anamali S et al (2015) Obesity and its association with comorbidities and hospital charges among patients hospitalized for dental conditions. J Investig Clin Dent 9:1–8
Assimakopolou T (2004) Evaluierung der Prävalenzrate bei 9 bis 10-jährigen Probanden nach den Kieferorthopädischen Indikationsgruppen (KIG). Zahnmed Dissertation. Medizinische Fakultät der Westfälischen Wilhelms-Universität Münster
Baumgart DC, le Claire M (2016) The expenditures for academic inpatient care of inflammatory bowel disease patients are almost double compared with average academic gastroenterology and hepatology cases and not fully recovered by Diagnosis-Related Group (DRG) Proceeds. PLoS ONE 11(1):e0147364. doi:10.1371/journal.pone.0147364
Beckwith FR, Ackerman RJ Jr, Cobb CM et al (1999) An evaluation of factors affecting duration of orthodontic treatment. Am J Orthod Dentofacial Orthop 115:439–447
Bock JJ, Czarnota J, Hirsch C et al (2011) Orthodontic treatment need in a representative adult cohort. J Orofac Orthop 72:421–433
Bock NC, von Bremen J, Ruf S (2016) Stability of Class II fixed functional appliance therapy-a systematic review and meta-analysis. Eur J Orthod 38:129–139
Björk A, Krebs A, Solow B (1964) Method for epidemiological registration of malocclusion. Acta Odont Scand 22:27–41
Brook PH, Shaw WC (1989) The development of an index of orthodontic treatment priority. Eur J Orthod 11:309–320
Busse R, Geissler A, Aaviksoo A et al (2013) Diagnosis related groups in Europe: moving towards transparency, efficiency, and quality in hospitals? BMJ 7(346):f3197
BZÄK/KZBV (2011) Daten & Fakten 2011
Campbell CL, Roberts WE, Hartsfield JK Jr et al (2007) Treatment outcomes in a graduate orthodontic clinic for cases defined by the American Board of Orthodontics malocclusion categories. Am J Orthod Dentofacial Orthop 132:822–829
Cansunar HA, Uysal T (2014) Relationship between pretreatment case complexity and orthodontic clinical outcomes determined by the American Board of Orthodontics criteria. Angle Orthod 84:974–979
Deguchi T, Honjo T, Fukunaga T et al (2005) Clinical assessment of orthodontic outcomes with the peer assessment rating, discrepancy index, objective grading system, and comprehensive clinical assessment. Am J Orthod Dentofac Orthop 127:434–443
Fisher MA, Wenger RM, Hans MG (2010) Pretreatment characteristics associated with orthodontic treatment duration. Am J Orthod Dentofac Orthop 137:178–186
Genzel H (2003) Richtlinien des Bundesausschusses der Zahnärzte und Krankenkassen für die kieferorthopädische Behandlung. Bundesanzeiger 226:24966
Glasl B, Ludwig B, Schopf P (2006) Prevalence and development of KIG-relevant symptoms in primary school students in Frankfurt am Main. J Orofac Orthop 67:414–423
Gottstein I, Borutta A (2007) Die Eignung der „Kieferorthopädischen Indikationsgruppen” (KIG) für die zahnärztliche Vorsorgeuntersuchung des Öffentlichen Gesundheitsdienstes (ÖGD). Gesundheitswesen 69:577–581
Holmes JH 4th (2008) Critical issues in burn care. J Burn Care Res 29(6 Suppl 2):180–187
Hsu BS, Brazelton TB 3rd (2015) A Comparison of Costs Between Medical and Surgical Patients in an Academic Pediatric Intensive Care Unit. WMJ 114(6):236–239
Izadi M, Gill DS, Naini FB (2010) Retrospective study to determine the change in referral pattern to St George’s Hospital Orthodontic Department before and after the 2006 NHS Dental Contract changes. Prim Dent Care 17:111–114
Kagan RJ, Edelman L, Solem L et al (2007) DRG 272: does it provide adequate burn center reimbursement for the care of patients with Stevens-Johnson syndrome and toxic epidermal necrolysis? J Burn Care Res 28:669–674
Kagan RJ, Gamelli R, Saffle JR (2007) DRG 504: the effect of 96 hours of mechanical ventilation on resource utilization. J Burn Care Res 28:664–668
KZBV (2001) Änderung der Kieferorthopädie-Richtlinien des Bundesausschusses der Zahnärzte und Krankenkassen—Einführung des neuen Systems kieferorthopädischer Indikationsgruppen (KIG)
KZBV (2015) Jahrbuch. Statistische Basisdaten zur vertragszahnärztlichen Versorgung 85:162–166
Lisson J, Rijpstra C (2016) Die kieferorthopädischen Indikationsgruppen (KIG) und ihre Grenzen. Dtsch Zahnarztl Z 1:25–37
Lotter O, Jaminet P, Amr A et al (2011) Reimbursement of burns by DRG in four European countries: an analysis. Burns 37:1109–1116
Mavreas D, Athanasiou AE (2008) Factors affecting the duration of orthodontic treatment: a systematic review. Eur J Orthod 30:386–395
Mehra T, Koljonen V, Seifert B et al (2015) Total inpatient treatment costs in patients with severe burns: towards a more accurate reimbursement model. Swiss Med Wkly 24(145):w14217. doi:10.4414/smw.2015.14217
Mesti T, Boshkoska BM, Kos M et al (2015) The cost of systemic therapy for metastatic colorectal carcinoma in Slovenia: discrepancy analysis between cost and reimbursement. Radiol Oncol 49(2):200–208
Tang EL, Wei SH (1990) Assessing treatment effectiveness of removable and fixed orthodontic appliances with the occlusal index. Am J Orthod Dentofac Orthop 98:550–556
von Bremen J, Pancherz H (2002) Efficiency of early and late Class II Division 1 treatment. Am J Orthod Dentofac Orthop 121(1):31–37
Wehrbein H, Wriedt S, Jung BA (2011) Change and innovation in orthodontics. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 54:1110–1115
Wiedel AP, Bondemark L (2015) Fixed versus removable orthodontic appliances to correct anterior crossbite in the mixed dentition—a randomized controlled trial. Eur J Orthod 37:123–127
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. von Bremen, E. M. Streckbein, and S. Ruf declare that they have no conflict of interest and did not receive financial support for this study.
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Dr. Julia von Bremen.
Rights and permissions
About this article

Cite this article
von Bremen, J., Streckbein, E.M. & Ruf, S. Changes in university orthodontic care over a period of 20 years. J Orofac Orthop 78, 321–329 (2017). https://doi.org/10.1007/s00056-017-0088-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-017-0088-y