
Abstract
Some decellularized musculoskeletal extracellular matrices (ECM)s derived from tissues such as bone, tendon and fibrocartilaginous meniscus have already been clinical use for tissue reconstruction. Repair of articular cartilage with its unique zonal ECM architecture and composition is still an unsolved problem, and the question is whether allogenic or xenogeneic decellularized cartilage ECM could serve as a biomimetic scaffold for this purpose.
Hence, this survey outlines the present state of preparing decellularized cartilage ECM-derived scaffolds or composites for reconstruction of different cartilage types and of reseeding it particularly with mesenchymal stromal cells (MSCs).
The preparation of natural decellularized cartilage ECM scaffolds hampers from the high density of the cartilage ECM and lacking interconnectivity of the rather small natural pores within it: the chondrocytes lacunae. Nevertheless, the reseeding of decellularized ECM scaffolds before implantation provided superior results compared with simply implanting cell-free constructs in several other tissues, but cartilage recellularization remains still challenging. Induced by cartilage ECM-derived scaffolds MSCs underwent chondrogenesis.
Major problems to be addressed for the application of cell-free cartilage were discussed such as to maintain ECM structure, natural chemistry, biomechanics and to achieve a homogenous and stable cell recolonization, promote chondrogenic and prevent terminal differentiation (hypertrophy) and induce the deposition of a novel functional ECM. Some promising approaches were proposed including further processing of the decellularized ECM before recellularization of the ECM with MSCs, co-culturing of MSCs with chondrocytes and establishing bioreactor culture e.g. with mechanostimulation, flow perfusion pressure and lowered oxygen tension.

Synopsis of tissue engineering approaches based on cartilage-derived ECM
Similar content being viewed by others


Introduction
Cartilage tissue is characterized by low cell content, low supply of nutrients and progenitor cells, lacking blood vessels, neurons and lymphatic drainage. These facts altogether result in a very limited intrinsic regenerative capacity of the tissue [1]. Reconstruction of damaged cartilage irrespective of its localization in the body remains so far unsatisfying. Current surgical techniques applied concerning joint cartilage damage such as arthroscopic debridement and lavage, subchondral bone microfracture, osteochondral transplantation (OATS) and autologous chondrocyte implantation (ACI) [2–6] do not allow functionally restoring cartilage. Poor joint cartilage repair often leads to the onset of osteoarthritis (OA) [7, 8], which is characterized by an imbalance between anabolic and catabolic processes in synovial joints [9]. In the intervertebral disc (IVD) weak intrinsic cartilage repair capacity leads to IVD degeneration and chronic back pain [10]. Tissue engineering techniques rise hope to develop improved cartilage repair strategies.
For tissue engineering, cells have to be seeded on a temporary scaffold to establish a three-dimensional (3D) ECM structure that retains the seeded cells and provides mechanical support to aid the development of cartilage over time. Thus, scaffold biomaterials must be biodegradable, cyto−/biocompatible, mechanically competent (i.e., similar to surrounding tissue), and capable of regulating cell activity, shaping into different sizes and forms for resurfacing partial- or full-thickness lesions [11]. Various synthetic and natural polymer-based scaffolds have been developed and used for cartilage reconstruction, including four primary groups like protein-based polymers (e.g. fibrin, collagen), mainly carbohydrate-based polymers (e.g. hyaluronic acid, alginate, chitosan), synthetic polymers (e.g. Polylactic acid [PLA], Polyglycolic acid [PGA], Polycaprolactone [PCL], Polylactic-co-glycolic acid [PLGA]), Polyurethane or composite polymers (e.g. collagen, silk, PLGA) [12, 13]. Cells colonizing these scaffolds need a long time to produce sufficient ECM. Therefore, cell seeded polymer scaffolds generally require substantial time to undergo tissue morphogenesis and remodeling under appropriate environmental conditions for gaining adequate mechanical properties [14–18].
Furthermore, the restoration of the microarchitecture and zonality of a given tissue that has to be artificially replaced remains challenging particular in the case of cartilage.
The usage of a natural cell-free cartilage ECM as a scaffold allows recruiting allogeneic and xenogeneic donor tissue sources and circumvents many of the restrictions mentioned above. The blank ECM usually presents only a low immunogenicity and is, therefore, ideal for implantation. Although several allogeneic ECM scaffolds have successfully been used in both animal studies and human clinical studies for the repair or regeneration of various tissue defects, until today, a limited number of attempts have been made to prepare xenogeneic ECM scaffolds for cartilage repair [19, 20].
There exist, so far, different approaches in utilizing cell-free ECM – both, mature or immature tissue-derived ECMs, but also ECMs produced by cultured cells in vitro can serve as a basis for decellularized scaffolds. Moreover, hybrid scaffolds have been designed consisting of artificially prepared synthetic or natural components, which were combined with a natural decellularized ECM as a functionalization strategy to improve cytocompatibility [21].
In many cases, the cell-free ECMs were optimized by combining them with cells in vitro before implantation [19]. Nevertheless, there exist several approaches focussing on different cell types and reseeding strategies.
Stem cells are promising candidates for cartilage repair due to their characteristics. Some studies suggest a role for mesenchymal stromal cells (MSCs) derived from bone marrow, synovium, or other tissue sources that can subsequently produce sufficient autologous or allogeneic tissue cells suitable for use in single-stage surgical intervention [22–25].
This review will focus on current experimental approaches and factors, which are essential for developing functional decellularized ECMs to support repair of different cartilage species. It will present various types of cartilage ECM-derived scaffolds for cartilage tissue engineering. In addition, it discusses the particular perspective of using MSCs for reseeding these natural cartilage scaffolds and it addresses so far published in vivo studies based on cartilage-derived ECM.
Cartilage and Cartilage Repair
At a glance cartilage tissue appears to be simply structured consisting of only one cell type (chondrocytes or fibrochondrocytes) and an abundant ECM. It can generally be defined as an internal support tissue high in fibrous proteins (mainly type II collagen) and water-binding, mostly sulfated glycosaminoglycans (sGAG) [26]. Based on the histological contribution, quality and distribution of fibers within the ECM, cartilage has been classified as hyaline cartilage, elastic cartilage, and fibrocartilage [27]. However, the ECM is of particular functional importance in this tissue since it represents more than 90 % of the tissue volume. This ECM has a filigree collagen fiber arrangement and a histo-architecture reflecting distinct zones detectable, not only in joint cartilage, but also in other cartilage species such as IVD, enthesis or meniscus fibrocartilage, but less thoroughly characterized. This unique zonal architecture is an intriguing argument for using decellularized articular cartilage ECM scaffolds for joint cartilage reconstruction, because they could present exactly this stratified structure. So far no artificial scaffold manufactured from either natural, synthetic or as a composite of different polymers can mimic all aspects of this structure, which is highly important for biomechanics.
Hyaline Cartilage Reconstruction
Hyaline cartilage is an ECM-rich tissue primarily consisting of type II collagen and the large proteoglycan aggrecan [28]. The functions of hyaline articular cartilage ECM, as a prerequisite for stable movement, are to allow permanent repetitive copression by evenly distributing the load on the joint surface and to provide only minimal friction [29]. Hyaline cartilage was thoroughly studied for its developmental role for forming the template for most of the major bones of the body and the cartilaginous joint interfaces. At the articulating surfaces in the joint, hyaline cartilage is retained during maturation and prone to traumatic injury or affected by OA [30]. Hyaline articular cartilage reconstruction is a complicated issue in the treatment of traumatic joint cartilage defects, but it is also an important topic in the area of head-neck surgeries where larynx, tracheal or nasoseptal cartilage is malformed or can be damaged by traumatic injury, tumor resection, toxic agents, radiation or prolonged intubation. Furthermore, it has also to be reconstructed e.g. for trachea replacement [31], laryngeal cartilage repair [32, 33] and treatment of nasoseptal cartilage defects [19].
In selected cases, facet joint cartilage of the spine should be substituted [34]. Reconstruction of the nasoseptal, tracheal and laryngeal hyaline cartilage components presents particular requirements since a perichondrium covers the cartilage, which possesses, attached to a basal lamina, an interface to the respiratory epithelium mediating clearance functions. These layers and possibly, subepithelial glands have also to be reconstructed. The perichondrium is of particular importance since it serves additionally as an immunological barrier [35]. Meanwhile, several approaches have been developed to utilize decellularized cartilage for reconstruction of these hyaline cartilage types to be discussed later in this review.
Elastic Cartilage Reconstruction
Elastic cartilage is identified in only a few locations within the human body such as the auricle, the external ear canal, eustachian tube, parts of the laryngeal cartilage such as arytenoid cartilage and epiglottis [36, 37]. Reconstruction of the auricle has to be undertaken in cases of traumatic injury or developmental malformation such as microtia. So far, the source of chondrocytes for elastic cartilage reconstruction relies on rib-derived or elastic cartilage grafted from the auricle [38, 39]. However, donor site morbidity is commonly observed while maintance of these tissues for grafting remains a significant issue [40]. Elastic chondrocytes might lose their capacity to synthesize and form elastic fibers in vitro [18]. Recently, a natural ECM scaffold of the auricle was produced by decellularization of a whole ear [41]. Elastic fibers were retained in this decellularized ECM. MSCs, which were cultured within this scaffold were able to undergo chondrogenesis [41].
Fibrocartilage Reconstruction
Tissue engineering for the replacement of fibrocartilage is another intriguing topic in regenerative medicine. Notably, reconstruction of IVD remains a major challenge [42, 43], whereby replacement of both the IVD using recellularized tissues, the nucleus pulposus (NP) [44–46] and annulus fibrosus (AF) [47] has to be addressed separately. At this moment, also the zonal architecture in the IVD should be considered [48].
Another great topic in orthopedic surgery is the replacement of meniscus fibrocartilage. Loss of meniscal tissue by traumatic injury increases the contact pressure in the knee joint cartilage and results in instability, which leads to OA. The 3D crossing fiber pattern of the natural meniscus is unique and significantly challenging to reconstruct [49].
Meanwhile, some efforts have been undertaken to utilize decellularized meniscus allo−/xenografts and to reseed them with different chondrogenic cells [50–54]. The meniscus ECM exerts a chondroinductive effect on MSCs [52]. The reconstruction of a fibrocartilaginous enthesis for stable implantation of tissue-engineered tendon and ligament constructs is an important future issue: in response to tendon/ligament injury and reconstruction, the enthesis is not sufficiently restored, leading to inferior biomechanics and the risk of loosing [55]. The enthesis has a zonal structure consisting of ligamentous, non-calcified fibrocartilaginous, calcified fibrocartilaginous and bony parts [56]. The dimension varies dependent on the localization of the enthesis [57]. However, the use of decellularized native tissue for enthesis reconstruction has not been reported so far, but a recent study describes the establishment of tissue-specific tendon and bone regions on a degradable scaffold, using ECM produced by NIH 3T3 fibroblasts and MC 3T3 osteoblast [58]. Ongoing studies on enthesis decellularization will be published in near future.
Protocols and Methods in Cartilage Decellularization
Approaches for tissue decellularization have been discussed previously [59], but have so far not explicity detailed cartilage ECM preparation. A wide variety of decellularization techniques have been investigated for cell lysis via physical (e.g. freeze/thaw cycles), osmotic (e.g. deionized water), chemical (e.g. SDS or Triton X-100) and enzymatic treatments (e.g. trypsin, DNAse) [60, 61] (Table 1). Most of the protocols are combined multistep procedures and often time-consuming.
Due to the high density of cartilage, the native tissue structure has to be partly disrupted for increasing the efficiency of chemical decellularization, which allows the ECM to be more effectively exposed to the chemical reagents for a particular duration of time e.g. by physical (e.g. sonication) or enzymatic treatment (Table 1 ). In several cases, scaffolds were prepared from cartilage, which were shattered before decellularized [52, 62, 63]. Typically the first step in decellularization consists of cell lysis followed by extraction of various cellular debris by using detergents. Processing the tissue mechanically at first may allow a shorter exposure time to the chemical reagents, which is usually beneficial for the retention of the microstructure including sGAG and type II collagen concentration [61]. Nevertheless, each decellularization processing step aimed to remove cell remnants will, to some degree, alter the native 3D structure of the ECM [60] (Table 2). The most commonly utilized methods for decellularization of tissues include a combination of physical and chemical treatments (Table 1). The physical treatments can consist of agitation or ultrasonication [64], mechanical massage or pressure [65, 66], or repetitive freezing and thawing [67–71]. These methods mechanically disrupt the cell membrane, allow the release of cell contents, and facilitate subsequent rinsing and removal of the cell remnants from the ECM. SDS is one of the most commonly used chemical detergents for decellularization [66].
Although SDS is highly effective in lysing cells [34, 66], its major shortcoming is its ancillary toxicity due to been captured within the decellularized scaffold. We have identified a modified protocol using in addition to a combined chemical, enzymatic-physical protocol bovine serum albumin (BSA) to extract SDS out of the scaffold [72]. BSA is a protein with high water solubility because it contains many ionizable amino acids [73]. Kelley et al. reported that ionic surfactants may bind to BSA through a variety of different physicochemical mechanisms [74]. Nevertheless, in respect to a future clinical approach autologous human serum albumin instead of the bovine source has to be utilized to avoid immunogenicity (Table 2).
Another topic is the extraction of the residual DNA, which was released by the lysed cells and distributed within the scaffold. Apart from thorough washing steps, DNAse treatment has been recommended for this purpose to mediate DNA breakdown [75–78]. Furthermore, defatting of the ECM e.g. by using ethanol (70 %) could be useful to prepare improved cell reseeding [79].
In the end, an adequate and safe sterilization procedure should be selected, which is efficient, reproducible and does not change ECM structure and composition. For experimental approaches inactivation of potential pathogens was performed by 1 M NaOH [19] or 70 % ethanol [79]. Gamma radiation has also been applied for neutralization of pathogens [80].
During all steps of cell-free ECM preparation, no endotoxins should enter the scaffolds. Therefore, endotoxin-free buffers and water have to be used for all procedures and endotoxin content should be finally tested using adequate procedures [81]. Before reseeding, an adaption of the ECM scaffold in culture medium [21] or using fetal or human serum is advisable [72].
Kinds of Decellularized ECMs
Recent tissue-engineering studies have focussed on the application of several ECM-derived prosthetic materials in different variations as bioactive supports for cartilage repair (suppl. Table 1). Scaffolds derived from decellularized tissues have been demonstrated to facilitate in vitro adhesion, growth, migration, proliferation and function of several cell types [82–84]. The advantage of using native ECM is the conservation of natural ECM protein composition that is site-specific and provides the exact niche of the previous resident cells, which presents a chondroinductive microenvironment for the recolonizing cells [85]. Thereby, a decellularized ECM might exert chondroinductive effects [86, 87]. Due to the fact that many ECM proteins are highly conserved, the removal of xenogenic or allogenic cellular contents via decellularization could theoretically produce a minimally immunogenic scaffold which is in most cases more abundantly available than autografts [88].
Sutherland et al. distinguished four kinds of decellularized cartilage ECM scaffolds: (1) devitalized native cartilage, (2) decellularized native cartilage, which can be produced from the native cartilage tissue, (3) devitalized cell-derived ECM and (4) decellularized cell-derived ECM which is harvested in vitro from cultured chondrocytes or MSCs [89–92] (see also graphical abstract) or other cell types such as fibroblasts [93]. In addition, synovial membrane derived stem cells have been used for cell-derived ECM production [44]. ECM expression of MSCs can be stimulated by ascorbic acid to produce cell sheets that might be feasable to undergo decellularization in future [94]. Lu et al. reported a method to prepare an autologous cell-derived ECM scaffolds by co-culturing autologous MSCs and human articular chondrocytes in a 3D template. Subsequently, the constructs were decellularized and the template was removed before the ECM was implanted into mice in vivo. The research group demonstrated an excellent biocompatibility for the self-prepared ECM scaffolds [70]. In the end, an ECM scaffold derived from cultured cells might lack sufficient biomechanical strength, due to the less stable organization of ECM components and the overall composition might substantially differ from the native tissue due to dedifferentiation of cultured cells such as chondrocytes. Nevertheless, the ECM can be stabilized by cross-linking e.g. by UV or chemical exposition [91, 95]. Cell-free ECMs have also been integrated into composite scaffolds by combination with various natural and synthetic polymer scaffolds to improve their properties e.g. biomechanics [96, 97].
The decellularized native or cell-derived ECM can be further processed to get more flexible scaffolds e.g. by crushing and freeze dry techniques [42] including thermally induced phase separation (TIPS) [98] or by preparing a hydrogel for meniscus or nucleus pulposus substitution [99, 100]. Some authors proved the chondroinductive effect of so-called decellularized cartilage ECM-derived particles by using them as carriers to induce chondrogenesis of MSCs. The researchers produced the particles (with a size of 263 ± 48 μm) from fresh cartilage through a series of procedures (shattering, decellularization, lyophilization, pulverization) [86, 87]. Generating a temperature gradient in freezing can allow the creation of aligned pores in a decellularized cartilage-ECM-derived scaffold [95].
It is worth noting here that decellularization can be distinguished from devitalization of tissue resident cells – the last one implies that the tissue still contains the killed cells and their DNA, which could expose their antigenes. Additionally, the natural holes in the cartilage ECM, called lacunae, are still occupied by death cells or cell debris and hence, not available for recolonization. Furthermore, catabolic mediators released by dying cells might be captured within the ECM.
Most natural ECM scaffolds used are derived from mature tissue [101, 102]. ECM harvested from immature tissues could provide additional inductive stimuli through the presence of various growth factors [61, 86]. Supporting this conclusion, decellularized renal tissues revealed that immature tissue derived scaffolds and cells could allow a higher rate of cell repopulation [103].
An imperative question that still remains is how do you recellularize a scaffold before implantation. Both approaches using directly cell-free ECM scaffolds [32] or recellularized scaffolds [68] were described. Several studies in other tissues, but also cartilage, suggested that a recellularized ECM scaffold led to superior results compared with a cell-free construct [104–106].
Arguments for Using Stem Cells for Recellularization and Properties of MSCs
In most implantation sites, particularly in the joint cartilage, there are not enough resident cells available to immigrate into the cell-free scaffold to colonize it homogeneously. In cartilage, the resident cells were immobilized by their surrounding ECM. Furthermore, it is significantly challenging to harvest enough autologous cells e.g. from IVD or meniscus for expanding and seeding them in vitro onto the scaffold. In addition, donor site morbidity e.g., in the case of harvesting cells from the IVD presents limitations. In contrast, recellularization techniques require a high number of cells and hence, sufficient cell expansion. To circumvent all these restrictions MSCs attract attention. MSCs are a well-studied adult stem cell line, which are multipotent and characterized by a high proliferative activity, whereby the number of population doublings depends on age [107–109]. Hence, this survey will focus exclusively on this stem cell type. Meanwhile, BMSCs and ADMSCs have been seeded in a variety of 3D culture systems in an effort to generate cartilage-like tissue, including natural biopolymers such as collagen [110], silk fibroin and chitosan [111], hydrogels such as alginate, gelatin, agarose [13, 112, 113] and hyaluronan [114], and hybrids of synthetic and natural materials [115, 116]. Cartilage-like tissue formation can be induced using BMSCs or ADMSCs as evidenced by type II collagen, aggrecan expression and accumulation of both cartilage markers in vitro and in vivo [13]. Moreover, it has been observed that chondrogenic differentiation and ECM deposition is superior in BMSCs compared to expanded and dedifferentiated chondrocytes [117]. The addition of growth factors such as TGF-β1 or TGF-β3 facilitates the expression of cartilaginous ECM and chondrogenesis, mediated by the transcription factor Sox9 [118]. Chondroprogenitors residing in adults are primed to undergo chondrogenic differentiation in response to signals provided by TGF-β, FGFs and Wnts superfamily members. It is known that both Smad3 and Wnt-associated β-catenin signaling mediates chondrogenic differentiation of BMSCs in vitro through signals exerted by TGF-β1 [119, 120].
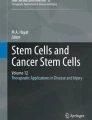
BMSCs have a high proliferative activity, plasticity and release many trophic and bioactive factors [121] (Fig. 1). In addition, they synthesize stimulatory ECM components – which are critical for the use of in vitro produced MSC-derived cell-free ECM [122], mediating the capacity to differentiate into connective tissue cells (e.g. in the chondrogenic, osteogenic, adipogenic and tenogenic lineage) [123–125]. Furthermore, they possess highly migratory properties, which allow a so-called “homing” as targeted migration to the place of origin or of injury and subsequent engraftment – thereby being attracted by chemokines [126]. Expression of chemokine receptors such as CCR1, CCR7, CCR9, CXCR4, CXCR5 and CXCR6 has been reported for BMSCs in passage 2 mediating their capability for homing. Additionally, pro-inflammatory cytokines such as TNFα and IL-1β act in a chemotactic manner on MSCs [127]. Inflammatory cytokines are usually released in injured tissues including cartilage and osteoarthritis. Activation of MSCs can be observed under these conditions. However, it is not sufficient under physiological conditions to restore cartilage integrity (Fig. 2). Unfortunately, in vitro expanded MSCs lose their capacity to express these chemokine receptors and hence, to migrate. Concomitantly, the expression of cell adhesion molecules such as ICAM-1, −2, VCAM-1 and CD157 is substantially decreased [128]. The high migratory potency of MSCs might facilitate recellularization in contrast to less migratory cell types.

Simplified scheme summarizing the mechanisms by which MSCs could influence cartilage repair. Mesenchymal stromal cells (MSC) are physiologically localized in a niche (a), once activated by various stimuli, they start division either in a symmetric manner for self-renewal (b) or in an asymmetric (c) manner. This diverse division capacity is typical for stem cells: (a) symmetric division means that two similar daughter cells arise both remaining in the stem cell niche and maintaining their full stem cell character. (b) The asymmetric produces two different daughter cells, one of them remains as a stem cell in the niche and the other cell leaves the niche and undergoes commitment. It can migrate (d) e.g. attracted by chemokines in response to tissue injury. Mesenchymal stromal cells can release trophic factors (c, d). Triggered by the presence of specific factors they differentiate into various directions (e) such as chondrocytes, osteocytes, adipocytes, fibroblasts, tenocytes, myocytes. If the microenvironment changes a dedifferentiation (f), transdifferentiation (g) or terminal differentiation such as hypertrophy (h) is possible

MSC activation in cartilage disorders such as cartilage injury and osteoarthritis. a An untreated full- thickness chondral defect in the knee joint of a minipig (medial femoral condyle) is depicted: only few repair tissue became evident six months after cartilage injury, but the subchondral bone marrow shows activated MSCs undergoing chondrogenesis (Hematoxylin-Eosin [HE] staining, arrows). b A severe state of human hip osteoarthritis is shown (a femoral head cartilage-bone segment was stained with HE): a fibrous repair tissue covers the subchondral bone completely devoid of articular cartilage. The bone marrow cavity beneath the subchondral bone reflects bone marrow activation containing cells undergoing fibrous tissue production (arrow). c: Knee joint cartilage (tibia plateau) derived from a rat osteoarthritis model (8 weeks post-induction) is depicted (alcian blue staining to visualize sGAGs): A segment of joint cartilage is focally broken through the subchondral bone plate forming a cyst. Also, an activation and chondrogenesis of MSCs appeared in the neighboring bone marrow cavity (arrow)
Additionally, MSCs are immunosuppressive, immunoprivileged, due to the lack of expression of co-stimulatory molecules, and possess immunomodulatory properties [129–133]. Low immunogenicity of stem cells is caused by low or nearly no major histocompatibility complex (MHC) II and costimulatory cell-surface protein expression [134]. This opens the perspective of allogeneic MSC transplantation [135, 136]. Inductors of the immunomodulatory effects are IFNγ and IL-1β [137, 138], whereas TNFα reduced their immunomodulatory capability [139, 140].
Protective humoral factors released from MSCs may stimulate cell survival, angiogenesis and reduce apoptosis and T cell response in certain diseases such as brain injury [141, 142]. Such regulatory factors are IL-1, IL-8, TNFα, leukemia inhibitory factor (LIF), granulocyte macrophage colony-stimulating factor (GM-CSF), thrombopoietin, macrophage inflammatory proteins (MIP1α) and FGF [143]. Furthermore, the secretion of a couple of other immunomodulatory factors such as IL-10, IL-6, hepatocyte growth factor (HGF), TGF-β, prostaglandin (PG)E2, indolamine-2,3-dioxygenase and nitric oxide (NO) has been reported [144, 145]. PGE2 induces the development of regulatory T cells (Treg) and activates B cells. MSCs can also induce the proliferation of pre-existing Tregs [146, 147]. They inhibit the maturation of antigen presenting cells (APCs) such as dendritic cells. MSC-derived NO, produced by inducible nitric oxide synthetase (iNOS), might inhibit T cell proliferation. The induction of cell cycle inhibitors in immune cells impairs their proliferation [143, 148]. The directed migratory activity is responsible for efficient engraftment in damaged tissue and homing of these cells to specific sites (Fig. 1). The indolamine-2,3-dioxygenase removes tryptophan from the local micromilieu – this amino acid is essential for lymphocyte proliferation [149]. Both immunomodulatory capacity and low immunogenicity are highly advantageous regarding MSCs as a cell source for reseeding decellularized scaffolds. MSCs cultured on the decellularized ECM scaffolds could enhance the biocompatibility of the constructs. In addition, the localized, sustained growth factor release of MSCs should encourage cell proliferation, differentiation and ECM production in the scaffolds. The native cartilage ECM might still contain factors and structural stimuli inducing them into a specific and appropriate chondrogenic lineage [87, 150]. Furthermore, they can be harvested, enriched and seeded directly on the implanted ECM in a one-step surgical procedure [24, 25]. Nevertheless, one has to keep in mind that MSCs also attain some disadvantages in that they can lose their differentiated phenotype when the microenvironment changes or undergo hypertrophy or other lineage differentiation (Fig. 2) [62]. Furthermore, the differentiation potential and the proliferative capacity of human ADMSCs and murine BMSCs depend on the donor age [108, 109]. Passaging of MSCs had the same effect in murine BMSCs [108]. Chondrogenic and osteogenic differentiative capability decreased in human ADMSCs whereas its senescence was increased [109]. The effect on adipogenesis differed [108, 109].
Further limitations of MSCs are their low number in the bone marrow, a weak or variable chondrogenic potential, not sufficient for repair (Fig. 2), subsequent vascularization, and mineralization of MSC-derived neo-tissues [62, 151]. Therefore, it is unclear whether stem cells are superior to chondrocytes in colonizing the ECM and forming the neocartilage-tissue. In another study chondrogenically induced MSC cultured on a cell-free IVD ECM revealed a higher GAG and collagen content than IVD cells, but a lower DNA content suggesting lower cell numbers [72]. Therefore, several open questions have still to be answered e.g. how to stabilize MSC driven chondrogenesis. Hence, it has to be considered which MSC source is the best for reseeding decellularized cartilage ECM scaffolds regarding chondrogenesis and accessibility. Stem cell populations such as bone marrow derived BMSCs, or stem cells derived from the adipose tissue (ADMSCs), infrapatellar fat pad (FPSCs) or synovium have been proposed. ADMSCs are easily and abundantly accessible. Adipose tissue contains a higher number of progenitor cells with higher proliferative capacity and viability [152]. Synovium-derived MSCs and FPSCs, which are naturally adapted to the joint milieu, present other promising sources for chondrogenesis [23, 150, 153–156]. Probably, the selection of the appropriate cell or stem cell type depends on the particular cartilage ECM selected for recellularization, accessibility, donor site morbidity and the future site of implantation.
Conditions Supporting MSC Chondrogenesis and Favoring them as Candidates to Colonize Decellularized Scaffolds
Co-Cultures
Co-cultures consisting of articular chondrocytes and MSCs have been developed to moderate the risk of hypertrophy and calcification associated with MSCs and to overcome the limited availability of chondrocytes. Interactions between both cell types can maintain their chondrogenic phenotype, resulting in enhanced chondrogenesis and cartilage-like ECM generation (Fig. 2), while reducing the number of chondrocytes needed for the start of culturing [151, 157, 158]. Meretoja et al. demonstrated that the majority of primary bovine chondrocytes could be replaced by MSCs in a co-culture setting without inhibitory effects on their in vitro chondrogenesis. The more detailed examination showed that similar DNA and GAG contents could be observed in chondrocytes-MSCs co-cultures in comparison to constructs with primary chondrocytes alone. Therefore, they concluded that the trophic effect of MSCs might recover and augment the chondrogenic potential of chondrocytes [157]. Another previous study has shown that chondrocytes cultured on a scaffold under flow perfusion were capable of synthesizing cartilage-like ECM within the scaffold that is effective in inducing the chondrogenesis of MSCs [21]. Levorson et al. developed an electrospun PCL scaffolds coated with a devitalized cartilage-like ECM, which was produced by co-culturing of chondrocytes and MSCs. They found that a 1:1 ratio of chondrocytes co-cultured for 14 days with MSCs led to a similar expression pattern of chondrogenic genes (collagen type II/I ratio and aggrecan) like MSCs cultured for 21 days alone but with TGF-β3 supplementation on scaffolds [159]. Tsai et al. co-cultured human IVD cells and human bone marrow-derived MSCs in an ECM structure-mimetic scaffold (consisting of nanofibers of synthetic polymers), which was stimulated by cyclic compression in a perfusion bioreactor. The research group found, that MSC-derived osteogenic cells residing in the interface layer turned into chondrogenic cells, with decreased expression of osteogenic markers and increased expression of chondrogenic markers [160]. The dynamic environment produced by a flow perfusion bioreactor resulted in superior neocartilage formation by MSCs cultured in a composite scaffold consisting of PCL and a decellularized cartilage ECM compared with static conditions [21].
Hypoxia
By reason of avoiding complications such as low chondrogenic or aberrant differentiation of MSCs, recent researches have studied the chondrogenesis of MSCs by mimicking the physiological conditions within cartilage tissue concerning impaired compared to ambient oxygen tensions. Due to increased Oct4 expression and telomerase activity, both adipogenic and osteogenic differentiation capacity of human BMSCs cultured in hypoxia was decreased [161–163]. Based on the findings that oxygen tension in the joint varies between approximately 7 % (cartilage surface) to as low as 1 % (subchondral bone), this range of low oxygen tension plays a key role in cartilage and bone development involving activated AKT signaling and hypoxia inducible factor (HIF) transcription factors [164, 165]. HIF-1 and HIF-2 are transcription factors of the HIF family, both of them regulate the cell response to hypoxia; HIF-1α is more ubiquitous whereas HIF-2α is more cell-specific [166]. Accordingly, Adesida et al. reported that hypoxic conditions enhanced the expression of HIF-2α by BMSCs and hypoxia-expanded BMSCs displaying a more robust chondrogenesis than normoxia-expanded BMSCs by increasing sGAG deposition and expression of cartilage matrix components aggrecan, type II collagen and the chondrogenic transcription factor Sox9 [167]. Similarly, BMSCs differentiated into chondrogenic cells in alginate beads exposed to the hypoxic environment. This study provided evidence that HIF-1α is essential for hypoxic induction of chondrogenesis. Moreover, additional in vivo analysis indicated that hypoxic conditions or HIF-1α overexpression are efficient and sufficient to induce the chondrocytic phenotype in BMSCs without utilization of growth factors [168]. A recent study explored the chondrogenesis and hypertrophy in co-cultures of bovine articular chondrocytes and BMSCs under reduced oxygen tension (5 % O2 versus 20 %). After two weeks of culture, hypoxia promoted a higher chondrogenesis by MSCs than normoxic culture condition. The risk of hypertrophy depicted by type X collagen expression was lower in co-cultures than in pure MSC cultures but higher under hypoxia [169].
On the other hand, the effects of hypoxia on ADMSCs were also well proved. The chondrogenic potential of ADMSCs was enhanced under hypoxic compared with normoxic conditions evidenced by decreased ADMSCs proliferation and increased chondrocytic marker expression [170]. This data supports the role of low oxygen tension as beneficial influence factor on the chondrogenic differentiation of ADMSCs and BMSCs.
In disease models, hypoxic sites release cytokines, chemokines and other mediators such as HIF-1 and stromal cell-derived factor-1 (SDF-1), which recruit MSCs to sites of injury, ischemia, and hypoxia from which subsequent tissue repair benefits [171, 172].
Pitfalls in Decellularization Protocols
An obstacle in using decellularized ECMs includes the incomplete removal of immunogenic cell remnants [14]. Furthermore, it is important to achieve interconnectivity in a tissue with no preexisting interconnecting pores, such as cartilage and adjusted appropriate cellularity, restore natural cell distribution and finally an adequate seeding strategy [156]. To achieve interconnectivity in decellularized cartilage, channels have been introduced into the tissue in a recent study, which improved subsequent cell colonization [155]. To reseed the tissue under perfusion pressure can facilitate a homogenous cell distribution [173].
Cells with maintained differentiation potential should be selected for seeding the ECM. Partington et al. reported a decline in soluble collagen in decellularized tissue, as well as the substantial reduction in GAG content, both of which might contribute to loss of mechanical integrity of biotracheas. For this reason, they suggested, that the decline of the decellularization time could result in better retention of GAGs [174] and probably allow cells to produce novel GAGs.
A major stumbling block with bioengineered organs is the provision of a functional blood supply. Unlike other transplants, cartilage or IVD replacement is rarely a life-saving procedure, and due to their physiological avascular and aneural conditions, this issue is less demanding. Restoring the access to blood vessels increases the risk of allograft rejection. However, blood supply is required if a whole organ containing cartilage such as the trachea is replaced.
Decellularized tissue could attract immunologically active cells and these cells could mediate an acute allograft rejection, which requires high-dose immunosuppression as shown for tracheal reconstruction [175].
Remnants of various chemical reagents used in this decellularization process could damage the colonizing cells. Therefore, decellularized scaffolds with high concentrations of residual chemicals like detergents are toxic to cells (Table 1 ). Consequently, it is essential to determine the cell compatibility of the ECM before it is used for recellularization, as well as eliminating the toxic decellularization buffer components [60].
Density of ECM in cartilage remains highly challenging for both de- and recellularization procedures, especially the calcified cartilage layer in joint cartilage. Decellularization has to be combined with decalcification to achieve cell removal in these tissue layers. The biomechanical resilience of this tissue can be impaired in response to decellularization [176]. Nevertheless, these biomechanical differences between native and decellularized tissues were often not significant [177]. Shortening of the time-consuming protocol, which often requires around one week of tissue processing with the risk of contamination and washing out of essential components would also be an issue in the future.
The cell size of recipients and pore sizes in the decellularized xenogeneic ECM should match which is the case in using bovine cartilage for rhino surgery [39].
It is also necessary to figure out adequate sterilization procedures, which do not change ECM properties or lead to remaining toxicity.
First Insights in Vivo Using Cartilage ECM
The biocompatibility between biomaterial and the immune system can only be detected in vivo. The systemic immune response could affect graft integration. Decellularized bone has been used clinically for decades for successful reconstruction of bone defects [178]. Decellularized cartilage ECM scaffolds also supported enchondral bone formation in a mouse model [62]. Yang et al. cultured chondrogenically induced BMSCs labeled with the fluorescent dye PKH26 on a natural, acellular, interconnected porous scaffold prepared from cartilage and implanted this subcutaneously into nude mice for four weeks. Following this they identified cartilage-like tissue formation, with positive staining for type II collagen, Safranin O and toluidine blue indicating GAG deposition [67]. In another study, a rat decellularized trachea scaffold was implanted subcutaneously in nude mice. After 12 months a whole recellularization could be observed in vivo [179]. Kang et al. cultured ADSCs on a decellularized articular cartilage ECM in a bioreactor dynamically and statically. Then they implanted the cartilage ECM construct into nude mice. Examination after three weeks showed that cell distribution in the dynamic group was more uniform than in the static group, and ECM as well as type II collagen deposition was stronger [63]. Cell-free cartilage ECM-derived particles seeded with BMSCs were implanted in the rat knee joint and supported cartilage repair [87] A cartilage ECM-derived scaffold optimized by the thermal-induced phase separation (TIPS) technique was seeded with BMSCs. Tested in the rabbit model, it led to the repair of full-thickness articular cartilage defects in the knee joint [98]. In another study osteochondral defect repair was tested in the femur condyles of dogs. The defects filled with biphasic decellularized cartilage ECM scaffolds seeded with BMSCs revealed superior results compared with the controls [71].
There exist so far no published studies describing the chondrogenesis of MSCs on decellularized nasoseptal cartilage ECM, but decellularized nasoseptal cartilage was successfully recolonized with nasoseptal chondrocytes and then implanted in a rat model for reconstruction of the nasal septum [180].
A couple of studies reported the fate of hyaline tracheal cartilage scaffolds in vivo in different animal models. In a rabbit model a decellularized graft trachea from a donor animal was implanted. Before implantation, MSCs isolated from recipient rabbit adipose tissue were cultured and marked with PKH26 before being seeded in the decellularized tracheal ECM. Histopathological analysis revealed the integration of MSCs seeded-decellularized cadaveric tracheas to the recipient tracheal sides and increased angiogenesis. After 30–90 days, the MSCs were detected by fluorescence microscopy in the ciliated epithelium, in the submucosal layer, and in the cartilage of the integrated new trachea suggesting cell survival and migration [181]. Grevemeyer et al. successfully substituted horse laryngeal cartilage by decellularized ECM performing a feasibility study [32]. In a large animal model (pig) long-segment circumferential tracheal allografts were decellularized using two different protocols and recellularized using recipient MSCs and tracheal epithelial progenitor cells before implanted heterotopically under a muscle flap in the neck of the beneficiaries. Recellularization impaired immune cell infiltration up to three weeks post-transplantation and allowed cartilage preservation [106]. There exists already an encouraging case report were the transferability of the results in humans could be proved: Macchiarini et al. removed cells and MHC antigens from a human donor trachea, which was then readily colonized by autologous epithelial cells and chondrogenically differentiated MSCs. Then they used it for replacing the recipient’s left main bronchus. Their findings demonstrated that autologous MSCs combined with a decellularized ECM probably provide successful treatment for patients with severe clinical disorders in future [182, 183].
There exist some in vivo studies describing fibrocartilage repair by using a decellularized ECM: Decellularized fibrocartilage ECM has already been tested in an IVD degeneration rabbit model in vivo [43]. In another study, the fibrocartilaginous meniscus ECM was tested in a rat model revealing a high biocompatibility [52].
Conclusion
Decellularization of various tissues for biomimetic scaffold preparation has become an emerging and expanding field in tissue engineering. Some approaches have already entered the clinical phase such as decellularized bone, heart valves ligaments, etc. [59]. Decellularizing cartilage presents some difficulties. Due to their easy availability, low donor site morbidity, differentiative flexibility, immunomodulatory capacities, low antigenicity and trophic effects MSCs can be considered as promising candidates for reseeding decellularized cartilage.
Some future perspectives could be proposed from the current literature: Firstly, it would be advantageous to functionalize scaffolds with chemotactic compounds for an increase in cell recruitment and to increase penetration of the scaffold by cells to achieve homogeneous cell distribution.
Furthermore, co-cultures with MSCs and differentiated cell populations could be performed to increase and stabilize their chondrogenic differentiation.
Additionally, bioreactor culture, adequate mechanostimulation protocols and low oxygen conditions could be developed for seeded ECM constructs to promote differentiation, cell distribution and cell activity.
ADMSCs, adipose tissue-derived stem cells; AF, annulus fibrosus cells; APC, antigen presenting cells; BMP, bone morphogenetic proteins; BMSC, bone-marrow derived mesenchymal stromal cells, Dkk-1, dickkopf-1; ECM, extracellular cartilage matrix; EGF, epithelial growth factor; FGF, fibroblast growth factor; GM-CSF, granulocyte macrophage colony-stimulating factor; HB-EGF, heparin-binding EGF-like growth protein; HE, hematoxylin-eosin; HGF, hepatocyte growth factor; HIF, hypoxia inducible factor; HMBG, high-mobility group box 1 protein; ICAM, intercellular adhesion molecule; IGF, insulin-like growth factor; IL, interleukin; IVD, intervertebral disc; LIF, leukemia inhibitory factor; MHC, major histocompatibility complex; MIP1alpha, macrophage inflammatory protein; MSC, mesenchymal stromal cells; NO, nitric oxide; NOS, nitric oxide synthase; NP, nucleus pulposus cells; PDGF, platelet derived growth factor; PG, proteoglycans; sGAG, sulfated glycosaminoglycans; SOX9, SRY (sex-determining region Y)-box 9 protein; TGF, transforming growth factor; TIPS, thermally induced phase separation; VCAM, vascular cell adhesion molecule; VEGF, vascular endothelial growth factor.
References
Steinert, A. F., Ghivizzani, S. C., Rethwilm, A., et al. (2007). Major biological obstacles for persistent cell-based regeneration of articular cartilage. Arthritis Research & Therapy, 9(3), 213.
Asik, M., Ciftci, F., Sen, C., et al. (2008). The microfracture technique for the treatment of full-thickness articular cartilage lesions of the knee: midterm results. Arthroscopy, 24(11), 1214–1220.
Bekkers, J. E., Inklaar, M., & Saris, D. B. (2009). Treatment selection in articular cartilage lesions of the knee: a systematic review. American Journal Sports Medicine, 37(Suppl 1), 148S–155S.
Bugbee, W.D. and F.R. Convery, Osteochondral allograft transplantation (1999). Clin Sports Medicine, 18(1), 67–75.
Chu, C. R., Convery, F. R., Akeson, W. H., et al. (1999). Articular cartilage transplantation. Clinical results in the knee. Clinical Orthopaedics and Related Research, 360, 159–168.
Brittberg, M., Lindahl, A., Nilsson, A., et al. (1994). Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. New England Journal of Medicine, 331(14), 889–895.
Logerstedt, D. S., Snyder-Mackler, L., Ritter, R. C., et al. (2010). Knee pain and mobility impairments: meniscal and articular cartilage lesions. The Journal of Orthopaedic and Sports Physical Therapy, 40(6), A1–A35.
Mandelbaum, B. R., Browne, J. E., Fu, F., et al. (1998). Articular cartilage lesions of the knee. American Journal of Sports Medicine, 26(6), 853–861.
Loeser, R. F. (2008). Molecular mechanisms of cartilage destruction in osteoarthritis. Journal of Musculoskeletal & Neuronal Interactions, 8(4), 303–306.
Pattappa, G., M. Peroglio, D. Sakai, et al., CCL5/RANTES is a key chemoattractant released by degenerative intervertebral discs in organ culture (2014). European Cells & Materials, 27, 124–136; discussion 136.
Safran, M. R., Kim, H., Zaffagnini, S., & The use of scaffolds in the management of articular cartilage injury (2008). The Journal of the American Academy of Orthopaedic Surgeons, 16(6), 306–311.
Wang, J., Yang, Q., Cheng, N., et al. (2016). Collagen/silk fibroin composite scaffold incorporated with PLGA microsphere for cartilage repair. Material Science & Enginering C Material Biological Applications, 61, 705–711.
Zimoch-Korzycka, A., Bobak, L., & Jarmoluk, A. (2016). Antimicrobial and antioxidant activity of chitosan/hydroxypropyl methylcellulose film-forming hydrosols hydrolyzed by cellulase. International Journal of Molecular Sciences, 17, 9.
Wong, M. L., & Griffiths, L. G. (2014). Immunogenicity in xenogeneic scaffold generation: antigen removal vs. decellularization. Acta Biomaterialia, 10(5), 1806–1816.
Mandal, B. B., & Kundu, S. C. (2009). Cell proliferation and migration in silk fibroin 3D scaffolds. Biomaterials, 30(15), 2956–2965.
Ko, C. S., Huang, J. P., Huang, C. W., & Chu, I. M. (2009). Type II collagen-chondroitin sulfate-hyaluronan scaffold cross-linked by genipin for cartilage tissue engineering. Journal of Bioscience and Bioengineering, 107(2), 177–182.
Tuan, R. S., Chen, A. F., & Klatt, B. A. (2013). Cartilage regeneration. The Journal of the American Academy of Orthopaedic Surgeons, 21(5), 303–311.
Lohan, A., Marzahn, U., El Sayed, K., et al. (2011). In vitro and in vivo neo-cartilage formation by heterotopic chondrocytes seeded on PGA scaffolds. Histochemistry and Cell Biology, 136(1), 57–69.
Schwarz, S., Koerber, L., Elsaesser, A. F., et al. (2012). Decellularized cartilage matrix as a novel biomatrix for cartilage tissue-engineering applications. Tissue Engineering Part A, 18(21–22), 2195–2209.
Cissell, D. D., Hu, J. C., Griffiths, L. G., & Athanasiou, K. A. (2014). Antigen removal for the production of biomechanically functional, xenogeneic tissue grafts. Journal of Biomechanics, 47(9), 1987–1996.
Liao, J., Guo, X., Grande-Allen, K. J., et al. (2010). Bioactive polymer/extracellular matrix scaffolds fabricated with a flow perfusion bioreactor for cartilage tissue engineering. Biomaterials, 31(34), 8911–8920.
Haleem, A. M., Singergy, A. A., Sabry, D., et al. (2010). The clinical use of human culture-expanded autologous bone marrow mesenchymal stem cells transplanted on platelet-rich fibrin glue in the treatment of articular cartilage defects: a pilot study and preliminary results. Cartilage, 1(4), 253–261.
Fan, J., Varshney, R. R., Ren, L., et al. (2009). Synovium-derived mesenchymal stem cells: a new cell source for musculoskeletal regeneration. Tissue Engineering. Part B, Reviews, 15(1), 75–86.
Steinwachs, M. R., Waibl, B., & Niemeyer, P. (2011). Use of human progenitor cells in the treatment of cartilage damage. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 54(7), 797–802.
Steinwachs, M. R., Waibl, B., Wopperer, S., & Mumme, M. (2014). Matrix-associated chondroplasty: A novel platelet-rich plasma and concentrated nucleated bone marrow cell-enhanced cartilage restoration technique. Arthroscopy Techniques, 3(2), e279–e282.
Hunziker, E. B., Quinn, T. M., & Hauselmann, H. J. (2002). Quantitative structural organization of normal adult human articular cartilage. Osteoarthritis Cartilage, 10(7), 564–572.
Cole, A. G. (2011). A review of diversity in the evolution and development of cartilage: the search for the origin of the chondrocyte. European Cells & Materials, 21, 122–129.
Han, L., Grodzinsky, A. J., & Ortiz, C. (2011). Nanomechanics of the cartilage extracellular matrix. Annual Review Material Research, 41, 133–168.
Chung, C., & Burdick, J. A. (2008). Engineering cartilage tissue. Advance Drug Delivery Review, 60(2), 243–262.
Yang, Q., Peng, J., Lu, S. B., et al. (2011). In vitro cartilage tissue engineering with cartilage extracellular matrix-derived porous scaffolds and bone marrow mesenchymal stem cells. Zhonghua Yi Xue Za Zhi, 91(17), 1161–1166.
Kojima, K., & Vacanti, C. A. (2014). Tissue engineering in the trachea. Anatomical Record (Hoboken), 297(1), 44–50.
Grevemeyer, B., L. Bogdanovic, S. Canton, et al., Regenerative medicine approach to reconstruction of the equine upper airway (2014). Tissue Engineering Part A, 20(7–8), 1213–1221.
Ma, A., Jiang, L., Song, L., et al. (2013). Reconstruction of cartilage with clonal mesenchymal stem cell-acellular dermal matrix in cartilage defect model in nonhuman primates. Internatinal Immunopharmacology, 16(3), 399–408.
Elder, B. D., Kim, D. H., & Athanasiou, K. A. (2010). Developing an articular cartilage decellularization process toward facet joint cartilage replacement. Neurosurgery, 66(4), 722–727 discussion 727.
Colnot, C., Zhang, X., & Knothe Tate, M. L. (2012). Current insights on the regenerative potential of the periosteum: molecular, cellular, and endogenous engineering approaches. Journal of Orthopaedic Research, 30(12), 1869–1878.
Matzenauer, C., Reckert, A., & Ritz-Timme, S. (2013). Estimation of age at death based on aspartic acid racemization in elastic cartilage of the epiglottis. International Journal of Legal Medicine, 128(6), 995–1000.
Sterodimas, A., de Faria, J., Correa, W. E., & Pitanguy, I. (2009). Tissue engineering and auricular reconstruction: a review. Journal of Plastic, Reconstructive & Aesthetic Surgery, 62(4), 447–452.
Mizuno, M., Kobayashi, S., Takebe, T., et al. (2014). Brief report: Reconstruction of joint hyaline cartilage by autologous progenitor cells derived from ear elastic cartilage. Stem Cells, 32(3), 816–821.
Goldberg-Bockhorn, E., Schwarz, S., Elsasser, A., et al. (2014). Physical characterization of decellularized cartilage matrix for reconstructive rhinosurgery. Laryngorhinootologie, 93(11), 756–763.
Uppal, R. S., Sabbagh, W., Chana, J., & Gault, D. T. (2008). Donor-site morbidity after autologous costal cartilage harvest in ear reconstruction and approaches to reducing donor-site contour deformity. Plastic and Reconstructive Surgery, 121(6), 1949–1955.
Utomo, L., Pleumeekers, M. M., Nimeskern, L., et al. (2015). Preparation and characterization of a decellularized cartilage scaffold for ear cartilage reconstruction. Biomedical Materials, 10(1), 015010.
Xu, H., Xu, B., Yang, Q., et al. (2013). Fabrication and analysis of a novel tissue engineered composite biphasic scaffold for annulus fibrosus and nucleus pulposus. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, 27(4), 475–480.
Yuan, M., Yeung, C. W., Li, Y. Y., et al. ((2013). Effects of nucleus pulposus cell-derived acellular matrix on the differentiation of mesenchymal stem cells. Biomaterials, 34(16), 3948–3961.
Shoukry, M., Li, J., & Pei, M. (2013). Reconstruction of an in vitro niche for the transition from intervertebral disc development to nucleus pulposus regeneration. Stem Cells and Development, 22(8), 1162–1176.
Chan, L. K., Leung, V. Y., Tam, V., et al. (2013). Decellularized bovine intervertebral disc as a natural scaffold for xenogenic cell studies. Acta Biomaterialia, 9(2), 5262–5272.
Mercuri, J. J., Gill, S. S., & Simionescu, D. T. (2011). Novel tissue-derived biomimetic scaffold for regenerating the human nucleus pulposus. Journal of Biomedical Materials Research. Part A, 96(2), 422–435.
Wu, L. C., Chiang, C. J., Liu, Z. H., et al. (2014). Fabrication and properties of acellular porcine anulus fibrosus for tissue engineering in spine surgery. Journal of Orthopaedic Surgery and Research, 9, 118.
Pattappa, G., Z. Li, M. Peroglio, et al., Diversity of intervertebral disc cells: phenotype and function (2012). Journal of Anatomy, 221(6), 480–496.
Fisher, M. B., Henning, E. A., Soegaard, N., et al. (2013). Organized nanofibrous scaffolds that mimic the macroscopic and microscopic architecture of the knee meniscus. Acta Biomaterialia, 9(1), 4496–4504.
Stabile, K. J., Odom, D., Smith, T. L., et al. ((2010). An acellular, allograft-derived meniscus scaffold in an ovine model. Arthroscopy, 26(7), 936–948.
Jiang, D., Zhao, L. H., Tian, M., et al. (2012). Meniscus transplantation using treated xenogeneic meniscal tissue: viability and chondroprotection study in rabbits. Arthroscopy, 28(8), 1147–1159.
Chen, Y. C., Chen, R. N., Jhan, H. J., et al. (2015). Development and characterization of acellular extracellular matrix scaffolds from porcine menisci for use in cartilage tissue engineering. Tissue Engineering Part C Methods, 21(9), 971–986.
Stapleton, T. W., Ingram, J., Katta, J., et al. (2008). Development and characterization of an acellular porcine medial meniscus for use in tissue engineering. Tissue Engineering Part A, 14(4), 505–518.
Stapleton, T. W., Ingram, J., Fisher, J., & Ingham, E. (2011). Investigation of the regenerative capacity of an acellular porcine medial meniscus for tissue engineering applications. Tissue Engineering Part A, 17(1–2), 231–242.
Rothrauff, B. B., & Tuan, R. S. (2014). Cellular therapy in bone-tendon interface regeneration. Organogenesis, 10(1), 13–28.
Benjamin, M., & McGonagle, D. (2009). Entheses: Tendon and ligament attachment sites. Scandinavian Journal of Medicine & Science in Sports, 19(4), 520–527.
Beaulieu, M. L., Carey, G. E., Schlecht, S. H., et al. (2015). Quantitative comparison of the microscopic anatomy of the human ACL femoral and tibial entheses. Journal of Orthopaedic Research, 33(12), 1811–1817.
Cooper, J. O., Bumgardner, J. D., Cole, J. A., et al. (2014). Co-cultured tissue-specific scaffolds for tendon/bone interface engineering. Journal of Tissue Engineering, 5, 2041731414542294.
Rana, D., Zreiqat, H., Benkirane-Jessel, N., et al. (2015). Development of decellularized scaffolds for stem cell-driven tissue engineering. Journal of Tissue Engineering Regenerative Medicine. doi:10.1002/term.2061.
Gilbert, T. W., Sellaro, T. L., & Badylak, S. F. (2006). Decellularization of tissues and organs. Biomaterials, 27(19), 3675–3683.
Sutherland, A. J., Converse, G. L., Hopkins, R. A., Detamore, M. S., & The bioactivity of cartilage extracellular matrix in articular cartilage regeneration (2015). Advance Healthcare Materials, 4(1), 29–39.
Gawlitta, D., Benders, K. E., Visser, J., et al. (2015). Decellularized cartilage-derived matrix as substrate for endochondral bone regeneration. Tissue of Engineering Part A, 21(3–4), 694–703.
Kang, H., S. Lu, J. Peng, et al., In vivo construction of tissue-engineered cartilage using adipose-derived stem cells and bioreactor technology (2014). Cell and Tissue Banking. 16(1):123–133.
Bronstein, J. A., Woon, C. Y., Farnebo, S., et al. (2013). Physicochemical decellularization of composite flexor tendon-bone interface grafts. Plastic and Reconstructive Surgery, 132(1), 94–102.
Zang, M., Zhang, Q., Chang, E. I., et al. (2012). Decellularized tracheal matrix scaffold for tissue engineering. Plastic and Reconstructive Surgery, 130(3), 532–540.
Elder, B. D., Eleswarapu, S. V., & Athanasiou, K. A. (2009). Extraction techniques for the decellularization of tissue engineered articular cartilage constructs. Biomaterials, 30(22), 3749–3756.
Yang, Q., Peng, J., Guo, Q., et al. (2008). A cartilage ECM-derived 3-D porous acellular matrix scaffold for in vivo cartilage tissue engineering with PKH26-labeled chondrogenic bone marrow-derived mesenchymal stem cells. Biomaterials, 29(15), 2378–2387.
Zhao, Y. H., Yang, Q., Xia, Q., et al. (2013). In vitro cartilage production using an extracellular matrix-derived scaffold and bone marrow-derived mesenchymal stem cells. Chinese Medical Journal (Engl), 126(16), 3130–3137.
Kim, H. W., Knowles, J. C., & Kim, H. E. (2005). Hydroxyapatite and gelatin composite foams processed via novel freeze-drying and crosslinking for use as temporary hard tissue scaffolds. Journal of Biomedical Materials Research. Part A, 72(2), 136–145.
Lu, H., Hoshiba, T., Kawazoe, N., & Chen, G. (2011). Autologous extracellular matrix scaffolds for tissue engineering. Biomaterials, 32(10), 2489–2499.
Yang, Q., Peng, J., Lu, S. B., et al. (2011). Evaluation of an extracellular matrix-derived acellular biphasic scaffold/cell construct in the repair of a large articular high-load-bearing osteochondral defect in a canine model. Chinese Medical Journal (Engl), 124(23), 3930–3938.
Huang, Z., Kohl, B., Kokozidou, M., et al. (2016). Establishment of a Cytocompatible Cell-Free Intervertebral Disc Matrix for Chondrogenesis with Human Bone Marrow-Derived Mesenchymal Stromal Cells. Cells Tissues Organs, 201(5), 354–365.
Giancola, C., De Sena, C., Fessas, D., et al. (1997). DSC studies on bovine serum albumin denaturation. Effects of ionic strength and SDS concentration. International Journal of Biological Macromolecules, 20(3), 193–204.
Kelley, D., & McClements, D. J. (2003). Interactions of bovine serum albumin with ionic surfactants in aqueous solutions. Food Hydrocolloids, 17(1), 73–85.
Price, A. P., England, K. A., Matson, A. M., et al. (2010). Development of a decellularized lung bioreactor system for bioengineering the lung: the matrix reloaded. Tissue Engineering. Part A, 16(8), 2581–2591.
Kheir, E., Stapleton, T., Shaw, D., et al. (2011). Development and characterization of an acellular porcine cartilage bone matrix for use in tissue engineering. Journal of Biomedical Materials Research. Part A, 99(2), 283–294.
Youngstrom, D. W., Barrett, J. G., Jose, R. R., & Kaplan, D. L. (2013). Functional characterization of detergent-decellularized equine tendon extracellular matrix for tissue engineering applications. PLoS One, 8(5), e64151.
Mendoza-Novelo, B., Avila, E. E., Cauich-Rodriguez, J. V., et al. (2011). Decellularization of pericardial tissue and its impact on tensile viscoelasticity and glycosaminoglycan content. Acta Biomaterialia, 7(3), 1241–1248.
Lumpkins, S. B., Pierre, N., & McFetridge, P. S. (2008). A mechanical evaluation of three decellularization methods in the design of a xenogeneic scaffold for tissue engineering the temporomandibular joint disc. Acta Biomaterialia, 4(4), 808–816.
Ding, Y., Ruan, D., Luk, K. D., et al. (2014). The effect of gamma irradiation on the biological properties of intervertebral disc allografts: in vitro and in vivo studies in a beagle model. PLoS One, 9(6), e100304.
Gorbet, M. B., & Sefton, M. V. (2005). Endotoxin: the uninvited guest. Biomaterials, 26(34), 6811–6817.
Conconi, M. T., De Coppi, P., Di Liddo, R., et al. (2005). Tracheal matrices, obtained by a detergent-enzymatic method, support in vitro the adhesion of chondrocytes and tracheal epithelial cells. Transplant International, 18(6), 727–734.
Dettin, M., Conconi, M. T., Gambaretto, R., et al. (2005). Effect of synthetic peptides on osteoblast adhesion. Biomaterials, 26(22), 4507–4515.
Burra, P., Tomat, S., Conconi, M. T., et al. (2004). Acellular liver matrix improves the survival and functions of isolated rat hepatocytes cultured in vitro. International Journal of Molecular Medicine, 14(4), 511–515.
Song, J. J., & Ott, H. C. (2011). Organ engineering based on decellularized matrix scaffolds. Trends Molecular Medicine, 17(8), 424–432.
Sutherland, A. J., Beck, E. C., Dennis, S. C., et al. (2015). Decellularized cartilage may be a chondroinductive material for osteochondral tissue engineering. PLoS One, 10(5), e0121966.
Yin, H., Wang, Y., Sun, Z., et al. (2016). Induction of mesenchymal stem cell chondrogenic differentiation and functional cartilage microtissue formation for in vivo cartilage regeneration by cartilage extracellular matrix-derived particles. Acta Biomaterialia, 33, 96–109.
Hutter, H., Vogel, B. E., Plenefisch, J. D., et al. (2000). Conservation and novelty in the evolution of cell adhesion and extracellular matrix genes. Science, 287(5455), 989–994.
Sutherland, A. J., Converse, G. L., Hopkins, R. A., & Detamore, M. S. (2014). The bioactivity of cartilage extracellular matrix in articular cartilage regeneration. Advance Healthcare Materials, 4(1), 29-39. doi:10.1002/adhm.201400165.
Hoshiba, T., Lu, H., Kawazoe, N., et al. (2013). Effects of extracellular matrix proteins in chondrocyte-derived matrices on chondrocyte functions. Biotechnology Progress, 29(5), 1331–1336.
Xu, Y., Xu, G. Y., Tang, C., et al. (2015). Preparation and characterization of bone marrow mesenchymal stem cell-derived extracellular matrix scaffolds. Journal of Biomedical Materials Research. Part B, Applied Biomaterials, 103(3), 670–678.
Pei, M., Li, J. T., Shoukry, M., & Zhang, Y. (2011). A review of decellularized stem cell matrix: a novel cell expansion system for cartilage tissue engineering. European Cell & Materials, 22, 333–343 discussion 343.
Zhou, Y., Zimber, M., Yuan, H., et al. (2016). Effects of human fibroblast-derived extracellular matrix on mesenchymal stem cells. Stem Cell Reviews., 12(5), 560–572.
Wei, F., Qu, C., Song, T., et al. (2012). Vitamin C treatment promotes mesenchymal stem cell sheet formation and tissue regeneration by elevating telomerase activity. Journal of Cellular Physiology, 227(9), 3216–3224.
Rowland, C. R., Colucci, L. A., & Guilak, F. (2016). Fabrication of anatomically-shaped cartilage constructs using decellularized cartilage-derived matrix scaffolds. Biomaterials, 91, 57–72.
Sadr, N., Pippenger, B. E., Scherberich, A., et al. (2012). Enhancing the biological performance of synthetic polymeric materials by decoration with engineered, decellularized extracellular matrix. Biomaterials, 33(20), 5085–5093.
Johnson, C., Sheshadri, P., Ketchum, J. M., et al. (2016). In vitro characterization of design and compressive properties of 3D–biofabricated/decellularized hybrid grafts for tracheal tissue engineering. Journal of the Mechanical Behavior Biomedical Materials, 59, 572–585.
Jia, S., T. Zhang, Z. Xiong, et al., In vivo evaluation of a novel oriented scaffold-bmsc construct for enhancing full-thickness articular cartilage repair in a rabbit model (2015). PLoS One, 10(12), e0145667.
Mercuri, J. J., Patnaik, S., Dion, G., et al. (2013). Regenerative potential of decellularized porcine nucleus pulposus hydrogel scaffolds: stem cell differentiation, matrix remodeling, and biocompatibility studies. Tissue Engineering. Part A, 19(7–8), 952–966.
Wu, J., Ding, Q., Dutta, A., et al. (2015). An injectable extracellular matrix derived hydrogel for meniscus repair and regeneration. Acta Biomaterialia, 16, 49–59.
Agrawal, V., Brown, B. N., Beattie, A. J., et al. (2009). Evidence of innervation following extracellular matrix scaffold mediated remodeling of muscular tissues. Journal of Tissue Engineering and Regenerative Medicine, 3(8), 590–600.
Chan, B. P., & Leong, K. W. (2008). Scaffolding in tissue engineering: general approaches and tissue-specific considerations. European Spine Journal, 17(Suppl 4), 467–479.
Nakayama, K. H., Batchelder, C. A., Lee, C. I., & Tarantal, A. F. (2011). Renal tissue engineering with decellularized rhesus monkey kidneys: age-related differences. Tissue Engineering. Part A, 17(23–24), 2891–2901.
Lohan, A., Stoll, C., Albrecht, M., et al. (2013). Human hamstring tenocytes survive when seeded into a decellularized porcine Achilles tendon extracellular matrix. Connect Tissue Researc, 54(4–5), 305–312.
Schulze-Tanzil, G., Al-Sadi, O., Ertel, W., & Lohan, A. (2012). Decellularized tendon extracellular matrix—a valuable approach for tendon reconstruction? Cells, 1(4), 1010–1028.
Haykal, S., Zhou, Y., Marcus, P., et al. (2013). The effect of decellularization of tracheal allografts on leukocyte infiltration and of recellularization on regulatory T cell recruitment. Biomaterials, 34(23), 5821–5832.
Lynch, K., & Pei, M. (2014). Age associated communication between cells and matrix: a potential impact on stem cell-based tissue regeneration strategies. Organogenesis, 10(3), 289–298.
Kretlow, J. D., Jin, Y. Q., Liu, W., et al. (2008). Donor age and cell passage affects differentiation potential of murine bone marrow-derived stem cells. BMC Cell Biology, 9, 60.
Maredziak, M., Marycz, K., Tomaszewski, K. A., et al. (2016). The influence of aging on the regenerative potential of human adipose derived mesenchymal stem cells. Stem Cells International, 2016, 2152435.
Zheng, L., Fan, H. S., Sun, J., et al. (2010). Chondrogenic differentiation of mesenchymal stem cells induced by collagen-based hydrogel: an in vivo study. Journal of Biomedical Materials Research. Part A, 93(2), 783–792.
Bhardwaj, N., & Kundu, S. C. (2012). Chondrogenic differentiation of rat MSCs on porous scaffolds of silk fibroin/chitosan blends. Biomaterials, 33(10), 2848–2857.
Eslaminejad, M. B., Mirzadeh, H., Mohamadi, Y., & Nickmahzar, A. (2007). Bone differentiation of marrow-derived mesenchymal stem cells using beta-tricalcium phosphate-alginate-gelatin hybrid scaffolds. Journal of Tissue Engineering and Regenerative Medicine, 1(6), 417–424.
Mauck, R. L., Yuan, X., & Tuan, R. S. (2006). Chondrogenic differentiation and functional maturation of bovine mesenchymal stem cells in long-term agarose culture. Osteoarthritis Cartilage, 14(2), 179–189.
Chung, C., & Burdick, J. A. (2009). Influence of three-dimensional hyaluronic acid microenvironments on mesenchymal stem cell chondrogenesis. Tissue Engineering Part A, 15(2), 243–254.
Han, Y., Wei, Y., Wang, S., & Song, Y. (2010). Cartilage regeneration using adipose-derived stem cells and the controlled-released hybrid microspheres. Joint Bone Spine, 77(1), 27–31.
Fan, H., Hu, Y., Zhang, C., et al. (2006). Cartilage regeneration using mesenchymal stem cells and a PLGA-gelatin/chondroitin/hyaluronate hybrid scaffold. Biomaterials, 27(26), 4573–4580.
Rackwitz, L., Djouad, F., Janjanin, S., et al. (2014). Functional cartilage repair capacity of de-differentiated, chondrocyte- and mesenchymal stem cell-laden hydrogels in vitro. Osteoarthritis Cartilage, 22(8), 1148–1157.
Chimal-Monroy, J., & Diaz de Leon, L. (1999). Expression of N-cadherin, N-CAM, fibronectin and tenascin is stimulated by TGF-beta1, beta2, beta3 and beta5 during the formation of precartilage condensations. International Journal of Developmental Biology, 43(1), 59–67.
Jian, H., Shen, X., Liu, I., et al. (2006). Smad3-dependent nuclear translocation of beta-catenin is required for TGF-beta1-induced proliferation of bone marrow-derived adult human mesenchymal stem cells. Genes & Development, 20(6), 666–674.
O'Sullivan, J., D'Arcy, S., Barry, F. P., et al. (2011). Mesenchymal chondroprogenitor cell origin and therapeutic potential. Stem Cell Research & Theraphy, 2(1), 8.
Murphy, M. B., Moncivais, K., & Caplan, A. I. (2013). Mesenchymal stem cells: environmentally responsive therapeutics for regenerative medicine. Experimental & Molecular Medicine, 45, e54.
Cameron, T. L., Belluoccio, D., Farlie, P. G., et al. (2009). Global comparative transcriptome analysis of cartilage formation in vivo. BMC Developmental Biology, 9, 20.
Pittenger, M. F., Mackay, A. M., Beck, S. C., et al. (1999). Multilineage potential of adult human mesenchymal stem cells. Science, 284(5411), 143–147.
Krampera, M., Pizzolo, G., Aprili, G., & Franchini, M. (2006). Mesenchymal stem cells for bone, cartilage, tendon and skeletal muscle repair. Bone, 39(4), 678–683.
Arinzeh, T. L. (2005). Mesenchymal stem cells for bone repair: preclinical studies and potential orthopedic applications. Foot and Ankle Clinics, 10(4), 651–665 viii.
Cornelissen, A. S., Maijenburg M. W., Nolte M. A., & Voermans C. (2015) Organ-specific migration of mesenchymal stromal cells: Who, when, where and why? Immunol Lett, 168(2), 159-169.
Bocker, W., Docheva, D., Prall, W. C., et al. (2008). IKK-2 is required for TNF-alpha-induced invasion and proliferation of human mesenchymal stem cells. Journal Molecular Medicine (Berl), 86(10), 1183–1192.
Bobis, S., Jarocha, D., & Majka, M. (2006). Mesenchymal stem cells: characteristics and clinical applications. Folia Histochemica et Cytobiologica, 44(4), 215–230.
Ozawa, K., Sato, K., Oh, I., et al. (2008). Cell and gene therapy using mesenchymal stem cells (MSCs). Journal of Autoimmunity, 30(3), 121–127.
Kotobuki, N., Katsube, Y., Katou, Y., et al. (2008). In vivo survival and osteogenic differentiation of allogeneic rat bone marrow mesenchymal stem cells (MSCs). Cell Transplantation, 17(6), 705–712.
Cipriani, P., Di Benedetto, P., Liakouli, V., et al. (2013). Mesenchymal stem cells (MSCs) from scleroderma patients (SSc) preserve their immunomodulatory properties although senescent and normally induce T regulatory cells (Tregs) with a functional phenotype: implications for cellular-based therapy. Clinical and Experimental Immunology, 173(2), 195–206.
Fazekasova, H., Lechler, R., Langford, K., & Lombardi, G. (2011). Placenta-derived MSCs are partially immunogenic and less immunomodulatory than bone marrow-derived MSCs. Journal of Tissue Engineering and Regenerative Medicine, 5(9), 684–694.
Glenn, J. D., & Whartenby, K. A. (2014). Mesenchymal stem cells: emerging mechanisms of immunomodulation and therapy. World Journal of Stem Cells, 6(5), 526–539.
Paebst, F., Piehler, D., Brehm, W., et al. (2014). Comparative immunophenotyping of equine multipotent mesenchymal stromal cells: an approach toward a standardized definition. Cytometry. Part A, 85(8), 678–687.
Carrade, D. D., Affolter, V. K., Outerbridge, C. A., et al. (2011). Intradermal injections of equine allogeneic umbilical cord-derived mesenchymal stem cells are well tolerated and do not elicit immediate or delayed hypersensitivity reactions. Cytotherapy, 13(10), 1180–1192.
Pigott, J. H., Ishihara, A., Wellman, M. L., et al. (2013). Investigation of the immune response to autologous, allogeneic, and xenogeneic mesenchymal stem cells after intra-articular injection in horses. Veterinary Immunology Immunopathology, 156(1–2), 99–106.
Chen, K., Wang, D., Du, W. T., et al. (2010). Human umbilical cord mesenchymal stem cells hUC-MSCs exert immunosuppressive activities through a PGE2-dependent mechanism. Clinical Immunology, 135(3), 448–458.
Jui, H. Y., Lin, C. H., Hsu, W. T., et al. (2012). Autologous mesenchymal stem cells prevent transplant arteriosclerosis by enhancing local expression of interleukin-10, interferon-gamma, and indoleamine 2,3-dioxygenase. Cell Transplantation, 21(5), 971–984.
Yoo, K. H., Jang, I. K., Lee, M. W., et al. (2009). Comparison of immunomodulatory properties of mesenchymal stem cells derived from adult human tissues. Cell Immunology, 259(2), 150–156.
Montespan, F., Deschaseaux, F., Sensebe, L., et al. (2014). Osteodifferentiated mesenchymal stem cells from bone marrow and adipose tissue express HLA-G and display immunomodulatory properties in HLA-mismatched settings: implications in bone repair therapy. Journal of Immunology Research, 2014, 230346.
Chung, D. J., Choi, C. B., Lee, S. H., et al. (2009). Intraarterially delivered human umbilical cord blood-derived mesenchymal stem cells in canine cerebral ischemia. Journal of Neuroscience Research, 87(16), 3554–3567.
Dharmasaroja, P. (2009). Bone marrow-derived mesenchymal stem cells for the treatment of ischemic stroke. Journal of Clinical Neuroscience, 16(1), 12–20.
Noel, D., Djouad, F., Bouffi, C., et al. (2007). Multipotent mesenchymal stromal cells and immune tolerance. Leukemia & Lymphoma, 48(7), 1283–1289.
Carrade, D. D., Lame, M. W., Kent, M. S., et al. (2012). Comparative analysis of the immunomodulatory properties of equine adult-derived mesenchymal stem cells(). Cell Medicine, 4(1), 1–11.
Carrade Holt, D. D., Wood, J. A., Granick, J. L., et al. (2014). Equine mesenchymal stem cells inhibit T cell proliferation through different mechanisms depending on tissue source. Stem Cells and Development, 23(11), 1258–1265.
Gore, A. V., Bible, L. E., Song, K., et al. (2015). Mesenchymal stem cells increase T-regulatory cells and improve healing following trauma and hemorrhagic shock. Journal of Trauma and Acute Care Surgery, 79(1), 48–52.
Duffy, M. M., Ritter, T., Ceredig, R., & Griffin, M. D. (2011). Mesenchymal stem cell effects on T-cell effector pathways. Stem Cell Research and Ther, 2(4), 34.
Kang, J. W., Koo, H. C., Hwang, S. Y., et al. (2012). Immunomodulatory effects of human amniotic membrane-derived mesenchymal stem cells. Journal of Veterinary Science, 13(1), 23–31.
Ryan, J. M., Barry, F. P., Murphy, J. M., & Mahon, B. P. (2005). Mesenchymal stem cells avoid allogeneic rejection. Journal of Inflammation (Lond), 2, 8.
Zhang, Y., Li, J., Davis, M. E., & Pei, M. (2015). Delineation of in vitro chondrogenesis of human synovial stem cells following preconditioning using decellularized matrix. Acta Biomaterialia, 20, 39–50.
Dickhut, A., Pelttari, K., Janicki, P., et al. (2009). Calcification or dedifferentiation: requirement to lock mesenchymal stem cells in a desired differentiation stage. Journal of Cellular Physiology, 219(1), 219–226.
Burk, J., I. Ribitsch, C. Gittel, et al., Growth and differentiation characteristics of equine mesenchymal stromal cells derived from different sources (2013). Veterinary Journal, 195(1), 98–106.
Fan, J., Gong, Y., Ren, L., et al. (2010). In vitro engineered cartilage using synovium-derived mesenchymal stem cells with injectable gellan hydrogels. Acta Biomaterialia, 6(3), 1178–1185.
Fan, J., Ren, L., Liang, R., et al. (2010). Chondrogenesis of synovium-derived mesenchymal stem cells in photopolymerizing hydrogel scaffolds. Journal of Biomaterials Science. Polymer Edition, 21(12), 1653–1667.
Luo, L., Eswaramoorthy, R., Mulhall, K. J., & Kelly, D. J. (2015). Decellularization of porcine articular cartilage explants and their subsequent repopulation with human chondroprogenitor cells. Journal of Mechanical Behavior Biomedical Materials, 55, 21–31.
Bautista, C. A., Park, H. J., Mazur, C. M., et al. (2016). Effects of chondroitinase abc-mediated proteoglycan digestion on decellularization and recellularization of articular cartilage. PLoS One, 11(7), e0158976.
Meretoja, V. V., Dahlin, R. L., Kasper, F. K., & Mikos, A. G. (2012). Enhanced chondrogenesis in co-cultures with articular chondrocytes and mesenchymal stem cells. Biomaterials, 33(27), 6362–6369.
Farrell, E., Both, S. K., Odorfer, K. I., et al. (2011). In-vivo generation of bone via endochondral ossification by in-vitro chondrogenic priming of adult human and rat mesenchymal stem cells. BMC Musculoskeletal Disorders, 12, 31.
Levorson, E. J., Hu, O., Mountziaris, P. M., et al. (2013). Cell-derived polymer/extracellular matrix composite scaffolds for cartilage regeneration, Part 2: construct devitalization and determination of chondroinductive capacity. Tissue Engineering. Part C, Methods, 20(4), 358–372.
Tsai, T. L., Nelson, B. C., Anderson, P. A., et al. (2014). Intervertebral disc and stem cells cocultured in biomimetic extracellular matrix stimulated by cyclic compression in perfusion bioreactor. Spine Journal., 14(9), 2127–2140.
Holzwarth, C., Vaegler, M., Gieseke, F., et al. (2010). Low physiologic oxygen tensions reduce proliferation and differentiation of human multipotent mesenchymal stromal cells. BMC Cell Biology, 11, 11.
D'Ippolito, G., Diabira, S., Howard, G. A., et al. (2006). Low oxygen tension inhibits osteogenic differentiation and enhances stemness of human MIAMI cells. Bone, 39(3), 513–522.
Grayson, W. L., Zhao, F., Bunnell, B., & Ma, T. (2007). Hypoxia enhances proliferation and tissue formation of human mesenchymal stem cells. Biochemical and Biophysical Research Communications, 358(3), 948–953.
Fermor, B., Christensen, S. E., Youn, I., et al. (2007). Oxygen, nitric oxide and articular cartilage. European Cell Materials, 13, 56–65 discussion 65.
Kanichai, M., Ferguson, D., Prendergast, P. J., & Campbell, V. A. (2008). Hypoxia promotes chondrogenesis in rat mesenchymal stem cells: a role for AKT and hypoxia-inducible factor (HIF)-1alpha. Journal of Cellular Physiology, 216(3), 708–715.
Loboda, A., Jozkowicz, A., & Dulak, J. (2010). HIF-1 and HIF-2 transcription factors--similar but not identical. Molecules and Cells, 29(5), 435–442.
Adesida, A. B., Mulet-Sierra, A., & Jomha, N. M. (2012). Hypoxia mediated isolation and expansion enhances the chondrogenic capacity of bone marrow mesenchymal stromal cells. Stem Cell Research & Theraphy, 3(2), 9.
Duval, E., Bauge, C., Andriamanalijaona, R., et al. (2012). Molecular mechanism of hypoxia-induced chondrogenesis and its application in in vivo cartilage tissue engineering. Biomaterials, 33(26), 6042–6051.
Meretoja, V. V., Dahlin, R. L., Wright, S., et al. (2013). The effect of hypoxia on the chondrogenic differentiation of co-cultured articular chondrocytes and mesenchymal stem cells in scaffolds. Biomaterials, 34(17), 4266–4273.
Xu, Y., Malladi, P., Chiou, M., et al. (2007). In vitro expansion of adipose-derived adult stromal cells in hypoxia enhances early chondrogenesis. Tissue Engineering, 13(12), 2981–2993.
Ceradini, D. J., & Gurtner, G. C. (2005). Homing to hypoxia: HIF-1 as a mediator of progenitor cell recruitment to injured tissue. Trends in Cardiovascular Medicine, 15(2), 57–63.
Rafii, S., & Lyden, D. (2003). Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. National Medical, 9(6), 702–712.
Hillebrandt, K., Polenz, D., Butter, A., et al. (2015). Procedure for decellularization of rat livers in an oscillating-pressure perfusion device. Journal of Visualized Experiments, 102, e53029.
Partington, L., Mordan, N. J., Mason, C., et al. (2013). Biochemical changes caused by decellularization may compromise mechanical integrity of tracheal scaffolds. Acta Biomaterialia, 9(2), 5251–5261.
Shaari, C. M., Farber, D., Brandwein, M. S., et al. (1998). Characterizing the antigenic profile of the human trachea: implications for tracheal transplantation. Head & Neck, 20(6), 522–527.
Ye, K., Felimban, R., Moulton, S. E., et al. (2013). Bioengineering of articular cartilage: past, present and future. Regenerative Medicine, 8(3), 333–349.
Hammer, N., Huster, D., Boldt, A., et al. (2016). A preliminary technical study on sodium dodecyl sulfate-induced changes of the nano-structural and macro-mechanical properties in human iliotibial tract specimens. Journal of Mechanical Behavior Biomedical Materials, 61, 164–173.
Urist, M. R. (1965). Bone: formation by autoinduction. Science, 150(3698), 893–899.
Kajbafzadeh, A. M., Sabetkish, S., Sabetkish, N., et al. (2015). In-vivo trachea regeneration: fabrication of a tissue-engineered trachea in nude mice using the body as a natural bioreactor. Surgery Today, 45(8), 1040–1048.
Elsaesser, A. F., Bermueller, C., Schwarz, S., et al. (2014). In vitro cytotoxicity and in vivo effects of a decellularized xenogeneic collagen scaffold in nasal cartilage repair. Tissue Engineering Part A, 20(11–12), 1668–1678.
Batioglu-Karaaltin, A., Karaaltin, M. V., Ovali, E., et al. (2015). In vivo tissue-engineered allogenic trachea transplantation in rabbits: a preliminary report. Stem Cell Reviews, 11(2), 347–356.
Macchiarini, P., Jungebluth, P., Go, T., et al. (2008). Clinical transplantation of a tissue-engineered airway. Lancet, 372(9655), 2023–2030.
Gonfiotti, A., Jaus, M. O., Barale, D., et al. (2014). The first tissue-engineered airway transplantation: 5-year follow-up results. Lancet, 383(9913), 238–244.
Cheng, N. C., Estes, B. T., Awad, H. A., & Guilak, F. (2009). Chondrogenic differentiation of adipose-derived adult stem cells by a porous scaffold derived from native articular cartilage extracellular matrix. Tissue Engineering. Part A, 15(2), 231–241.
Yang, B., Zhang, Y., Zhou, L., et al. (2010). Development of a porcine bladder acellular matrix with well-preserved extracellular bioactive factors for tissue engineering. Tissue Engineering. Part C, Methods, 16(5), 1201–1211.
Gong, Y. Y., Xue, J. X., Zhang, W. J., et al. (2011). A sandwich model for engineering cartilage with acellular cartilage sheets and chondrocytes. Biomaterials, 32(9), 2265–2273.
Azhim, A., Ono, T., Fukui, Y., et al. (2013). Preparation of decellularized meniscal scaffolds using sonication treatment for tissue engineering. Conference Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2013, 6953–6956.
Petersen, T. H., Calle, E. A., Colehour, M. B., & Niklason, L. E. (2012). Matrix composition and mechanics of decellularized lung scaffolds. Cells, Tissues, Organs, 195(3), 222–231.
Schwarz, S., Elsaesser, A. F., Koerber, L., et al. (2015). Processed xenogenic cartilage as innovative biomatrix for cartilage tissue engineering: effects on chondrocyte differentiation and function. Journal of Tissue Engineering and Regenerative Medicine, 9(12), E239–E251.
Giraldo-Gomez, D. M., Leon-Mancilla, B., Del Prado-Audelo, M. L., et al. (2016). Trypsin as enhancement in cyclical tracheal decellularization: morphological and biophysical characterization. Materials Science & Engineering, C: Materials for Biological Applications, 59, 930–937.
Guo, L., Qu, J., Zheng, C., et al. (2015). Preparation and characterization of a novel decellularized fibrocartilage “book” scaffold for use in tissue engineering. PloS One, 10(12), e0144240.
Pinheiro, A., Cooley, A., Liao, J., et al. (2016). Comparison of natural crosslinking agents for the stabilization of xenogenic articular cartilage. Journal of Orthopaedic Research, 34(6), 1037–1046.
Kato, T., Miyaki, S., Ishitobi, H., et al. (2014). Exosomes from IL-1beta stimulated synovial fibroblasts induce osteoarthritic changes in particular chondrocytes. Arthritis Research & Therapy, 16(4), R163.
Acknowledgments
None.
Authors Contribution
GST and ZH wrote the manuscript and arranged tables and figs. OG revised the manuscript carefully.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
All authors received no funding for this work.
Conflict of Interest
All authors declare that there exists no potential conflict of interest.
Electronic supplementary material
ESM 1
(DOC 113 kb)
Rights and permissions
About this article

Cite this article
Huang, Z., Godkin, O. & Schulze-Tanzil, G. The Challenge in Using Mesenchymal Stromal Cells for Recellularization of Decellularized Cartilage. Stem Cell Rev and Rep 13, 50–67 (2017). https://doi.org/10.1007/s12015-016-9699-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12015-016-9699-8