
Abstract
Aims/hypothesis
The aim of the present study was to estimate the prevalence and healthcare costs of diabetic retinopathy (DR).
Methods
This population-based study included all residents (n = 251,386) in the catchment area of the eye clinic of Linköping University Hospital, Sweden. Among patients with diabetes (n = 12,026), those with and without DR were identified through register data from both the Care Data Warehouse in Östergötland, an administrative healthcare register, and the Swedish National Diabetes Register. Healthcare cost data were elicited by record linkage of these two registers to data for the year 2008 in the Cost Per Patient Database developed by Östergötland County Council.
Results
The prevalence of any DR was 41.8% (95% CI 38.9–44.6) for patients with type 1 diabetes and 27.9% (27.1–28.7) for patients with type 2 diabetes. Sight-threatening DR was present in 12.1% (10.2–14.0) and 5.0% (4.6–5.4) of the type 1 and type 2 diabetes populations respectively. The annual average healthcare cost of any DR was €72 (€53–91). Stratified into background retinopathy, proliferative DR, maculopathy, and the last two conditions combined, the costs were €26 (€10–42), €257 (€155–359), €216 (€113–318) and €433 (€232–635) respectively. The annual cost for DR was €106 000 per 100,000 inhabitants.
Conclusions
This study presents new information on the prevalence and costs of DR. Approximately one-third of patients with diabetes have some form of DR. Average healthcare costs increase considerably with the severity of DR, which suggests that preventing progression of DR may lower healthcare costs.
Similar content being viewed by others


Introduction
Approximately 220 million people in the world suffer from diabetes mellitus [1]. The risk of micro- and macrovascular complications of diabetes is great, with possible complications including retinopathy, nephropathy, neuropathy, heart disease, stroke and non-traumatic lower extremity amputations [2]. Diabetic retinopathy (DR), the vision-related complication, affects the vessels in the patient’s eyes and is one of the main causes of blindness [3]. The prevalence of DR has been estimated in several studies, including large studies such as the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) [4, 5], the UK Prospective Diabetes Study (UKDPS) [6] and the DCCT [7]. Klein et al. (WESDR) have reported that, after 15 years of diabetes duration, virtually all individuals diagnosed with diabetes at less than 30 years of age and more than 70% of individuals diagnosed aged 30 years or older develop retinopathy [4, 5]. Many of the studies available on the prevalence of DR are relatively old, however, and improvements in diabetes care over recent decades [8] have led to a call for updated estimates of the prevalence and severity of DR. More recent studies including updated estimations of the prevalence of DR have been published (e.g. [9–12]) but are, in general, based on study populations limited to patients of specific ages or with particular duration of diabetes.
In addition to constituting a physical and emotional burden to patients [13], DR also represents an economic burden to society. Estimating the size of this burden is important, as it plays a central role in the decision on whether or not to implement new treatments for the disease. By calculating the potential cost savings of treatments that reduce the risk of DR, the costs of DR can be used as an input in cost-effectiveness analyses, contributing valuable information to decision-makers concerning the cost-effectiveness of different treatment alternatives. In the USA, the total direct medical costs of DR in adults have been estimated at €342 (US$493) million per year and the average treatment cost per patient with DR at €436 (US$629) per year [14]. The societal cost of DR in Germany for the year 2002 has been estimated [15] to be €1433 per patient. However, to our knowledge no study to date has presented costs of DR specified by severity level among type 1 as well as type 2 diabetes patients using a population-based approach.
To gain an overview of the current situation of DR, there is a need for updated prevalence estimates and cost estimates independent of age and diabetes duration. Thus, the main aim of the present population-based study was to estimate the prevalence and additional healthcare costs of DR, both for any DR and for different DR severity levels.
Methods
The current study is a cross-sectional population-based register study of the prevalence and annual additional healthcare costs of DR. Patients with diabetes with and without DR were identified through register data from both the Care Data Warehouse in Östergötland (CDWÖ) and the National Diabetes Register (NDR). The healthcare cost of DR was elicited by linking and matching data in these two registers to data in the Cost Per Patient (CPP) Database. The study was approved by the local ethics committee in Linköping.
Study population
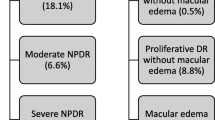
All individuals who at the time of inclusion were registered at a primary healthcare centre and were living in the catchment area of the eye clinic of Linköping University Hospital in the county of Östergötland, Sweden (n = 251,386) were included in the study (virtually all inhabitants in the county of Östergötland are registered at a primary healthcare centre). The county of Östergötland is the fifth largest county in Sweden, with a relatively high proportion of employment in manufacturing (24%) [16]. Our study population covers approximately 60% of the population of Östergötland. Linköping University Hospital is one of three hospitals in the county and contains one of the county’s two eye clinics. All individuals with diabetes covered by this clinic are screened for DR at regular intervals. The catchment area of the eye clinic in Linköping has an age and sex distribution similar to the national distribution [17] and the percentage of individuals with higher education is 19.2% (the national average is 18.0%) [18]. The selection of the study population is shown in Fig. 1.

Population selection diagram. Solid line shows the division of the study population into subpopulations. Dashed line shows which groups have been compared to calculate the additional average cost of DR
Data sources
The CDWÖ is an administrative database recording the date, name, unique personal identification number and diagnosis (main diagnosis and up to nine secondary diagnoses) according to the International Classification of Diseases, 10th version (ICD-10), for every healthcare visit or stay within the county of Östergötland. Information on all healthcare resources provided by the county council has been recorded in the CDWÖ since 1999. Data from the healthcare units were formerly transferred to the register each month, but are now, thanks to the electronic patient record system, transferred on a daily basis. Since diabetes is a chronic disease involving continuous contact with the healthcare system, virtually all patients with diagnosed diabetes living in the county are registered in the CDWÖ (except for those only visiting a few private practices that are not connected to the CDWÖ, none of which specialises in DR treatment, and those who have been misclassified in the registration process). This database has previously been described in greater detail [19].
Data from the CDWÖ were compared and complemented with data on DR from the NDR. The NDR [20] was initiated in 1996 to serve as a tool for continuous quality assessment of Swedish diabetes care and for benchmarking against national treatment goals. Demographic factors, diabetes duration, treatment modalities, diabetes complications and risk factors are registered annually for patients 18 years and older, based on data from actual patient visits to primary healthcare or hospital outpatient clinics. Registration is carried out voluntarily by nurses or physicians by completing a paper form, using database software or through the NDR website.
Data from the CDWÖ and the NDR were also matched and linked to data in a regional cost database, held by Östergötland County Council. This database is based on a patient-related cost-accounting method called Cost Per Patient (CPP), which was introduced by the Swedish Association of Local Authorities and Regions [21]. The national CPP project was initiated to develop a useful tool for improvements in the allocation of resources to the healthcare sector by creating national principles and models for CPP accounts in all sectors of the health service. Healthcare costs are, in accordance with the national CPP principle, calculated by a four-step procedure using a bottom-up approach [22]. First, relevant healthcare costs are identified in the overall budget. Second, identified costs are divided into patient-related costs and costs for joint activities. The joint activities are also distributed between healthcare units. Third, healthcare services are described and the costs of these calculated. Fourth and finally, the consumption of different services is linked to specific healthcare contacts. The regional CPP database contains costs for all healthcare services within Östergötland County, and, combined with the CDWÖ, offers individual-based cost data that may be summarised for certain populations or clinics. Together with patient data concerning ICD-10 codes from the CDWÖ, these cost calculations make it possible to perform prevalence-based cost studies for specific diseases.
Data collection
Patients with diabetes were identified in the CDWÖ by a search for patients who had been in contact with healthcare providers between 2000 and 2007 and had been assigned one of the ICD-10 codes E10, E11 or E14 as a main or secondary diagnosis. Individuals in the CDWÖ were defined as having type 1 diabetes if they were registered with ICD-10 code E10, and type 2 if registered with codes E11 or E14. To be considered as having DR, based on the registrations in the CDWÖ, one of the following ICD-10 codes had to be registered for at least one eye: H36.0A, H36.0B or H36.0X. Individuals with only H36.0A were classified as having background retinopathy (BR), individuals with HR36.0B but not H36.0X as having proliferative diabetic retinopathy (PDR), individuals with H36.0X but not H36.0B as having maculopathy, and individuals with H36.0X and H36.0B as having PDR as well as maculopathy. Although H36.0X is a code for unspecified DR, at the eye clinic at Linköping University Hospital it has been used to designate maculopathy. In the NDR, DR is reported by marking any of the assigned boxes representing yes, no or unknown. If the answer is yes, the respondent is asked for complementary information concerning type of retinopathy and whether treatment has been provided.
Prevalence estimates
The prevalence of DR on 31 December 2007 was estimated using data from both the CDWÖ and the NDR. Based on the assumption that no patients had been diagnosed with DR if DR was not present, we defined a case of DR as having a diagnosis of the complication in at least one of the two registers. The prevalence was estimated as the ratio of the number of patients with an identified diagnosis of DR to the number of individuals with diabetes in the total population covered by the eye clinic at Linköping University Hospital at the same time point. Using the available data in the CDWÖ concerning the different severity levels of DR, it was also possible to estimate the prevalence of BR, PDR, maculopathy, and PDR in combination with maculopathy. Individuals registered as having DR in the NDR but not in the CDWÖ were excluded from this analysis as no information was available on their DR severity level. In cases of more than one severity level for the same patient, the condition of the worse eye was used to determine which group the patient should belong to. When maculopathy and BR were present in the same individual, the patient was included in the maculopathy group. The prevalence of DR and the four severity levels was estimated for type 1 and type 2 diabetes as well as for men and women. The prevalence of diabetes is based only on registrations in the CDWÖ. Prevalence estimates are presented with 95% CI.
Cost estimates
The healthcare costs of DR were defined as all costs attributable to diagnosing or treating DR at the eye clinic. Included in these costs are, for example, hospital overheads, ophthalmologist fees, eye examinations including photographs of the retina, photocoagulation, hospitalisations and other resource use related to vitrectomy. Based on the prevalence estimates, an average healthcare cost for 2008 was calculated for individuals with any severity of DR as well as for individuals with diabetes but no DR. The average additional costs of DR were estimated by subtracting the average cost for diabetic patients without DR from the average costs for diabetic patients with DR:
C DRi represents the individual costs for patients with diabetes and DR, while C noDRi represents the individual costs for patients with diabetes but without DR. N DR is the number of patients with diabetes and DR, and N noDR the number of patients with diabetes but without DR. The same method was used to estimate the costs of the four severity levels of DR (BR, PDR, maculopathy, and PDR in combination with maculopathy). To calculate the average costs for the different severity levels, each severity group was compared with the group without DR. The comparisons between groups for the calculation of costs are shown in Fig. 1 by dotted lines. Individuals diagnosed with DR in 2008 were included in the DR group. The cost estimates were standardised for age and sex using the distributions of the groups with DR and were presented with 95% CI. Costs were converted from Swedish kronor to euros using an exchange rate of 10.24 SEK/€.
Results
The prevalence of diabetes was 4.8% (95% CI 4.7–4.9). Of these, 9.6% (1,149/12,026) had type 1 diabetes and 90.4% (10,877/12,026) type 2 diabetes. The diabetes prevalence was 4.5% (95% CI 4.4–4.6) among women and 5.0% (95% CI 4.9–5.2) among men.
Prevalence of DR
Of the individuals with diabetes, 29.2% (95% CI 28.4–30.0) were registered as having DR. However, the majority of these, approximately 80%, did not have sight-threatening DR (i.e. PDR and/or maculopathy). Prevalence estimates for DR divided into sex and type of diabetes are presented in Table 1. The mean age of patients with and without DR was 67.2 (95% CI 66.7–67.7) and 67.6 (95% CI 67.3–68.0) years respectively.
Of the individuals identified in the CDWÖ as having diabetes, 66.0% (7,932/12,026) were registered in the NDR in 2007. However, information on whether or not the individuals had DR was recorded in this register for only 43.6% (5,244/12,026). For these patients, a comparison of the DR registrations is included in Table 2. The level of agreement between the two registers regarding DR registration was 86.3%.
Healthcare costs for DR
The annual healthcare cost of any DR was estimated at €72 (95% CI 53–91) per patient (Table 3). The corresponding costs of BR, PDR, maculopathy, and PDR and maculopathy combined were €26 (95% CI 10–42), €257 (95% CI 155–359) and €216 (95% CI 113–318) and €433 (€232–635) respectively. By multiplying the estimation of DR prevalence by the average costs for DR, a Swedish annual healthcare cost was approximated for DR. For this extrapolation we assumed that the Swedish population was 9,302,000 [23] and that 4.9% of these have diabetes [24]. The total healthcare costs of DR in Sweden add up to approximately €9.9 million per year, representing an overall healthcare cost of €106,000 per 100,000 inhabitants.
Discussion
In this study we estimated the prevalence and annual healthcare costs of DR in a diabetic population. Our results show that the prevalence of any DR in the total diabetic population is 29.2%. DR was more frequent among patients with type 1 diabetes than among those with type 2 diabetes, with DR prevalence of 41.8% and 27.9% respectively. The prevalence of DR was also significantly higher for men (30.9%) than for women (27.4%). Sight-threatening retinopathy such as PDR and maculopathy was present in 5.7% of all individuals with diabetes. The study also showed that treatment of DR costs €72 per year per patient. The costs varied considerably, however, between different severity levels of the disease and were estimated at €26, €257, €216 and €433 per patient per year for BR, PDR, maculopathy, and PDR combined with maculopathy respectively. Combined, the results for prevalence and average costs yielded an annual total healthcare cost of DR of €106,000 per 100 000 inhabitants.
The main strengths of this study are the large size of the study population and the fact that, being based on register data, it covers an entire population. However, even though the register-based method eliminates the risk of recall bias, it includes a risk of misclassification, such as missed or erroneous registrations. This risk of misclassification of DR was reduced in the present study by using information from two different registers. For approximately 40% of the diabetic population, we were able to compare the DR diagnoses in the CDWÖ with registrations of DR in the NDR. This comparison showed that 96.8% (1993/2058) of the total cases of DR in our population were identified in the CDWÖ. Assuming that this sensitivity is also valid for the remaining 60%, this gives a maximum prevalence of any DR of 29.9%, which is very close to our original figure of 29.2%. In total, the level of agreement between the two registers was approximately 86%. The 14% on which the registers disagreed were mainly cases in which individuals had received a DR diagnosis in the CDWÖ but not in the NDR. A possible explanation for this could be that patients with diabetes are registered in the NDR voluntarily at any time during the year, which could be before the patient has been screened for DR. New cases of DR that are detected after the registration form has been sent to the NDR would consequently not be registered until the following year. Of course, there may still be a few cases of DR that have been missed in both the registers we have used, which could have led to an underestimation of the prevalence of DR. However, our estimates may be further validated by comparison with the results of a previous study [25] from a region included in the catchment area of the present study. All patients <70 years old with type 2 diabetes living in this region had been screened for DR, with the results showing a prevalence of BR of 19.8% and a prevalence of severe DR of 6.7% (22.5% and 5.0% in the present study). Our estimates for the prevalence of diabetes (types 1 and 2), which were 4.5% among women and 5.0% among men, were based only on registrations in the CDWÖ but correspond well with the self-reported prevalence published in a report by the Swedish National Institute of Public Health [24] (4% for women and 5% for men among individuals 16–84 years old in Östergötland).
A further strength of the current study is that we had good information on the local practice behind the data in the registers we used. This information made us aware of the differences in practice between the county’s two eye clinics, which resulted in a decision to limit our study population to the catchment area of the eye clinic at Linköping University Hospital (M. Abrahamsson, personal communication).
It also made us aware of the potential risk that not all cases of maculopathy had been registered in the last months of the period for which we searched the CDWÖ, and that individuals diagnosed with maculopathy for the first time in the last months may thus mistakenly have been included in the BR or PDR groups. Since this would have concerned only the registration of a few individuals, we do not believe that it would have substantially affected the prevalence of the different severity levels.
A limitation of the study is that the DR patients identified solely through the NDR could not be classified into a specific severity level, which may have caused a slight underestimation of the prevalence of BR, PDR and maculopathy. As these patients (1.8% of our DR population) were not registered with a diagnosis of DR in the CDWÖ during the period of data extraction (2000–2007), they are not likely to have had DR for a long period, and we may therefore suspect that the majority of these belong to the BR group. If we include these patients in the BR group, the prevalence of BR increases from 23.2% to 23.6%. A second limitation is that we could not identify patients who were blind, since there is no specific ICD 10-code for blindness. As a result, patients with DR who became blind before the year 2000 have been classified as not having DR, which might have affected the estimates of prevalence as well as costs. However, only a negligible number of individuals (approximately 20) in the catchment area of the eye clinic of Linköping University Hospital are known to be blind as a consequence of DR (unpublished data, patient register at the Vision Central, Linköping University Hospital). Further, most of these individuals are no longer receiving treatment and are therefore not expected to generate large healthcare costs. That blindness increases costs in other areas of society is beyond the perspective of this study. It could also be considered a limitation that we have used costs from a regional database. However, there are various reasons for us to believe that these costs can be extrapolated to a national level. First, the demographics of the patients included in the database are similar to those of the national population [17]. Second, there are national guidelines concerning treatment of diabetes and diabetic retinopathy [26, 27]. Third, healthcare costs in Östergötland have been seen to be similar to national healthcare costs [28]. Furthermore, previous studies within other disease areas have used cost data from the CPP database to approximate costs on an aggregate national level [29].
Our prevalence estimates for any DR, for type 1 as well as type 2 diabetes, are substantially lower than those reported in two previous studies from Sweden [30, 31], in which the authors have reported a DR prevalence of more than 60% for younger-onset diabetes and over 35% for older-onset diabetes. However, both of these clinic-based studies were conducted almost two decades ago, which might explain some of the differences from our study. Over recent decades, diabetes care has improved in terms of decreased mean HbA1c and mean systolic blood pressure [8], changes that have been shown to have a preventive effect on diabetic complications [32, 33]. Previous research [34, 35] has shown a similar effect on the incidence of DR in Sweden. However, for type 2 diabetes, this explanation is contradicted by two Swedish population-based studies from the same time period [25, 36]. Lundman et al. [36] have reported a DR prevalence of 18.7% in non-insulin-dependent adults living in a county in central Sweden, and Falkenberg et al. [25] have reported a prevalence of 26.5% among type 2 diabetic patients <70 years old living in a rural area within the catchment area of the eye clinic of Linköping University Hospital. Our results for any DR are in line with the results from an American study from 2007 [10], in which the authors have reported a prevalence of 27.4% among individuals aged 40 years or older with diabetes. For the same age interval the prevalence of DR in our study was estimated to be 29.4%.
Comparing our results on the healthcare costs of any DR with the results of other studies is difficult because many cost studies lack information on the prevalence of PDR and maculopathy. The costs of PDR (€257), maculopathy (€216) and of both complications combined (€433) reported here could, however, be compared with the results of a German study [15] and a Canadian study [37]. Including only costs for ophthalmologist fees, medication and hospitalisation—corresponding to our definition of healthcare costs—the estimations from the German study give an average cost of €468 for patients with PDR and €681 for macular oedema. In the Canadian study, the costs for PDR, macular oedema and both complications combined were estimated to be €284, €254 and €333 respectively in the first year of these conditions. The annual subsequent cost was €26 for all these health states. Differences between these results and those of the present study could perhaps be explained by dissimilarities in how DR is treated in different countries. In Sweden, PDR is treated with photocoagulation, and in severe cases by vitrectomy, while maculopathy is primarily treated with photocoagulation. At present, pharmaceuticals are usually not used to treat DR. Other possible explanations are differences in the definitions used for classification of the different severity levels, and different proportions of type 1 and type 2 diabetes in the study populations. Regarding the German study, another explanation for the higher costs could be that only patients who had received treatment during the year for which their costs were calculated were included in the study.
In summary, the present study offers not only information on prevalence and costs of DR in Sweden but also information on the prevalence of diabetes. Approximately 5% of the population have diabetes, and approximately one-third of these patients have some form of DR. Of all patients with diabetes, approximately 6% have sight-threatening DR, such as PDR or maculopathy. By estimating the average additional healthcare costs for different severity levels of DR, our study shows the potential cost savings per patient per year of preventing development of DR. These average annual healthcare costs vary considerably with DR severity, indicating that prevention of DR progression may reduce healthcare costs. However, in order to investigate further whether it is worth spending resources on interventions directed to DR prevention, the costs of DR must be set in relation to the effect of a specific treatment in a formal cost-effectiveness analysis. In such an analysis, we believe that the average costs of DR that have been presented in this study would constitute a good input.
Abbreviations
- BR:
-
Background retinopathy
- CDWÖ:
-
Care Data Warehouse in Östergötland
- CPP:
-
Cost per patient
- DR:
-
Diabetic retinopathy
- ICD-10:
-
International Classification of Diseases, 10th version
- NDR:
-
National Diabetes Register
- PDR:
-
Proliferative diabetic retinopathy
References
World Health Organization (2009) Diabetes: fact sheet no. 312. Available from www.who.int/mediacentre/factsheets/fs312/en/, accessed 12 March 2010
Amos AF, McCarty DJ, Zimmet P (1997) The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet Med 14(Suppl 5):S1–85
Resnikoff S, Pascolini D, Etya’ale D et al (2004) Global data on visual impairment in the year 2002. Bull World Health Org 82:844–851
Klein R, Klein BE, Moss SE, Davis MD, DeMets DL (1984) The Wisconsin epidemiologic study of diabetic retinopathy. II. Prevalence and risk of diabetic retinopathy when age at diagnosis is less than 30 years. Arch Ophthalmol 102:520–526
Klein R, Klein BE, Moss SE, Davis MD, DeMets DL (1984) The Wisconsin Epidemiologic Study of Diabetic Retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch Ophthalmol 102:527–532
Kohner EM, Aldington SJ, Stratton IM et al (1998) United Kingdom Prospective Diabetes Study, 30: diabetic retinopathy at diagnosis of non-insulin-dependent diabetes mellitus and associated risk factors. Arch Ophthalmol 116:297–303
Malone JI, Morrison AD, Pavan PR, Cuthbertson DD (2001) Prevalence and significance of retinopathy in subjects with type 1 diabetes of less than 5 years’ duration screened for the diabetes control and complications trial. Diab Care 24:522–526
Gudbjornsdottir S, Cederholm J, Eliasson B, Nilsson PM NDR 10 years, The Swedish National Diabetes Register 1996–2005, Gothenburg, Sweden
Kempen JH, O’Colmain BJ, Leske MC et al (2004) The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol 122:552–563
Candrilli SD, Davis KL, Kan HJ, Lucero MA, Rousculp MD (2007) Prevalence and the associated burden of illness of symptoms of diabetic peripheral neuropathy and diabetic retinopathy. J Diab Complications 21:306–314
Kullberg CE, Abrahamsson M, Arnqvist HJ, Finnstrom K, Ludvigsson J (2002) Prevalence of retinopathy differs with age at onset of diabetes in a population of patients with type 1 diabetes. Diabet Med 19:924–931
Williams R, Airey M, Baxter H, Forrester J, Kennedy-Martin T, Girach A (2004) Epidemiology of diabetic retinopathy and macular oedema: a systematic review. Eye (London, England) 18:963–983
Woodcock A, Bradley C, Plowright R, Ffytche T, Kennedy-Martin T, Hirsch A (2004) The influence of diabetic retinopathy on quality of life: interviews to guide the design of a condition-specific, individualised questionnaire: the RetDQoL. Patient Educ Couns 53:365–383
Rein DB, Zhang P, Wirth KE et al (2006) The economic burden of major adult visual disorders in the United States. Arch Ophthalmol 124:1754–1760
Happich M, Reitberger U, Breitscheidel L, Ulbig M, Watkins J (2008) The economic burden of diabetic retinopathy in Germany in 2002. Albrecht Von Graefes Arch Klin Exp Ophthalmol 246:151–159
National Encyclopaedia Östergötlands län. Available from www.ne.se/lang/östergötlands-län, accessed 12 May 2010
Statistics Sweden (2009) Sveriges befolkning 31 December 2008. Kommunala jämförelsetal. Available from www.scb.se/Pages/ProductTables____25795.aspx, accessed 2 November 2009
Statistics Sweden (2010) Befolkning 16-74 år efter kommun, utbildningsnivå och kön. År 1985–2009. Available from www.ssd.scb.se/databaser/makro/Produkt.asp?produktid=UF0506, accessed 12 May 2010
Wirehn AB, Karlsson HM, Carstensen JM (2007) Estimating disease prevalence using a population-based administrative healthcare database. Scand J Public Health 35:424–431
Gudbjornsdottir S, Cederholm J, Nilsson PM, Eliasson B (2003) The National Diabetes Register in Sweden: an implementation of the St. Vincent Declaration for Quality Improvement in Diabetes Care. Diabetes Care 26:1270–1276
Swedish Association of Local Authorities and Regions (SALAR) (2010) KPP—Kostnad Per Patient. Available from www.skl.se/web/KPP.aspx, accessed 12 February 2010
Wiréhn A-B (2007) A data-rich world: population-based registers in healthcare research. Department of Medicine and Health Sciences, Linköping University, Linköping
Statistics Sweden (2009) Population 31 July 2009, Quick figures. Available from www.scb.se/Pages/FigureList____4000.aspx, accessed 10 September 2009
Paulsson K, KA-S, Wadman C (2009) Hälsa på lika villkor. Resultat från Nationella folkhälsoenkäten Hälsa på lika villkor, 2008. Swedish National Institute of Public Health, Östersund
Falkenberg M, Finnstrom K (1994) Associations with retinopathy in type 2 diabetes: a population-based study in a Swedish rural area. Diabet Med 11:843–849
The National Board of Health and Welfare (2010) Nationella riktlinjer för diabetesvården Available from www.socialstyrelsen.se/nationellariktlinjerfordiabetesvarden, accessed 25 May 2010
The working group for revision of the national priority list within opthalmology (2005–2008) Prioriteringslista. Available from http://swedeye.org/foreningen/prioriteringslista, accessed 25 May 2010
The Swedish Association of Local Authorities and Regions (2009) Sjukvårdsdata i fokus. Costs per consumed DRG score year 2008. Comparison between the county of Östergötland and Sweden. Available from www.skl.se/web/Sjukvardsdata_i_fokus_1_1.aspx, accessed 11 May 2010
Tinghog G, Carlsson P, Synnerstad I, Rosdahl I (2008) Societal cost of skin cancer in Sweden in 2005. Acta Derm Venereol 88:467–473
Henricsson M, Nilsson A, Groop L, Heijl A, Janzon L (1996) Prevalence of diabetic retinopathy in relation to age at onset of the diabetes, treatment, duration and glycemic control. Acta Ophthalmol Scand 74:523–527
Reuterving CO, Kratholm J, Wachtmeister L (1999) Ophthalmic health care in diabetes mellitus: a cross-sectional study in northern Sweden. Ophthalmic Epidemiol 6:267–278
Kohner EM (2008) Microvascular disease: what does the UKPDS tell us about diabetic retinopathy? Diabet Med 25(Suppl 2):20–24
Zhang L, Krzentowski G, Albert A, Lefebvre PJ (2001) Risk of developing retinopathy in Diabetes Control and Complications Trial type 1 diabetic patients with good or poor metabolic control. Diab Care 24:1275–1279
Henricsson M, Nystrom L, Blohme G et al (2003) The incidence of retinopathy 10 years after diagnosis in young adult people with diabetes: results from the nationwide population-based Diabetes Incidence Study in Sweden (DISS). Diab Care 26:349–354
Nordwall M, Bojestig M, Arnqvist HJ, Ludvigsson J (2004) Declining incidence of severe retinopathy and persisting decrease of nephropathy in an unselected population of type 1 diabetes—the Linkoping Diabetes Complications Study. Diabetologia 47:1266–1272
Lundman B, Engstrom L (1998) Diabetes and its complications in a Swedish county. Diab Res Clin Pract 39:157–164
O’Brien JA, Patrick AR, Caro JJ (2003) Cost of managing complications resulting from type 2 diabetes mellitus in Canada. BMC Health Serv Res 3:7
Acknowledgements
The authors would like to thank Östergötland County Council and the NDR group for assistance in the extraction of data from the CDWÖ, the CPP database and the NDR. We are also grateful to C. Gylling for her excellent guidance in the registration procedure at Linköping University Hospital eye clinic.
Duality of interest
The present study was financed by AstraZeneca AB. However, the authors retained full control over the manuscript’s content and submission. B. Peebo has previously worked as a medical advisor for Pfizer and has given lectures for Novartis and Alcon. U. Rosenqvist has given lectures and worked as a consultant at pharmaceutical companies such as MSD, sanofi-aventis, Lilly, Novo Nordisk, Pfizer, AstraZeneca and Bristol-Myers Squibb. None of the authors has shares or employment in these companies.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Heintz, E., Wiréhn, AB., Peebo, B.B. et al. Prevalence and healthcare costs of diabetic retinopathy: a population-based register study in Sweden. Diabetologia 53, 2147–2154 (2010). https://doi.org/10.1007/s00125-010-1836-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-010-1836-3