
Abstract
Introduction
Osteonecrosis of the femoral head (ONFH) is a devastating disease with complete collapse of the femoral head often reported in greater than 70% of patients within 3 to 4 years of diagnosis. Early intervention prior to collapse may improve the chance of success of joint preserving procedures.
Questions/Purposes
The purpose of this study was to evaluate whether core decompression with mesenchymal stem cells combined with bisphosphonate therapy can improve the clinical outcomes and reduce the risk of hip replacement when compared to treatment with bisphosphonate therapy alone.
Methods
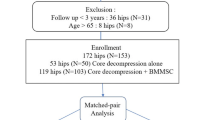
Between 2006 and 2014, 84 consecutive patients who were diagnosed with ONFH were identified from our institution’s registry. Of these 84 patients, 49 patients (62 hips), fit inclusion/exclusion criteria. Twenty-nine patients (40 hips) were treated with bisphosphonate therapy only. Twenty patients (20 hips) were treated with bisphosphonates, core decompression, and mesenchymal stem cells. Functional outcomes were assessed using the Modified Harris Hip Score (MHHS), the visual analog score (VAS), and evaluation of support system. Clinical failure was defined as deterioration of the MHHS/VAS scores and support system used severe enough to require THR. Radiologic outcome measures included the XR and MR imaging staging of the hip. Survival analysis was performed with total hip replacement as the end point failure. Collapse was defined as progression from Ficat stage I or II to stage III and from Steinberg I, II, III to IV, V, VI.
Results
Failure requiring THR occurred in 21/40 (52.5%) of bisphosphonates (BP)-treated hips at a mean follow-up of 25.3 ± 11.5 months and 5/22 (22.73%) of BP + CD + MSC-treated hips at a mean follow-up of 22.7 ± 19.5 months. The median (Q1, Q3) time to collapse was 24.9 (7.4, 33.0) months in BP-treated hips and 27.3 (27.3) months in BP + CD + MSC-treated hips. There was no evidence of a difference in functional outcomes between the two treatment groups. After adjusting for baseline Ficat stage, age, and sex, an unreplaced hip treated with BP + CD + MSC had 0.42 (95% CI 0.11, 1.57) times the risk of being replaced in the next moment compared to an unreplaced hip treated with bisphosphonates only (P = 0.196).
Conclusion
Our results demonstrate that treatment with BP alone or BP + CD + MSC can postpone the need for total hip arthroplasty (THA) in the first 24 months in patients with ONFH compared to previously reported data, but there is no statistically significant difference between the two treatment groups. Combination therapy of BP + CD + MSC may be more effective in delaying the progression of collapse in early stage ONFH. Future prospective studies are warranted to determine the efficacy of these treatment strategies in the long term.

Similar content being viewed by others


References
Agarwala S, Jain D, Joshi VR, Sule A. Efficacy of alendronate, a bisphosphonate, in the treatment of AVN of the hip. A prospective open-label study. Rheumatology (Oxford). 2005; 44(3): 352-359.
Agarwala S, Shah S, Joshi VR. The use of alendronate in the treatment of avascular necrosis of the femoral head: follow-up to 8 years. J Bone Joint Surg (Br). 2009; 91(8): 1013-1018.
Aigner N, Schneider W, Eberl V, Knahr K. Core decompression in early stages of femoral head avascular necrosis—an MRI-controlled study. Int Orthop. 2002; 26: 31.
Belmar CJ, Steinberg ME, Hartman-Sloan KM. Does pain predict outcome in hips with osteonecrosis? Clin Orthop Relat Res. 2004; 425: 158-162.
Bozic KJ, Zurakowski D, Thornhill TS. Survivorship analysis of hips treated with core decompression for nontraumatic osteonecrosis of the femoral head. J Bone Joint Surg Am. 1999; 81(2): 200-209.
Chen C, Chang J, Lai K, Hou S, Chang C, Wang G. Alendronate in the prevention of collapse of the femoral head in nontraumatic osteonecrosis: a two-year multicenter, prospective, randomized, double-blind, placebo-controlled study. Arthritis Rheumatol. 2012; 64(5): 1572-1578.
Colwell CW Jr, Robinson CA, Stevenson DD, Vint VC, Morris BA. Osteonecrosis of the femoral head in patients with inflammatory arthritis or asthma receiving corticosteroid therapy. Orthopedics. 1996; 19(11): 941-946.
Ficat R, Arlet J. Necrosis of the femoral head. In: Ischemia and necrosis of bone. Baltimore: Williams & Wilkins; 1980: 171-182.
Gangji V, De Maertelaer V, Hauzeur J. Autologous bone marrow cell implantation in the treatment of non-traumatic osteonecrosis of the femoral head: five year follow-up of a prospective controlled study. Bone. 2011; 49(5): 1005-1009.
Hashimoto M. The distribution of active marrow in the bones of normal adult. Kyushu J Med Sci. 1960; 11(3): 103-105.
Hernigou P, Beaujean F. Treatment of osteonecrosis with autologous bone marrow grafting. Clin Orthop Relat Res. 2002; 405: 14-23.
Hernigou P, Beaujean F, Lambotte JC. Decrease in the mesenchymal stem-cell pool in the proximal femur in corticosteroid-induced osteonecrosis. J Bone Joint Surg (Br). 1999; 81(2): 349-355.
Hernigou P, Poignard A, Zilber S, Rouard H. Cell therapy of hip osteonecrosis with autologous bone marrow grafting. Indian J Orthop. 2009; 43(1): 40-45.
Johannson HR, Zywiel MG, Marker DR, Jones LC, McGrath MS, Mont MA. Osteonecrosis is not a predictor of poor outcomes in primary total hip arthroplasty: a systematic literature review. Int Orthop. 2011; 35(4): 465-473.
Kang P, Pei F, Shen B, Zhou Z, Yang J. Are the results of multiple drilling and alendronate for osteonecrosis of the femoral head better than those of multiple drilling? A pilot study. Joint Bone Spine. 2012; 79(1): 67-72.
Koo KH, Kim R, Ko GH, Song HR, Jeong ST, Cho SH. Preventing collapse in early osteonecrosis of the femoral head. A randomised clinical trial of core decompression. J Bone Joint Surg (Br). 1995; 77(6): 870-874.
Lai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, Lin RM. The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. J Bone Joint Surg Am. 2005; 87(10): 2155-2159.
Mont MA, Carbone JJ, Fairbank AC. Core decompression versus nonoperative management for osteonecrosis of the hip. Clin Orthop Relat Res. 1996; 324(324): 169-178.
Neumayr LD, Aguilar C, Earles AN, et al. Physical therapy alone compared with core decompression and physical therapy for femoral head osteonecrosis in sickle cell disease. J Bone Joint Surg Am. 2006; 88(12): 2573-2582.
Sen RK. Management of avascular necrosis of femoral head at pre-collapse stage. Indian J Orthop. 2009; 43(1): 6-16.
Sen RK, Tripathy SK, Aggarwal S, Marwaha N, Sharma RR, Khandelwal N. Early results of core decompression and autologous bone marrow mononuclear cells instillation in femoral head osteonecrosis: a randomized control study. J Arthroplasty. 2012; 27(5): 679-686.
Steinberg ME, Bands RE, Parry S, Hoffman E, Chan T, Hartman K. Does lesion size affect the outcome in avascular necrosis? Clin Orthop Relat Res. 1999; 367: 262-271.
Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis. J Bone Joint Surg (Br). 1995; 77(1): 34-41.
Stulberg BN, Davis AW, Bauer TW, Levine M, Easley K. Osteonecrosis of the femoral head: a prospective randomized treatment protocol. Clin Orthop Relat Res. 1991; 268: 140-151.
Wang GJ, Cui Q, Balian G. The Nicolas andry award. The pathogenesis and prevention of steroid-induced osteonecrosis. Clin Orthop Relat Res. 2000; 370(370): 295-310.
Wang C, Peng J, Lu S. Summary of the various treatments for osteonecrosis of the femoral head by mechanism: a review. Exp Ther Med. 2014; 8(3): 700-706.
Yang S, Halim AY, Werner BC, Gwathmey FW, Cui Q. Does osteonecrosis of the femoral head increase surgical andmedical complication rates after total hip arthroplasty? A comprehensive analysis in the United States. Hip Int. 2015; 25(3): 237-244.
Zalavras CG, Lieberman JR. Osteonecrosis of the femoral head: evaluation and treatment. J Am Acad Orthop Surg. 2014; 22(7): 455-464.
Zhao D, Cui D, Wang B, et al. Treatment of early stage osteoecrosis of the femoral head with autologous implantation of bone marrow-derived and cultured mesenchymal stem cells. Bone. 2012; 50(1): 325-330.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Arianna L Gianakos, BS, Joaquin Moya-Angeler, MD, Shivi Duggal, BS, MBA, Lester Zambrana, BA, Kara G. Fields, MS, Douglas N. Mintz, MD, and Charles N. Cornell, MD have declared that they have no conflict of interest. Joseph M. Lane, MD reports other from Bone Therapeutics, SA and Emcyte; personal fees and other from Grafty’s, ISTO and Kuros; personal fees from CollPlant Inc, outside the work.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Informed Consent
Informed consent was obtained from all patients for being included in the study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Additional information
Level of Evidence: III
Rights and permissions
About this article

Cite this article
Gianakos, A.L., Moya-Angeler, J., Duggal, S. et al. The Efficacy of Bisphosphonates with Core Decompression and Mesenchymal Stem Cells Compared with Bisphosphonates Alone in the Treatment of Osteonecrosis of the Hip: a Retrospective Study. HSS Jrnl 12, 137–144 (2016). https://doi.org/10.1007/s11420-016-9487-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-016-9487-7