
Abstract
Background
A review update is necessary to document evidence regarding the effectiveness of computer-tailored physical activity and nutrition education.
Purpose
The purpose of this study was to summarize the latest evidence on the effectiveness of computer-tailored physical activity and nutrition education, and to compare the results to the 2006 review.
Methods
Databases were searched for randomized controlled trials evaluating computer-tailored physical activity and nutrition education aimed at primary prevention in adults, published from September 2004 through June 2011.
Results
Compared to the findings in 2006, a larger proportion of studies found positive effects for computer-tailored programs compared to generic or no information, including those for physical activity promotion. Effect sizes were small and generally at short- or medium-term follow-up.
Conclusions
The results of the 2006 review were confirmed and reinforced. Future interventions should focus on establishing larger effect sizes and sustained effects and include more generic health education control groups and objective measurements of dietary behavior.
Similar content being viewed by others
Introduction
The potential impact of physical activity and healthy dietary habits on the prevention of a range of chronic conditions is substantial [1, 2]. Effective physical activity and dietary promotion interventions are needed. Successful intervention strategies and techniques to motivate and guide people to adopt healthy choices need to be identified. Over the last decades, computer tailoring has proven to be an innovative and promising health education technique [3–12]. A computer-tailored intervention mimics interpersonal counseling using a computerized process, but, unlike interpersonal counseling, it can be widely distributed through interactive media channels at a relatively low cost. Computer tailoring allows for individualized feedback and advice on personal behavior, personal motivation, outcome expectations, self-efficacy, social and physical environmental opportunities, and other behavioral determinants.
In recent years, a number of systematic reviews and meta-analyses have been published on the effectiveness of computer-tailored health education covering a range of behaviors [4, 5, 9, 10, 13, 14]. The effects of tailoring may, however, be behavior specific. It has been argued that computer tailoring may be especially promising for complex health behaviors, such as physical activity and dietary behaviors [15]. Examples of complex health behaviors are gaining increased awareness of personal behavioral patterns, comparing one's own behaviors with recommendations, and setting and monitoring progress toward behavior change goals. The first systematic review that explicitly focused on the effectiveness of computer-tailored health education on physical activity and dietary behaviors was published in 2006 and included intervention studies published up to September 2004 [3]. In concordance with other more narrative reviews on computer-tailored health education [15, 16], the authors concluded that computer tailoring was promising, especially for dietary behaviors, although the effect sizes were small. The authors made key recommendations for improving research on computer tailoring, i.e., using objective outcome measures instead of self-report or using generic health education comparison groups instead of or in addition to no-intervention control groups. The latter would allow more precise evaluation of the effects of tailoring health education interventions. Finally, it was concluded that longer follow-up was needed to assess the sustained effects in all studies.
Since many original studies have been published since 2004, a review update is needed to document evidence regarding the effectiveness of computer-tailored physical activity and nutrition education programs. Furthermore, responding to recommendations made in 2006, comparing effects and specific study and intervention characteristics over time, is additive to other systematic reviews and meta-analyses. This review update aims to: (1) review the evidence on computer-tailored physical activity and nutrition education from studies published since September 2004, (2) compare the evidence from this review update to that derived from the original review regarding intervention characteristics, study characteristics, and effects, and (3) provide updated recommendations for further research and practice.
Methods
This paper reports on a second systematic review conducted using the study protocol of the original 2006 review. This protocol was based on guidelines extracted from the Cochrane Reviewers' Handbook [17].
Search Strategy and Data Sources
For the original review, intervention studies published from 1965 to September 2004 were identified through a structured computerized search of PubMed, PsychInfo, and Web of Science. For this update, a nearly identical search was conducted from September 2004 to June 2011. The review differed from 2006 as we added the search engines' most recent thesaurus terms, resulting in the following search terms for nutrition: ((nutrition OR feeding OR food OR diet OR dietary OR intake OR nutritional status OR feeding behavi* OR food consumption) AND (education OR behavior OR behavio* OR education)) AND (tailored OR tailoring OR tailor* OR expert system) and for physical activity: (exercise OR motor activity OR sports OR leisure activities) OR (physical* AND active) OR (physical* AND activity) OR (physical* AND activities) OR exercis* OR walking OR cycling OR sport* OR leisure activit* AND (education OR behavior OR behavio* OR education) AND (tailored OR tailoring OR tailor* OR expert system). No limitations for age or study design were added.
Selection of Studies
Just as in the original 2006 review, new studies had to examine a computer-tailored intervention aimed at promoting healthy physical activity or dietary behaviors for primary prevention of chronic diseases in apparently healthy adults. Evaluation studies that used a randomized controlled trial were included. Tailoring was defined by Kreuter as “the intention to reach one specific person, based on characteristics that are unique to that person, are related to the outcome of interest, and have been derived from an individual assessment” [18]. Interventions were considered to be computer tailored if the tailored advice was generated through a computerized process. Randomized controlled trials were included if: (1) published in a peer-reviewed scientific journal, 2) published in English, and 3) conducted in an adult sample (18+ years). Studies were excluded if the tailored intervention was part of a larger intervention program that made it impossible to isolate the effect of tailoring components from the other intervention components.
Data Extraction
Detailed information was extracted only from new studies that met the aforementioned inclusion criteria. Two reviewers independently summarized the new studies for content and methods. The following intervention characteristics were extracted: theories used for intervention development, variables used to tailor the computer-tailored information, the “tool” that was used to provide individual feedback, frequency of tailored feedback, and additional health education activities. Extracted study characteristics were: the country where the study was conducted, size and source of the study population, eligibility criteria, intervention modes, and primary outcome measures. Results from single and multiple post-test measurements were extracted. The outcomes included all physical activity and dietary behavior measures. To interpret and compare results from the studies that used differing measures to assess physical activity and dietary outcomes, effect sizes (ESs) were calculated if significant effects were found (provided the data were available). The effect size, Cohen’s ES, was calculated by dividing the difference between two means at follow-up by their pooled standard deviation [19, 20]. Cutoff points for ESs were 0.2–0.5 for small ES, 0.5–0.8 for moderate ES, and >0.8 for large ES [21]. The findings were summarized per behavioral outcome (physical activity, fat intake, fruit and vegetable consumption, and other dietary behaviors) and separately for short- (<3 months), medium- (3–6 months), and long-term (>6 months) follow-up.
Apart from reporting the results found in the current review, we compared these with the results of the original 2006 review. In order to check whether recommendations from the original review were met, we compared intervention and study characteristics of the present review with the original one. Frequencies on the number of studies that found significant effects, as well as the number of studies that used objective outcome measures, various types of comparison groups (generic health education versus no-intervention control groups), and long-term follow-up, as well as delivery mode (printed versus electronically) are provided, linked to the original or current review.
Results
Study Selection
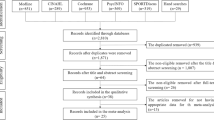
The initial cross-database search resulted in 2,590 publications. After eliminating duplicates, 1,562 remained. Titles and abstracts were reviewed for eligibility criteria, resulting in 141 publications that were fully considered. Fifty publications were finally included: 29 studies on physical activity and 34 on dietary behaviors, 21 on fat consumption, 18 on fruit and vegetable consumption, and 14 on other dietary topics. Other dietary topics included: energy/carbohydrate intake, the consumption of sugar, dairy, fiber, whole grain, and body fat, as well as weight and waist circumference. Thirteen studies in the current review evaluated interventions that targeted both physical activity and diet. Some publications reported on the characteristics and effects of one intervention using various follow-up measurements (e.g., short- and long-term effects) [22–26, 39], effects in a variety of study samples [27–30], effects on other types of outcomes (e.g., fruit intake and variety of fruit intake) [31], or the effects of various doses of the intervention (e.g., delivered at once or at multiple time points) [32, 33]. As a consequence, this review update reports on the characteristics and effects of 25 interventions targeted at physical activity, 27 interventions targeted at dietary behavior, and 10 interventions for both behaviors. Of the 27 interventions on dietary behavior, 17 were directed at fat reduction, 14 at increasing fruit and vegetable intake, and 12 at other dietary behaviors. The main reasons for exclusion were: the age of the study population was not in the required range, lack of randomized controlled trial design, no focus on primary prevention, absence of behavioral outcomes, or the computer tailoring was part of a multicomponent intervention that made it impossible to isolate the effect of tailoring.
Intervention Characteristics
Characteristics of the interventions from studies in the current review are summarized in the Electronic Supplementary Material. Both physical activity and nutrition education interventions were predominantly guided by the Transtheoretical Model and Social Cognitive Theory. Most interventions (81 % of physical activity, 84 % of nutrition) provided tailored feedback on self-reported behavior. Two interventions (4 %) also provided feedback based on more objective data obtained from pedometers [34] or accelerometers [35]. Most interventions (92 % of physical activity, 68 % of nutrition) were tailored on presumed behavioral determinants such as intention, motivation, and stage of change, as well as self-efficacy and skills. Regarding nutrition education interventions, equal numbers of interventions provided print-delivered and electronically tailored feedback; however, the majority of physical activity interventions used electronic feedback formats (see also Table 1). Some interventions using electronic feedback had additional online discussion/message boards [36–38] (6 % of all interventions) or an e-buddy system (2 % of all interventions) [22, 38]. Electronic feedback was given on-screen (41 % of all interventions), by email reports (10 %), CD-ROM (4 %), or by mobile phone (2 %). Approximately one third of the interventions provided additional information such as booklets or information sheets. One intervention included weekly home visits [26, 39]. Less than half of the interventions provided tailored feedback more than once for dietary behaviors (48 %), and 65 % did so for physical activity.
Study Characteristics
The characteristics and effects for studies in the current review are shown in the Appendix. The majority of studies were conducted in the USA, followed by the Netherlands and Belgium, the UK, and several other countries.
Studies in the USA predominantly assessed physical activity with the validated 7-day Physical Activity Recall [40–43]; this was the most commonly used tool. The next most common tool was the validated Short Questionnaire Assessing Health-Enhancing Physical Activity (SQUASH) [44] predominantly used by Dutch researchers. The International Physical Activity Questionnaire (IPAQ) [45, 46] was the third most commonly used assessment tool. Six studies (21 %) included objective assessments of physical activity, i.e., pedometer, actigraph, or accelerometer. Five studies (17 %) measured aerobic fitness by either a (1 mile) walking test [47, 48], the Chester step test [49], or the submaximal exercise treadmill test [50].
Fat reduction was most often assessed using food frequency questionnaires. In the USA, the Block questionnaire was used most frequently [51] and in the Netherlands, a questionnaire developed by Van Assema et al. [52]. Two studies obtained data from either an electronic scanner [53] or shopping receipts [34] in a supermarket setting. Data on fruit and vegetable consumption were obtained from questionnaires (the Block questionnaire in the majority of studies); one study also used shopping receipts [34]. Studies that included measures of weight or BMI either used self-report [38, 54] or measured [24, 27, 28, 34, 55, 56]. Fiber, grain, energy, or added sugar intakes were assessed by food frequency questionnaires [57, 58].
Effects on Physical Activity (Section A, Appendix)
Of the 29 studies on physical activity, 20 (69 %) showed significant differences in favor of the computer-tailored intervention. Five studies looked at short-term effects [36, 37, 59–61], of which four found significant effects for the tailored intervention [36, 37, 59, 60] with small effect sizes, compared to no intervention. In one study, this applied to participants who did not comply to the physical activity guidelines at baseline [60]. Of the 17 studies with medium-term follow-up periods, 12 found significant effects with small effect sizes: six compared to no intervention [22, 36, 62–65], five compared to generic health education [24, 32, 33, 66, 67], and one compared to a health risk assessment [67]. Studies that investigated two computer-tailoring techniques [22, 54, 63, 67] found significant effects for both tailoring conditions. Six of the 13 studies with long-term follow-up found significant effects of the tailored intervention [23, 25, 32, 34, 65, 67]. Effect sizes were small except for one study that reported medium effect size for one of the two computer-tailored interventions investigated [67]. Of the eight studies that assessed effects at various follow-up periods, four studies reported no effects at either short, medium, or long term [35, 61, 68, 69]; six studies reported sustained effects over time[22, 23, 25, 34, 36, 65, 67], and one study reported no effect at short term but a significant effect at medium term [62].
Effects on Fat Consumption (Section B, Appendix)
Of the 21 studies on fat consumption, 17 (81 %) showed significant differences in favor of the computer-tailored intervention. Six studies tested short-term effects and reported significant effects of tailoring compared to no intervention [36, 60, 70, 71], or generic health education [72, 73] with small effect sizes. Two of those studies (also) targeted an at-risk population [60, 72]. At medium term, all eight studies found significant effects compared to no intervention [36, 70, 74], or generic health education [33, 72–75]. One of those studies targeted a low-income ethnically diverse population [76], and a second study also found a significant effect among risk consumers (i.e., people with fat intake levels higher than recommended at baseline) [72]. Ten studies tested the long-term effects of an intervention, and five found significant effects for tailoring compared to no intervention [29, 30, 70] or generic health education [24, 32] with small effect sizes. Two of the ten studies (also) targeted high-risk populations [29, 30], and another study targeted women aged 50–69 years [24]. Multiple measurements in time were reported for seven studies, of which five studies reported sustained significant effects [25, 36, 70, 72, 73], one study reported a significant effect at short term [26] that was not sustained in the long term [39], and one study reported no effects at both medium- and long-term time periods [77].
Effects on Fruit and Vegetable Consumption (Section C, Appendix)
Of the 18 studies on fruit and vegetable consumption, 15 (83 %) showed significant differences in favor of the computer-tailored intervention. Two of these studies measured the short-term effects of a computer-tailored intervention, and both found significant effects compared to no intervention [36, 71] with small effect sizes in a general population. Six studies measured medium-term effects, of which five found significant effects compared to no intervention [36, 65, 78] or generic health education [33, 75] with small effect sizes. One study investigated the effects of two intervention conditions (either delivered in one or four installments) compared to generic health education and measured the effects of retailored feedback [75]. The latter measured the effect of retailored feedback provided in four installments. Eight of the 12 studies that tested the long-term effects of an intervention found significant effects for tailoring interventions compared to no intervention [31, 34, 65, 79] or generic health education [24, 32, 80, 81]. The eight studies found small effect sizes, except for one that had targeted church members, which found a large effect size over the long term [31]. Two studies with effective long-term interventions targeted populations who were over 50 years of age [24, 56]. Heimendinger and colleagues found a significant effect of (re)tailored advice when spread across four booklets, as opposed to no effect when the advice was delivered in a single booklet [81]. Nine studies reported multiple measurements in time, and seven of these reported sustained effects [25, 32, 34, 36, 65, 75, 78]. One of the nine studies reported no medium-term effect but a significant long-term effect [79], and one study reported no medium- or long-term effect [77].
Effects on Other Diet-Related Behaviors (Section D, Appendix)
Of the 14 studies on other dietary behaviors, 8 (57 %) showed significant differences in favor of the computer-tailored intervention. Four interventions for weight loss found significant effects including: one short, medium, and long term [28]; one medium and long term [38]; and two long term only [34, 55]. Effect sizes were small [34, 55], medium [28], or large [38]. Of the three interventions on energy intake, one reported a significant short- and medium-term effect [72]. The corresponding effect size was small for the general study population and medium among risk consumers in the short term. In addition, at medium term, only the effect of print-based advice (as opposed to delivery through CD-ROM) was of significance in the general population with a small effect size. Both studies considering fiber consumption found significant short-, medium- [70], and long-term effects [34] with small effect sizes. The intervention on grain intake showed no significant effect, nor did an intervention aimed at reducing added sugar. No significant effect was observed for the intervention to change dairy consumption [82].
A Comparison Between the Present Update and the Original 2006 Review
The present review included 50 publications over just under 7 years, while the original review in 2006 included 30 publications over 13 years, showing an apparent increase in studies on physical activity and tailored nutrition education. This increase was most obvious for physical activity (29 studies in the present review, 11 in the original review).
Since 2004, the number of computer-tailored interventions electronically delivered has increased, particularly in physical activity studies (see Table 1). New delivery modes, such as mobile phone and CD-ROM, were introduced since 2004. Similar to the original review, in the majority of studies included in the present update, a no-intervention control group was included without a generic health education comparison group. Most studies continue to lack objective assessments of effects of nutrition interventions, but physical activity intervention studies often used objective assessments for behavior changes. As recommended in the original 2006 review, more nutrition intervention studies included long-term follow-up.
In this update, the majority of studies reported significant effects of computer tailoring, both for dietary and physical activity behavior (the largest increase). However, effects sizes remained small in general for dietary as well as physical activity behavior.
Discussion
The present review update confirms and further strengthens the evidence that computer-tailored physical activity and nutrition education is likely to be effective [4, 5, 9, 10, 13, 14], although effect sizes related to tailored physical activity and nutrition education interventions are likely to be small. The evidence for long-term effects of computer tailoring remains inconclusive.
The present review is an update of a 2006 review of the literature published up to September 2004. A number of differences in the results of the original and updated review are noteworthy. First, both for physical activity and dietary behavior, the number of published studies has increased substantially. In addition, a larger proportion of published studies reported favorable effects of tailored interventions in the update period than in the original review. Evidence on the efficacy of computer-tailored education is now also apparent for physical activity promotion. Second, the use of objective outcome measurement instruments increased in studies on physical activity education, but not for nutrition education studies. Third, overall, there was no increase in comparisons of interventions with generic health education since 2004. Fourth, remarkably more studies with long-term follow-up were performed in the past years, particularly on nutrition education. Finally, the electronic delivery of feedback increased, particularly in studies on physical activity promotion; discussion boards/forums were frequently added to interventions.
The observed differences over time for the use of objective outcome measurements and various types of control groups, follow-up periods, and delivery modes require more attention. Since 2004, a larger number of objective measures have been included in tailoring studies, especially regarding physical activity education. In this field, accelerometers and pedometers have grown in popularity, due to increased usability and feasibility [83]. In the field of nutrition, no such development was seen. The objective measurement of dietary intake can be achieved by monitoring biologic dietary indicators, such as serum cholesterol and serum carotenoids [84]. However, the assessment of biologic indicators is relatively expensive, and these indicators are subject to genetic differences. Alternatively, two studies used shopping receipts and electronic shop scanners as objective indicators of food purchases [34, 53]. In addition, anthropometrics and waist circumference were the most frequent objective indicators.
The fact that the evidence in favor of computer-tailored physical activity and nutrition education is now stronger than based on the studies published up to 2004 is promising and important. However, the strongest evidence comes from studies that compared tailored interventions to no-intervention control groups. Thus, these studies could not assess the effects of tailoring compared to non-tailored interventions. Significant effects were most often found in studies with a no-intervention control group. These findings do not differ from the results of the original review or other comparable reviews [3, 6–8, 13]. Therefore, the evidence is stronger for a comparison between tailored interventions and with no intervention than with generic health education. However, this is probably because of the larger number of studies that included a no-intervention control group. If generic health education control groups were included in a study, the evidence was quite consistently in favor of tailoring. If this review had been restricted only to comparisons between tailored interventions with generic health education comparison groups, it would have focused specifically on the additional effects of tailoring in health education. Nevertheless, we believe that the comparison with no-intervention control conditions is also important, because it shows that tailored interventions are likely to be effective—because of the tailoring or other factors—and that is important information for health education practice. In addition, further exploration of the effectiveness of computer-tailored interventions compared to other control conditions, such as theory-based or personalized interventions, would be valuable to verify whether individually tailored education is better than theory-based and/or personalized education.
For physical activity and nutrition interventions to have an effect on health, the effects should be sustained over long periods of time [76]. The present review update shows that since 2004, more studies with long-term follow-up (>6 months) have been published. However, the positive effects of these studies were generally observed at short- and medium-term follow-up. Lack of long-term effects of health education interventions has been reported before. In a meta-analysis of computer-tailored interventions, Krebs and colleagues also found a significant trend of decreasing effect size when follow-up time increased [4]. Some evidence suggests that “dynamic tailoring” with more tailored feedback moments throughout a long intervention period may improve effects beyond the short term. The present updated review further shows that iterative feedback and tools supporting self-regulatory skills (e.g., goal setting activities, self-monitoring tools, skills building activities, email reminders, booster sessions, and interactive activities) are ways to realize such repeated tailoring [4, 5, 15, 85].
Not only has the number of electronically delivered interventions grown since 2004, but evidence for effectiveness has too. Before 2004, only a third of these “second-generation” dietary interventions were effective, compared to 60 % after 2004. For effective promotion of physical activity, the likelihood of effect appears not to be dependent on delivery mode. Furthermore, mobile phones were a delivery mode that was not yet available in the studies in the original 2006 review. A study by Haapala et al. indicates that mobile phone delivery can be an effective method for supporting weight loss. By allowing for two-way communication and showing a log-on frequency that is twice the rate of other web-based programs [86, 87], mobile phones have potential for the future. Because of these advantages and given the massive increase of the use of smartphones worldwide, mobile technologies will and probably should be used more often to promote lifestyle changes [88].
Overall, studies published since 2004 appear to have partially taken into account the recommendations for further research in the original review. Although more objective outcome measurement instruments were used in studies published after 2004, this was restricted to interventions on physical activity. Further, despite the increased number of studies, the proportion of comparisons with generic health education has not increased since 2004. Long follow-ups have been included more frequently in more recent studies, but only in nutrition interventions. Comparisons with generic health education, instead of no-intervention control groups, are most important because they provide information on the effects of tailoring. Therefore, we repeat and strongly advocate the recommendation to study tailoring as compared to other intervention methods, such as generic health education. Long-term follow-up should remain a priority, as well as the inclusion of objective outcome measures including their use in nutrition intervention research.
This review update has limitations. We used the same review protocol as was applied in the original 2006 review. Therefore, potential limitations such as the non-blinding of reviewers to authorship or the journal of the reviewed publications also applied to the present review. A lack of unequivocal scientific evidence that blinding is essential to obtain valid review results was already discussed in the original 2006 review [3, 89, 90]. In addition, a new independent reviewer assessed eligibility of the studies for the present update, which could have led to some differences in decisions and interpretations. Previous research has shown that updating a review can affect both the direction and the precision of the outcome [91, 92]. Yet, two reviewers who were involved in the reviewing process of the original 2006 review were also part of the present update team. No risk of bias and/or quality assessment evaluations were performed for either the original and updated review, although the use of such tools has been recommended for systematic reviews [17]. Fortunately, because only randomized controlled trials were included, the variety in methodological quality was small. Nevertheless, the methodological quality of the studies included in this review could have had an impact on estimates of effects, which might have affected the validity of the conclusions. Finally, as with any review of published literature, the present update may have been affected by publication bias that may have caused an overestimation of the positive findings.
Notwithstanding these potential limitations, this review importantly updates the systematic overview of developments and evidence regarding computer-tailored physical activity and nutrition education over the past years. Furthermore, this review update provides the most recent overview of the content and effects of computer-tailored interventions in the field of physical activity and nutrition. Reviews of the literature need to be updated regularly in order to provide up-to-date overviews of the evidence base to inform health promotion practice and to provide new recommendations for research to further strengthen the evidence base. This comparison is strengthened by our use of comparable reviewing methods at two time points, 2006 and 2011, giving us the opportunity to compare effects, intervention, and study characteristics over time. Such updating of reviews using a similar methodology is advocated and common practice in review consortia such as the Cochrane collaboration.
On the whole, from this updated review, it can be concluded that the evidence on computer-tailored interventions for the promotion of physical activity and dietary change has become stronger and now is also convincing for physical activity promotion. However, this effect particularly accounted for studies with no-intervention control groups, effect sizes were generally small, and the evidence is generally restricted to rather short-term effects, i.e., up to 3 months follow-up. Further, it remains unclear whether the effect of tailored interventions is caused by tailoring as such or by the fact that tailored interventions are more likely to be carefully designed and based on behavioral theory. Previously formulated recommendations regarding the use of objective outcome measurements, generic HE control groups, and long-term follow-up periods for the development of computer-tailored interventions were only partially met. Based on the present review, the use of computer-tailored interventions in physical activity and healthy nutrition promotion can be advocated, but future interventions should especially focus on: (1) establishing larger effect sizes and sustained effects, (2) using more objective measurements in studies on dietary behavior, (3) using more generic HE control groups and especially control groups in which the generic health education is also carefully designed and theory-based in order to distinguish the effect of tailoring from the effects of theory-based intervention development, and (4) including more long-term follow-up measurements. Future research should also focus on why and how computer-tailored physical activity and nutrition interventions are effective, by conducting mediation analyses [23, 93], and supporting large-scale dissemination of such interventions [94].
References
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347-60.
Hooper L, Summerbell CD, Higgins JP, et al. Dietary fat intake and prevention of cardiovascular disease: Systematic review. BMJ. 2001;322:757-63.
Kroeze W, Werkman A, Brug J. A systematic review of randomized trials on the effectiveness of computer-tailored education on physical activity and dietary behaviors. Ann Behav Med. 2006;31:205-23.
Krebs P, Prochaska JO, Rossi JS. A meta-analysis of computer-tailored interventions for health behavior change. Prev Med. 2010;51:214-21.
Lustria ML, Cortese J, Noar SM, Glueckauf RL. Computer-tailored health interventions delivered over the Web: Review and analysis of key components. Patient Educ Couns. 2009;74:156-73.
Neville LM, O'Hara B, Milat A. Computer-tailored physical activity behavior change interventions targeting adults: A systematic review. Int J Behav Nutr Phys Act. 2009;6:30.
Neville LM, Milat AJ, O'Hara B. Computer-tailored weight reduction interventions targeting adults: A narrative systematic review. Health Promot J Austr. 2009;20:48-57.
Neville LM, O'Hara B, Milat AJ. Computer-tailored dietary behaviour change interventions: A systematic review. Health Educ Res. 2009;24:699-720.
Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol Bull. 2007;133:673-93.
Noar SM, Grant Harrington N, Shemanksi Aldrich R. The role of message tailoring in the development of persuasive health communication messages. In: Beck CS, ed. Communication Yearbook 33. Routledge, 2009:73-133.
Eyles HC, Mhurchu CN. Does tailoring make a difference? A systematic review of the long-term effectiveness of tailored nutrition education for adults. Nutr Rev. 2009;67:464-80.
Yap TL, Davis LS. Physical activity: The science of health promotion through tailored messages. Rehabil Nurs. 2008;33:55-62.
Enwald HP, Huotari ML. Preventing the obesity epidemic by second generation tailored health communication: An interdisciplinary review. J Med Internet Res. 2010;12:e24.
Portnoy DB, Scott-Sheldon LA, Johnson BT, Carey MP. Computer-delivered interventions for health promotion and behavioral risk reduction: A meta-analysis of 75 randomized controlled trials, 1988-2007. Prev Med. 2008;47:3-16.
Brug J, Oenema A, Campbell M. Past, present, and future of computer-tailored nutrition education. Am J Clin Nutr. 2003;77:1028S-34S.
Skinner CS, Campbell MK, Rimer BK, Curry S, Prochaska JO. How effective is tailored print communication? Ann Behav Med. 1999;21:290-8.
Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration, 2011.
Kreuter MW, Strecher VJ, Glassman B. One size does not fit all: The case for tailoring print materials. Ann Behav Med. 1999;21:276-83.
Cohen J. Statistical Power Analysis for the Behavioural Sciences. New York: Academic; 1977.
Cohen JA. Power primer. Psychol Bull. 1992;112:155-159.
Mullen PD, Simons-Morton DG, Ramirez G, Frankowski RF, Green LW, Mains DA. A meta-analysis of trials evaluating patient education and counseling for three groups of preventive health behaviors. Patient Educ Couns. 1997;32:157-73.
van Stralen MM, de Vries H, Mudde AN, Bolman C, Lechner L. Efficacy of Two Tailored Interventions Promoting Physical Activity in Older Adults. Am J Prev Med. 2009;37:405-17.
van Stralen MM, de Vries H, Mudde AN, Bolman C, Lechner L. The long-term efficacy of two computer-tailored physical activity interventions for older adults: Main effects and mediators. Health Psychol. 2011;30:442-52.
Walker SN, Pullen CH, Boeckner L, et al. Clinical trial of tailored activity and eating newsletters with older rural women. Nurs Res. 2009;58:74-85.
Walker SN, Pullen CH, Hageman PA, et al. Maintenance of activity and eating change after a clinical trial of tailored newsletters with older rural women. Nurs Res. 2010;59:311-21.
Elder JP, Ayala GX, Campbell NR, et al. Interpersonal and print nutrition communication for a Spanish-dominant Latino population: Secretos de la Buena Vida. Health Psychol. 2005;24:49-57.
Tanaka M, Adachi Y, Adachi K, Sato C. Effects of a non-face-to-face behavioral weight-control program among Japanese overweight males: A randomized controlled trial. Int J Behav Med. 2010;17:17-24.
Adachi Y, Sato C, Yamatsu K, Ito S, Adachi K, Yamagami T. A randomized controlled trial on the long-term effects of a 1-month behavioral weight control program assisted by computer tailored advice. Behav Res Ther. 2007;45:459-70.
Prochaska JO, Velicer WF, Rossi JS, et al. Multiple risk expert systems interventions: Impact of simultaneous stage-matched expert system interventions for smoking, high-fat diet, and sun exposure in a population of parents. Health Psychol. 2004;23:503-16.
Prochaska JO, Velicer WF, Redding C, et al. Stage-based expert systems to guide a population of primary care patients to quit smoking, eat healthier, prevent skin cancer, and receive regular mammograms. Prev Med. 2005;41:406-16.
Do M, Kattelmann K, Boeckner L, et al. Low-income young adults report increased variety in fruit and vegetable intake after a stage-tailored intervention. Nutr Res. 2008;28:517-22.
de Vries H, Kremers SPJ, Smeets T, Brug J, Eijmael K. The effectiveness of tailored feedback and action plans in an intervention addressing multiple health behaviors. Am J Health Promot. 2008;22:417-25.
Smeets T, Kremers SPJ, Brug J, de Vries H. Effects of tailored feedback on multiple health behaviors. Ann Behav Med. 2007;33:117-23.
Winett RA, Anderson ES, Wojcik JR, Winett SG, Bowden T. Guide to health: Nutrition and physical activity outcomes of a group-randomized trial of an Internet-based intervention in churches. Ann Behav Med. 2007;33:251-61.
Slootmaker SM, Chinapaw MJM, Schuit AJ, Seidell JC, van Mechelen W. Feasibility and effectiveness of online physical activity advice based on a personal activity monitor: Randomized controlled trial. J Med Internet Res. 2009;11:e27.
Sternfeld B, Block C, Quesenberry CPJ, et al. Improving diet and physical activity with ALIVE: A worksite randomized trial. Am J Prev Med. 2009;36:475-83.
Hurling R, Catt M, Boni MD, et al. Using internet and mobile phone technology to deliver an automated physical activity program: Randomized controlled trial. J Med Internet Res. 2007;9:e7.
Rothert K, Strecher VJ, Doyle LA, et al. Web-based weight management programs in an integrated health care setting: A randomized, controlled trial. Obesity (Silver Spring). 2006;14:266-72.
Elder JP, Ayala GX, Campbell NR, et al. Long-term effects of a communication intervention for Spanish-dominant Latinas. Am J Prev Med. 2006;31:159-66.
Hellman EA, Williams MA, Thalken L. Modifications of the 7-Day Activity Interview for Use Among Older Adults. J Appl Gerontol. 1996;15:116-32.
Hayden-Wade HA, Coleman KJ, Sallis JF, Armstrong C. Validation of the telephone and in-person interview versions of the 7-day PAR. Med Sci Sports Exerc. 2003;35:801-9.
Sallis JF, Haskell WL, Wood PD, et al. Physical activity assessment methodology in the Five-City Project. Am J Epidemiol. 1985;121:91-106.
Blair SN, Haskell WL, Ho P, et al. Assessment of habitual physical activity by a seven-day recall in a community survey and controlled experiments. Am J Epidemiol. 1985;122:794-804.
Wendel-Vos GC, Schuit AJ, Saris WH, Kromhout D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol. 2003;56:1163-9.
Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381-95.
Rosenberg DE, Bull FC, Marshall AL, Sallis JF, Bauman AE. Assessment of sedentary behavior with the International Physical Activity Questionnaire. J Phys Act Health. 2008;5(Suppl 1):S30-S44.
Kline GM, Porcari JP, Hintermeister R, et al. Estimation of VO2max from a one-mile track walk, gender, age, and body weight. Med Sci Sports Exerc. 1987;19:253-9.
Hageman PA, Walker SN, Pullen CH, Pellerito P. Test-Retest Reliability of the Rockport Fitness Walking Test and Other Fitness Measures in Women Ages 50-69 Years. J Geriatr Phys Ther 2001;24.
Buckley JP, Sim J, Eston RG, Hession R, Fox R. Reliability and validity of measures taken during the Chester step test to predict aerobic power and to prescribe aerobic exercise. Br J Sports Med. 2004;38:197-205.
Morris M, Lamb KL, Hayton J, Cotterrell D, Buckley J. The validity and reliability of predicting maximal oxygen uptake from a treadmill-based sub-maximal perceptually regulated exercise test. Eur J Appl Physiol. 2010;109:983-8.
Block G, Hartman AM, Naughton D. A reduced dietary questionnaire: Development and validation. Epidemiology. 1990;1:58-64.
Van Assema P, Brug J, Ronda G, Steenhuis I. The relative validity of a short Dutch questionnaire as a means to categorize adults and adolescents to total and saturated fat intake. J Hum Nutr Diet. 2001;14:377-90.
Ni Mhurchu C, Blakely T, Jiang Y, Eyles HC, Rodgers A. Effects of price discounts and tailored nutrition education on supermarket purchases: A randomized controlled trial. Am J Clin Nutr. 2010;91:736-47.
Prochaska JO, Butterworth S, Redding CA, et al. Initial efficacy of MI, TTM tailoring and HRI's with multiple behaviors for employee health promotion. Prev Med. 2008;46:226-31.
Haapala I, Barengo NC, Biggs S, Surakka L, Manninen P. Weight loss by mobile phone: A 1-year effectiveness study. Public Health Nutr. 2009;12:2382-91.
Werkman A, Hulshof PJ, Stafleu A, et al. Effect of an individually tailored one-year energy balance programme on body weight, body composition and lifestyle in recent retirees: A cluster randomised controlled trial. BMC Public Health. 2010;10:110.
Feunekes GI, Van Staveren WA, De Vries JH, Burema J, Hautvast JG. Relative and biomarker-based validity of a food-frequency questionnaire estimating intake of fats and cholesterol. Am J Clin Nutr. 1993;58:489-96.
Feunekes IJ, Van Staveren WA, Graveland F, De VJ, Burema J. Reproducibility of a semiquantitative food frequency questionnaire to assess the intake of fats and cholesterol in The Netherlands. Int J Food Sci Nutr. 1995;46:117-23.
Quintiliani LM, Campbell MK, Bowling JM, Steck S, Haines PS, DeVellis BM. Results of a randomized trial testing messages tailored to participant-selected topics among female college students: Physical activity outcomes. J Phys Act Health. 2010;7:517-26.
Oenema A, Brug J, Dijkstra A, de Weerdt I, de Vries H. Efficacy and use of an internet-delivered computer-tailored lifestyle intervention, targeting saturated fat intake, physical activity and smoking cessation: A randomized controlled trial. Ann Behav Med. 2008;35:125-35.
Wanner M, Martin-Diener E, Braun-Fahrlander C, Bauer G, Martin BW. Effectiveness of active-online, an individually tailored physical activity intervention, in a real-life setting: Randomized controlled trial. J Med Internet Res. 2009;11:e23.
Dunton GF, Robertson TP. A tailored Internet-plus-email intervention for increasing physical activity among ethnically-diverse women. Prev Med. 2008;47:605-11.
Spittaels H, De Bourdeaudhuij I, Vandelanotte C. Evaluation of a website-delivered computer-tailored intervention for increasing physical activity in the general population. Prev Med. 2007;44:209-17.
Smeets T, Brug J, de Vries H. Effects of tailoring health messages on physical activity. Health Educ Res. 2008;23:402-13.
van Keulen HM, Mesters I, Ausems M, et al. Tailored print communication and telephone motivational interviewing are equally successful in improving multiple lifestyle behaviors in a randomized controlled trial. Ann Behav Med. 2011;41:104-18.
Hageman PA, Walker SN, Pullen CH. Tailored versus standard internet-delivered interventions to promote physical activity in older women. J Geriatr Phys Ther. 2005;28:28-33.
Marcus BH, Napolitano MA, King AC, et al. Telephone versus print delivery of an individualized motivationally tailored physical activity intervention: Project STRIDE. Health Psychol. 2007;26:401-9.
Napolitano MA, Whiteley JA, Papandonatos G, et al. Outcomes from the women's wellness project: A community-focused physical activity trial for women. Prev Med. 2006;43:447-53.
Marcus BH, Lewis BA, Williams DM, et al. A comparison of Internet and print-based physical activity interventions. Arch Intern Med. 2007;167:944-9.
Fries E, Edinboro P, McClish D, et al. Randomized trial of a low-intensity dietary intervention in rural residents: The Rural Physician Cancer Prevention Project. Am J Prev Med. 2005;28:162-8.
Blair Irvine A, Ary DV, Grove DA, Gilfillan-Morton L. The effectiveness of an interactive multimedia program to influence eating habits. Health Educ Res. 2004;19:290-305.
Kroeze W, Oenema A, Campbell M, Brug J. The efficacy of Web-based and print-delivered computer-tailored interventions to reduce fat intake: Results of a randomized, controlled trial. J Nutr Educ Behav. 2008;40:226-36.
Kroeze W, Oenema A, Dagnelie PC, Brug J. Examining the minimal required elements of a computer-tailored intervention aimed at dietary fat reduction: Results of a randomized controlled dismantling study. Health Educ Res. 2008;23:880-91.
De Bourdeaudhuij I, Stevens V, Vandelanotte C, Brug J. Evaluation of an interactive computer-tailored nutrition intervention in a real-life setting. Ann Behav Med. 2007;33:39-48.
Gans KM, Risica PM, Strolla LO, et al. Effectiveness of different methods for delivering tailored nutrition education to low income, ethnically diverse adults. Int J Behav Nutr Phys Act. 2009;6:24.
Glasgow RE, Klesges LM, Dzewaltowski DA, Bull SS, Estabrooks P. The future of health behavior change research: What is needed to improve translation of research into health promotion practice? Ann Behav Med. 2004;27:3-12.
Dutton GR, Napolitano MA, Whiteley JA, Marcus BH. Is physical activity a gateway behavior for diet? Findings from a physical activity trial. Prev Med. 2008;46:216-21.
Nitzke S, Kritsch K, Boeckner L, et al. A stage-tailored multi-modal intervention increases fruit and vegetable intakes of low-income young adults. Am J Health Promot. 2007;22:6-14.
Kreuter MW, Sugg-Skinner C, Holt CL, et al. Cultural tailoring for mammography and fruit and vegetable intake among low-income African-American women in urban public health centers. Prev Med. 2005;41:53-62.
Alexander GL, McClure JB, Calvi JH, et al. A randomized clinical trial evaluating online interventions to improve fruit and vegetable consumption. Am J Public Health. 2010;100:319-26.
Heimendinger J, O'Neill C, Marcus AC, et al. Multiple tailored messages are effective in increasing fruit and vegetable consumption among callers to the cancer information service. J Health Commun. 2005;10:65-82.
Poddar KH, Hosig KW, Anderson ES, Nickols-Richardson SM, Duncan SE. Web-based nutrition education intervention improves self-efficacy and self-regulation related to increased dairy intake in college students. J Am Diet Assoc. 2010;110:1723-7.
The Handbook of Health Behavior Change. New York: Springer Publishing Company, 2009.
Babor TF, Sciamanna CN, Pronk NP. Assessing multiple risk behaviors in primary care. Screening issues and related concepts. Am J Prev Med. 2004;27:42-53.
Brug J, Steenhuis I, Van AP, Glanz K, De Vries H. Computer-tailored nutrition education: Differences between two interventions. Health Educ Res. 1999;14:249-56.
Tate DF, Wing RR, Winett RA. Using Internet technology to deliver a behavioral weight loss program. JAMA. 2001;285:1172-7.
Harvey-Berino J, Pintauro S, Buzzell P, et al. Does using the Internet facilitate the maintenance of weight loss? Int J Obes Relat Metab Disord. 2002;26:1254-60.
Soureti A, Murray P, Cobain M, Chinapaw M, van MW, Hurling R. Exploratory study of web-based planning and mobile text reminders in an overweight population. J Med Internet Res. 2011;13:e118.
Van Rooyen S, Godlee F, Evans S, Smith R, Black N. Effect of blinding and unmasking on the quality of peer review. J Gen Intern Med. 1999;14:622-4.
Davidoff F. Masking, blinding, and peer review: The blind leading the blinded. Ann Intern Med. 1998;128:66-8.
McInnes E, Duf L, McClarey M. Challenges in updating a systematic review. Nursing Times Res. 1999;4:66-71.
Stead LF, Lancaster T, Silagy CA. Updating a systematic review--what difference did it make? Case study of nicotine replacement therapy. BMC Med Res Methodol. 2001;1:10.
van Stralen MM, de Vries H, Mudde AN, Bolman C, Lechner L. The working mechanisms of an environmentally tailored physical activity intervention for older adults: A randomized controlled trial. Int J Behav Nutr Phys Act 2009;6.
Brouwer W, Kroeze W, Crutzen R, et al. Which intervention characteristics are related to more exposure to internet-delivered healthy lifestyle promotion interventions? A systematic review. J Med Internet Res. 2011;13:e2.
Jacobs AD, Ammerman AS, Ennett ST, et al. Effects of a Tailored Follow-Up Intervention on Health Behaviors, Beliefs, and Attitudes. Journal of Women's Health. 2004;13:557-68.
Carroll JK, Lewis BA, Marcus BH, Lehman EB, Shaffer ML, Sciamanna CN. Computerized tailored physical activity reports a randomized controlled trial. Am J Prev Med. 2010;39:148-56.
Pekmezi DW, Neighbors CJ, Lee CS, et al. A culturally adapted physical activity intervention for Latinas: A randomized controlled trial. Am J Prev Med. 2009;37:495-500.
Spittaels H, De Bourdeaudhuij I, Brug J, Vandelanotte C. Effectiveness of an online computer-tailored physical activity intervention in a real-life setting. Health Educ Res. 2007;22:385-96.
Chinapaw MJ, Slootmaker SM, Schuit AJ. van ZM, van MW. Reliability and validity of the Activity Questionnaire for Adults and Adolescents (AQuAA). BMC Med Res Methodol. 2009;9:58.
Liu RD, Buffart LM, Kersten MJ, et al. Psychometric properties of two physical activity questionnaires, the AQuAA and the PASE, in cancer patients. BMC Med Res Methodol. 2011;11:30.
Acknowledgments
We gratefully acknowledge René Otten of the VU University Medical Library for his assistance in searching the databases.
Conflict of Interest
The authors have no conflict of interest to disclose.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material: Intervention Characteristics
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 53 kb)
Appendix
Appendix
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Broekhuizen, K., Kroeze, W., van Poppel, M.N. et al. A Systematic Review of Randomized Controlled Trials on the Effectiveness of Computer-Tailored Physical Activity and Dietary Behavior Promotion Programs: an Update. ann. behav. med. 44, 259–286 (2012). https://doi.org/10.1007/s12160-012-9384-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-012-9384-3