
Abstract
Background
This study was designed to evaluate the survival outcomes of patients undergoing simple cholecystectomy and to investigate which patients would benefit from cholecystectomy alone in treating gallbladder carcinoma.
Methods
The available medical records of patients who underwent cholecystectomy alone for gallbladder carcinomas from August 1992 to February 2005 were retrospectively reviewed. Cancer stages were evaluated by clinical meaning based on the AJCC Cancer Staging Manual, 6th edition. “Clinical” R0, defined as gallbladder confined tumor (pT1-3 with negative resection margin) with cN0 and cM0, was tentatively established to evaluate the quality of simple cholecystectomy.
Results
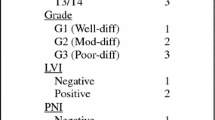
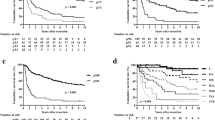
Seventy-five patients underwent cholecystectomy alone for gallbladder carcinomas. Twenty-eight patients were male, and forty-seven patients were female, with their mean age 63.5 years (range, 29-80 years). Forty-one patients (54.7%) underwent laparoscopic cholecystectomy, and thirty-four patients (45.3%) underwent open cholecystectomy. T3 lesions were most common (26 patients), followed by T1 (24 patients), T2 (19 patients), and T4 (6 patients). “Clinical R0” could be defined in 48 patients (63%) after simple cholecystectomy. Multivariate analysis showed that incidental gallbladder carcinoma, T stage, and clinical R0 status were independent prognostic factors of long-term survival. When comparing survival outcomes of clinical R0 according to the T stage, no patients with Tis, T1a, and T1b had cancer-related mortality during follow-up. Especially, in patients with T2 gallbladder carcinomas, the mean survival rate was 68.9 months, and the 5-year survival rate was 77.8%. On the contrary, those with T3 lesions had poor prognoses.
Conclusion
Cholecystectomy alone could be proper management for well-selected patients with gallbladder carcinomas (incidental gallbladder carcinoma, gallbladder confined carcinoma, clinical R0). More experiences and a proper prospective study must be performed to confirm the meaning of clinical R0 in treating gallbladder carcinoma.



Similar content being viewed by others
References
Destoll M. Rationis mendendi. In Batavorum L, Haak ET Socios A et J Honkoop, ed. Nosocomio practico vendobonensi, Part I, 1788.
DeRegato JA, Spjut HJ. Digestive tract/accessory organo-gallbladder. In Ackerman LV, DeRegato JA, (eds). Cancer-Diagnosis, Treatment and Prognosis, 5th ed. St Louis: CV Mosby, 1977, pp 599–604.
Wakai T, Shirai Y, Yokoyama N, Nagajura S, Watanabe H. Early carcinoma of the gallbladder. Eur J Surg 1992;158:545–548.
Togoroki T, Kawamoto T, Takahashi H, et al. Treatment of gallbladder cancer by radical resection. Br J Surg 1999;86:622–627.
Bartlett DL, Fong Y, Fortner JG, Brennan MF, Blumgart LH. Long-term results after resection for gallbladder cancer: implications for staging and management. Ann Surg 1955;142:6–16.
Misra S, Chaturvedi A, Misra NC, Sharma ID. Carcinoma of the gallbladder. Lancet Oncol 2003;4:167–176.
Shirai Y, Yoshida K, Tsukada K, Muto T. Inapparent carcinoma of the gallbladder: an appraisal of a radical second operation after simple cholecystectomy. Ann Surg 1992;2155:326–331.
Frederick LG, David LP, Irvin DF, et al. AJCC Cancer Staging Manual, 6th ed. Philadelphia: Lippincott-Raven; 2002.
Piehler JM, Crichlow RW. Primary carcinoma of the gallbladder. Surg Gynecol Obstet 1978;929–942.
Chijiwa K, Sumiyoshi K, Nakayama F. Impact of recent advances in hepatobiliary imaging techniques on the preoperative diagnosis of carcinoma of the gallbladder. World J Surg 1991;15:323–337.
Ueno N, Tomiyama T, Tano S, et al. Diagnosis of gallbladder carcinoma with color Doppler ultrasonography. Am J Gastroenterol 1996;91:1647–1649.
Azuma T, Yoshikawa T, Araida T, Takasaki K. Differential diagnosis of polypoid lesions of the gallbladder by endoscopic ultrasonography. Am J Surg 2001;181:65–70.
Shoup M, Fong Y. Surgical indications and extent of resection in gallbladder cancer. Surg Oncol Clin N Am 2002;11:285–294.
Sasaki R, Itabashi H, Fujita T, et al. Significance of extensive surgery including resection of the pancreas head for the treatment of gallbladder cancer-from the perspective of mode of lymph node involvement and surgical outcome. World J Surg 2006;30:36–42.
Fong Y. Treatment of T2 gallbladder carcinoma. Ann Surg Oncol 2003;10:490.
De Aretxabala X, Roa IS, Burgos LA, et al. Curative resection in potentially respectable tumors of the gallbladder. Eur J Surg 1997;163:419–426.
Fong Y, Jarnagin W, Blumgart LH. Gallbladder cancer: comparison of patients presenting initially for definitive operation with those presenting after prior noncurative intervention. Ann Surg 2000;232:557–569.
Suzuki S, Yokoi Y, Kurachi K, et al. Appraisal of surgical treatment for pT2 gallbladder carcinomas. World J Surg 2004;28:160–165.
Acknowledgement
We give special thanks to Seo Won. Youl (Biostatistical Supporting Laboratory Yonsei University College of Medicine) for so much advice in analyzing biostatics data.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kang, C.M., Lee, W.J., Choi, G.H. et al. Does “Clinical” R0 Have Validity in the Choice of Simple Cholecystectomy for Gallbladder Carcinoma?. J Gastrointest Surg 11, 1309–1316 (2007). https://doi.org/10.1007/s11605-007-0225-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-007-0225-9