
Abstract
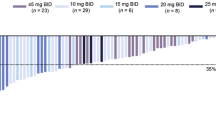
The National Institute for Health and Care Excellence (NICE) invited the manufacturer of ruxolitinib (Novartis) to submit clinical and cost-effectiveness evidence for ruxolitinib within its licensed indication (the treatment of disease-related splenomegaly or symptoms in adult patients with myelofibrosis), according to the Institute’s Single Technology Appraisal process. The Centre for Reviews and Dissemination and Centre for Health Economics at the University of York were commissioned to act as the independent Evidence Review Group (ERG). This article provides a description of the company submission, the ERG review and the resulting NICE guidance TA289 issued in June 2013. The ERG critically reviewed the evidence presented in the manufacturer’s submission and identified areas requiring clarification, for which the manufacturer provided additional evidence. The main clinical effectiveness data were derived from two phase III, multicentre, randomised controlled trials (RCTs): Controlled myelofibrosis study with oral JAK inhibitor treatment (COMFORT)-II compared ruxolitinib with best available therapy (BAT), and COMFORT-I compared ruxolitinib with placebo. These RCTs demonstrated that ruxolitinib confers significant benefits in terms of spleen size reduction and improvement in symptom burden. In the COMFORT-II trial, a reduction in spleen volume of ≥35 % was achieved in 28 % of ruxolitinib-treated patients compared with 0 % of patients in the BAT group (p < 0.001) at 48 weeks, and there was a mean change in spleen volume of −30.1 versus +7.3 % (p < 0.001). Ruxolitinib also provided significant improvements in myelofibrosis-associated symptoms and health-related quality-of-life compared with BAT and placebo. The ERG concluded that ruxolitinib appears to reduce splenomegaly and its associated symptoms, but that there was considerable uncertainty surrounding the manufacturer’s cost-effectiveness estimates due to limitations in the manufacturer’s model. The manufacturer’s model did not allow for disease progression, did not accurately capture symptomatic relief, had several implausible or unjustified assumptions, and there were several parameter choices that the ERG found sub-optimal. ERG sensitivity analyses found that nearly all plausible adjustments to the model reduced the cost effectiveness of ruxolitinib. It is very likely that the base-case incremental cost-effectiveness ratio of £73,980/quality-adjusted life-year presented by the manufacturer represents a best-case scenario. The NICE Appraisal Committee concluded that ruxolitinib was clinically effective, but could not be considered a cost effective use of National Health Service (NHS) resources for treating disease-related splenomegaly or symptoms in adults with myelofibrosis. Ruxolitinib is not recommended for the treatment of disease-related splenomegaly or symptoms in adult patients with primary myelofibrosis (also known as chronic idiopathic myelofibrosis), post-polycythaemia vera myelofibrosis and post-essential thrombocythaemia myelofibrosis in NICE TA289.
Similar content being viewed by others


References
National Institute for Health and Clinical Excellence. Guide to the single technology appraisal (STA) process. London: NICE; 2006.
Craig D, et al. Ruxolitinib for the treatment of myelofibrosis. Southampton: Health Technology Assessment Programme; 2012.
Craig D, et al. Retigabine for the adjunctive treatment of adults with partial-onset seizures in epilepsy with and without secondary generalization. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31:101–10.
Kearns B, et al. Cabazitaxel for the second-line treatment of metastatic hormone refractory prostate cancer. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31:479–88.
Tosh J, et al. Golimumab for the treatment of rheumatoid arthritis after the failure of previous disease-modifying anti-rheumatic drugs. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31:653–61.
Armstrong N, et al. Golimumab for the treatment of ankylosing spondylitis. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31:415–25.
Greenhalgh J, et al. Rituximab for the firstline maintenance treatment of follicular non-Hodgkin’s lymphoma. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31:403–13.
Simpson EL, et al. Bivalirudin for the treatment of ST-segment elevation myocardial infarction. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31(4):269–75.
Rafia R, et al. Trabectedin for the treatment of advanced metastatic soft tissue sarcoma. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31:471–8.
Spackman E, et al. Trastuzumab for the treatment of HER2 positive metastatic gastric cancer. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31(3):185–94.
Kilonzo M, Hislop J, Elders A. Pazopanib for the first-line treatment of patients with advanced and/or metastatic renal cell carcinoma. A NICE Single Technology Appraisal. Pharmacoeconomics. 2013;31(1):15–24.
Sculpher M. Single technology appraisal at the UK National Institute for Health and Clinical Excellence: a source of evidence and analysis for decision making internationally. Pharmacoeconomics. 2010;28(5):347–9.
Dickson R, et al. Erlotinib monotherapy for the maintenance treatment of non-small cell lung cancer after previous platinum-containing chemotherapy. A NICE Single Technology Appraisal. Pharmacoeconomics. 2011;29(12):1051–62.
Scotland G, et al. Denosumab for the prevention of osteoporotic fractures in post-menopausal women. A NICE Single Technology Appraisal. Pharmacoeconomics. 2011;29(11):951–61.
Stevenson M, Pandor A. Febuxostat for the management of hyperuricaemia in patients with gout. A NICE Single Technology Appraisal. Pharmacoeconomics. 2011;29(2):133–40.
McKenna C, et al. Dronedarone for the treatment of atrial fibrillation. A NICE Single Technology Appraisal. Pharmacoeconomics. 2012;30(1):35–46.
Holmes M, Carroll C, Papaioannou D. Dabigatran etexilate for the prevention of venous thromboembolism in patients undergoing elective hip or knee surgery. A NICE Single Technology Appraisal. Pharmacoeconomics. 2012;30(2):137–46.
Yang HQ, et al. Golimumab for the treatment of psoriatic arthritis. A NICE Single Technology Appraisal. Pharmacoeconomics. 2012;30(4):257–70.
Boyers D, et al. Eltrombopag for the treatment of chronic immune or idiopathic thrombocytopenic purpura. A NICE Single Technology Appraisal. Pharmacoeconomics. 2012;30(6):483–95.
Burch J, et al. Omalizumab for the treatment of severe persistent allergic asthma in children aged 6–11 years. A NICE Single Technology Appraisal. Pharmacoeconomics. 2012;30(11):991–1004.
Whyte S, Pandor A, Stevenson M. Bevacizumab for metastatic colorectal cancer. A NICE Single Technology Appraisal. Pharmacoeconomics. 2012;30(12):1119–32.
Bagust A, et al. Cetuximab for recurrent and/or metastatic squamous cell carcinoma of the head and neck/A NICE Single Technology Appraisal. Pharmacoeconomics. 2010;28(6):439–48.
Rodgers M, et al. Alitretinoin for severe chronic hand eczema. A NICE Single Technology Appraisal. Pharmacoeconomics. 2010;28(5):351–62.
National Institute for Health and Clinical Excellence. Myelofibrosis (splenomegaly, symptoms)—ruxolitinib [ID510]. 2013 (cited 2013 February). http://guidance.nice.org.uk/TA/Wave0/615.
Girodon F, et al. Significant increase in the apparent incidence of essential thrombocythemia related to new WHO diagnostic criteria: a population-based study. Haematologica. 2009;94(6):865–9.
McNally RJ, et al. Age and sex distributions of hematological malignancies in the U.K. Hematol Oncol. 1997;15(4):173–89.
Phekoo KJ, et al. The incidence and outcome of myeloid malignancies in 2,112 adult patients in southeast England. Haematologica. 2006;91(10):1400–4.
Orphanet. Prevalence of rare diseases: bibliographic data, Paris; 2012. p. 30.
European Medicines Agency (EMA) and Committee for Orphan Medicinal Products. In: Public summary of opinion on orphan designation. (R)-3-(4-(7H-pyrrolo[2,3-d]pyrimidin-4-yl)-1H-pyrazol-1-yl)-3-cyclopentylpropanenitrile phosphate for the treatment of myelofibrosis secondary to polycythaemia vera or essential thrombocythaemia. London: European Medicines Agency; 2011. p. 5.
Novartis. Single Technology Appraisal (STA): Ruxolitinib (Jakavi) for the treatment of primary myelofibrosis, post-polycythaemia vera myelofibrosis and post-essential thrombocythaemia myelofibrosis. Manufacturer’s submission. 2012. p. 294.
Harrison C, et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N Engl J Med. 2012;366(9):787–98.
Verstovsek S, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799–807.
National Institute for Health and Clinical Excellence (NICE). Final scope for the proposed appraisal of ruxolitinib for the treatment of myelofibrosis. London: National Institute for Health and Clinical Excellence; 2012.
Committee for Medicinal Products for Human Use (CHMP). CHMP assessment report: Jakavi Ruxolitinib. EMA/465846/2012. 2012 (cited 2012). http://www.emea.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002464/WC500133226.pdf.
Verstovsek S, et al. Safety and efficacy of INCB018424, a JAK1 and JAK2 inhibitor, in myelofibrosis. N Engl J Med. 2010;363(12):1117–27.
Harrison CN, et al. Results of a randomized study of the JAK inhibitor ruxolitinib (INC424) versus best available therapy (BAT) in primary myelofibrosis (PMF), post-polycythemia vera-myelofibrosis (PPV-MF) or post-essential thrombocythemia-myelofibrosis (PET-MF). J Clin Oncol. 2011;29(18 Suppl. 1):LBA6501.
Verstovsek S, et al. Long-term outcome of Ruxolitinib treatment in patients with Myelofibrosis: durable reductions in spleen volume, improvements in quality of life, and overall survival advantage in COMFORT-I. Abstract Number 800, in 54th ASH Annual Meeting, Atlanta, 2012.
Cervantes F., et al. Long-term safety, efficacy, and survival findings from COMFORT-II, a phase 3 study comparing ruxolitinib with best available therapy (BAT) for the treatment of myelofibrosis (MF). Abstract Number 801, in 54th ASH Annual Meeting, Atlanta, 2012.
Verstovsek S, et al. A phase I/II study of INCB018424, an oral, selective JAK inhibitor, in patients with primary myelofibrosis (PMF) and post polycythemia vera/essential thrombocythemia myelofibrosis (Post-PV/ET MF). J Clin Oncol. 2008;26(15):7004.
Cervantes F, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113(13):2895–901.
National Institute for Health and Clinical Excellence (NICE). Eribulin for the treatment of advanced metastatic breast cancer (TA250). London: National Institute for Health and Clinical Excellence; 2012. p. 67.
Roskell NS, et al. Using a condition-specific measure of patient-reported outcomes to derive utilities in myelofibrosis. In: ISPOR 17th annual international meeting, Washington, DC, 2012.
Roskell NS, et al. Using a condition-specific measure of patient-reported outcomes to derive utilities in myelofibrosis. Value Health. 2012;15(4):A224–5.
National Institute for Health and Clinical Excellence. Guide to the methods of technology appraisal. London: NICE; 2008. p. 76.
Tefferi A, et al. International Working Group (IWG) consensus criteria for treatment response in myelofibrosis with myeloid metaplasia, for the IWG for Myelofibrosis Research and Treatment (IWG-MRT). Blood. 2006;108(5):1497–503.
National Institute for Health and Care Excellence. Ruxolitinib for disease-related splenomegaly or symptoms in adults with myelofibrosis. Appraisal consultation document (ACD). 2013 (cited 2013 April 29). http://guidance.nice.org.uk/TA/Wave0/615/Consultation/DraftGuidance.
Verstovsek S, et al. The MD Anderson Cancer Center (MDACC) experience with ruxolitinib, an oral JAK1 and JAK2 inhibitor, in myelofibrosis: long-term follow-up outcomes of 107 patients from a phase I/II study. Blood. 2011;118(21):1646.
Tefferi A, Pardanani A. Serious adverse events during ruxolitinib treatment discontinuation in patients with myelofibrosis. Mayo Clin Proc. 2011;86(12):1188–91.
National Institute for Health and Care Excellence. Final appraisal determination: Ruxolitinib for disease-related splenomegaly or symptoms in adults with myelofibrosis. 2013 (cited 2013 April 29). http://www.nice.org.uk/nicemedia/live/13687/63722/63722.pdf.
Acknowledgments
This project was funded by the National Institute for Health Research (NIHR) Health Technology Assessment (HTA) Programme (project number 11/79/01) and will be published as part of a compendium of ERG articles in Health Technology Assessment. See the HTA programme website (http://www.hta.ac.uk) for further project information. This summary of the ERG report was compiled after the Appraisal Committee’s review and incorporates additional information and comment from the authors on the STA process and iterations of the NICE guidance not covered by the HTA report.
The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the NICE or the Department of Health. The authors would like to thank Professor Stephen Palmer, Centre for Health Economics, for providing advice throughout the project.
This work is Crown copyright (UK).
Author contributions
Ros Wade reviewed the clinical evidence submitted and wrote most sections of the manuscript.
Micah Rose reviewed the cost-effectiveness evidence submitted and wrote the cost-effectiveness sections of the manuscript.
Aileen Rae Neilson reviewed the cost-effectiveness evidence submitted and provided comments on drafts of the manuscript.
Lisa Stirk reviewed the search strategies and provided comments on drafts of the manuscript.
Rocio Rodriguez-Lopez reviewed the search strategies and provided comments on drafts of the manuscript.
David Bowen provided clinical advice throughout the project and comments on drafts of the manuscript. In terms of conflicts of interest, Professor David Bowen has received payments from Novartis, although not directly related to ruxolitinib. He attended a Novartis UK Advisory Board in 2011 to discuss the management of myeloproliferative disease and the position of ruxolitinib within the current agents used. In addition he works closely with Novartis in other areas and has the following relationships with them: member of Trial Steering Committee for a global commercial phase III study (TELESTO) for which he is paid per hour; co-chair of SC for EUMDS Registry programme, an academic study funded by Novartis via the University of Nijmegen and for which no direct funding is received by Professor Bowen personally. In addition, he has attended Advisory Boards for various agents, for which he is paid honoraria.
Dawn Craig took responsibility for the cost-effectiveness evidence appraisal and contributed to all aspects of the review of the evidence submitted and provided comments on drafts of the manuscript.
Nerys Woolacott took overall managerial responsibility for the project, contributed to all aspects of the review of the evidence submitted and provided comments on drafts of the manuscript.
Ros Wade, Micah Rose, Aileen Rae Neilson, Lisa Stirk, Rocio Rodriguez-Lopez, Dawn Craig and Nerys Woolacott have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wade, R., Rose, M., Neilson, A.R. et al. Ruxolitinib for the Treatment of Myelofibrosis: A NICE Single Technology Appraisal. PharmacoEconomics 31, 841–852 (2013). https://doi.org/10.1007/s40273-013-0083-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40273-013-0083-0