
Abstract
Background
Patients with cancer in the United States are estimated to have a suicide incidence that is approximately twice that of the general population. Patients with bone and soft tissue cancer often have physical impairments and activity limitations develop that reduce their quality of life, which may put them at high risk for depression, anxiety, and suicidal ideation. To our knowledge, there have been no large studies determining incidence of suicide among patients with bone and soft tissue cancer; this information might allow screening of certain high-risk groups.
Questions/Purposes
To determine (1) the incidence of suicide in patients with bone and soft tissue cancer, (2) whether the incidence of suicide is greater in patients with bone and soft tissue cancer than it is in the general US population, and (3) any demographic and tumor characteristics associated with increased suicide incidence.
Methods
A retrospective analysis of the Surveillance, Epidemiology, and End Results (SEER) program was performed. A total of 23,620 patients with primary bone and soft tissue cancer were identified in this database from 1973 and 2013. Patients with a cause of death listed as “suicide and self-inflicted injury” were considered to have committed suicide and suicide incidences were determined for different demographic and tumor characteristics in this subset of patients. Patient data for age, gender, race, marital status, year of diagnosis, primary cancer site, cancer stage, course of treatment, and survival time were collected and analyzed. The incidence of suicide in patients with bone and soft tissue sarcoma was compared with the age-, gender-, and race-adjusted incidence of suicide in the general US population from 1970 to 2013 available from the National Center for Health Statistics through the SEER Program.
Results
The overall suicide incidence in this population was 32 per 100,000 person-years, which was higher than the age-, race-, and gender-adjusted US general population suicide incidence of 13 per 100,000 person-years. When compared with the incidence of suicide in matched subgroups of the general US population, a higher suicide incidence was observed in men (standardized mortality ratio [SMR], 2.49; 95% CI, 1.92–3.22; p < 0.001), patients of white race (SMR, 2.68; 95% CI, 1.94–3.56; p < 0.001), patients 21 to 30 years old (SMR, 4.40; 95% CI, 3.44–5.54; p < 0.001) and 61 to 70 years old (SMR, 3.27; 95% CI, 2.54–4.18; p < 0.001), patients with cancer of the vertebral column (SMR, 2.88; 95% CI, 2.13–3.83; p < 0.001) and pelvic bones (SMR, 2.75; 95% CI, 2.00–3.65; p < 0.001), and patients within the first 5 years of cancer diagnosis (SMR, 10.8; 95% CI, 9.19–12.61; p < 0.001).
Conclusions
With identification of these characteristics that are associated with higher incidence of suicide, physicians should consider screening patients possessing these traits. By identifying at-risk patients, we can hope to reduce the incidence of suicide in this population by providing the treatment that these patients need. Further research must be done to determine how best to screen these patients and to identify the best interventions to reduce suicide incidence.
Level of Evidence
Level III, prognostic study.
Similar content being viewed by others


Introduction
Suicide is the 10th leading cause of death in the United States (US), and the incidence of suicide among patients with cancer is even higher [12, 21]. Some studies have estimated the suicide incidence for all patients with cancer to be approximately twice that of the general US population [3, 17]. Despite advancements in cancer therapy that have increased survival times, cancer is a multidimensional disease and there are various other factors that physicians must address when caring for these patients. Many of these factors may increase a patient’s likelihood of suicide including the psychosocial and psychosomatic effects of their illness, pain, side effects of treatment, and preexisting psychologic conditions [4, 7, 24]. Misono et al. [17] examined the Surveillance, Epidemiology, and End Results (SEER) database to determine the suicide incidence in persons with all types of cancer from 1973 to 2002. They found that higher suicide incidences were observed in men and patients of white race, and that suicide incidence was highest during the first 5 years after diagnosis.
To our knowledge, there has been no large, comprehensive study of suicide among patients with bone and soft tissue cancer. Other studies that have examined the incidence of suicide in patients with cancer have not isolated bone and soft tissue cancer among the cancer subtypes they examined [3, 17, 21]. Bone and soft tissue cancer poses different challenges to the patient that are not seen in many other malignancies such as changes in gait, function, stability, strength, and appearance [9, 10, 22]. These changes can make it difficult for patients to resume their precancer lives, which can produce psychologic sequelae for years after remission is achieved [9, 10, 22, 23, 27]. Additionally, high levels of depression and demoralization have been shown in patients with bone and soft tissue cancer [20, 23, 27]. These psychologic changes are widely known to increase suicide risk [4, 7, 24]. We were concerned that the number of adverse effects related to diagnosis and treatment of bone and soft tissue cancer may be associated with greater incidence of suicide in this population compared with the general US population and the population with cancer as a whole. These are important gaps in knowledge, as this information might allow future screening of certain high-risk groups.
We therefore wished to determine (1) the incidence of suicide in patients with bone and soft tissue cancer, (2) whether the incidence of suicide is greater in patients with bone and soft tissue cancer than it is in the general US population, and (3) any demographic and tumor characteristics associated with increased suicide incidence.
Patients and Methods
We used the SEER database, which is a national cancer database created by the National Cancer Institute [18]. The most recent version consists of data from 18 regionally diverse population-based cancer registries from throughout the United States from 1973 to 2013. There are 10 state registries, five metropolitan area registries, and three Native American registries. These registries cover approximately 28% of the US population and the followup rate among patients entered in the database through 2013 is approximately 90% [18]. Each registry has a contractual obligation to meet specific data-quality goals and the SEER Program has an extensive set of field edits to prevent and correct data errors [18].
All patients with a primary bone or soft tissue tumor were abstracted at the beginning of this study. Patients were classified into eight subgroups according to their primary cancer sites using the “primary site-labeled” variable in the SEER Program, which included: upper limb (long bones: upper limb, scapula, and associated joints; short bones of upper limb and associated joints); lower limb (long bones of lower limb and associated joints; short bones of lower limb and associated joints); skull and face (bones of skull and face and associated joints); vertebral column; rib, sternum, and clavicle (and associated joints); pelvic bones (pelvic bones, sacrum, coccyx, and associated joints); spinal cord; and other (bone, not otherwise specified).
Patient data for age, gender, race, marital status at diagnosis, primary cancer site, year of diagnosis, cause of death, cancer stage, treatment course (radiation only, surgery only, both, or neither), survival time, and status of followup were obtained from the SEER registries. Patients with a cause of death of “suicide and self-inflicted injury” were considered to have committed suicide. Cancer staging was performed using the 6th and 7th editions of the American Joint Commission on Cancer’s Cancer Staging Manual [2]. Stage was classified as localized (N0M0), regional (N+), distant (M1), or unknown (blank). Patients encoded in the SEER database with a survival time of 0 were recoded to have a survival time of ½ month in compliance with accepted epidemiologic practices [15]. Data analyses were performed in 2016.
This study did not involve the use of human participants or access to personal identifying information, therefore approval by an institutional review board was not required.
Statistical analysis was performed using SAS® statistical software, Version 9.3 (SAS Institute, Inc, Cary, NC, USA), and Microsoft® Excel® (Microsoft Corp, Redmond, WA, USA). Patient survival times and suicide incidences were compared with the US general population mortality data from 1970 to 2013, which was available from the National Center for Health Statistics of the US Census Bureau through the SEER Program [28]. Incidence comparisons were made based on different demographic and tumor characteristics including age, gender, and primary cancer site. Suicide incidences per 100,000 person-years were calculated by dividing the number of suicides in each categorical subset by the total survival time, in person-years, accumulated by patients in that subset. Standardized mortality ratios (SMR) were calculated with 95% CIs by determining the ratio of suicides in the population with bone and soft tissue cancer to suicides in the general US population. The overall suicide incidence in the population with cancer was compared with an age-, gender-, and race-adjusted incidence in the US general population. Additionally, incidences among subgroups of the population with cancer were compared with incidences in matched subpopulations of the US general population for age, gender, and race. All other characteristics including cancer site, year of diagnosis, cancer stage, treatment modality, and time since diagnosis were compared with the incidence of suicide in the age-, gender-, and race-adjusted US general population. SMRs with a p value less than 0.05 were considered statistically significant.
Results
Incidence of Suicide Among Patients With Cancer
Fifty-two suicides were identified among 23,620 patients with bone and soft tissue cancer observed for 164,455 person-years, producing a suicide incidence of 32 per 100,000 person-years.
Comparison of Patients With Cancer and the US Population
The incidence of suicide among patients with bone and soft tissue cancer was greater than that of the US general population. The age-, gender-, and race-adjusted suicide incidence in the US general population during the same period was 13 per 100,000 person-years. The SMR among patients with bone and soft tissue cancer was 2.43 (95% CI, 1.74–3.29; p < 0.001) compared with the matched US general population.
Characteristics Associated With Increased Suicide Incidence
Demographic Characteristics
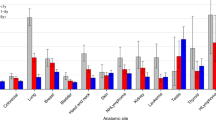
Men (SMR, 2.49; 95% CI, 1.92–3.22; p < 0.001) and patients of white race (SMR, 2.68; 95% CI, 1.94–3.56; p < 0.001) had higher suicide incidences than their matched counterparts in the US general population (Table 1). Patients in all age groups except the 40- to 50-year-old age group had higher suicide incidences than people in the same age groups in the US general population (Fig. 1). Patients 21 to 30 years old (SMR, 4.40; 95% CI, 3.44–5.54; p < 0.001) had the highest incidence of suicide followed by patients 61 to 70 years old (SMR, 3.27; 95% CI, 2.54–4.18; p < 0.001). Additionally, patients who received neither radiation nor surgery (SMR, 3.38; 95% CI, 2.59–4.45; p < 0.001) had the highest suicide incidence of all other patients with known treatment regimens when compared with the age-, gender-, and race-adjusted suicide incidence of the US general population. Marital status provided no conclusive evidence that any one characteristic in this category was more highly associated with increased suicide incidence. Additionally, we could not draw any inferences regarding the association of disease status at diagnosis with suicide, as almost 70% of the data on disease status at diagnosis were missing.

The graph shows the standardized mortality ratios with 95% CIs for patients with bone and soft tissue cancer by age at diagnosis. Reference population is the general US population in corresponding age groups. *Age group deemed to have a suicide incidence that was statistically different from the reference population with a p value less than 0.05.
Primary Cancer Site
Patients with bone and soft tissue tumors at all analyzed sites except for rib, sternum, and clavicle had higher suicide incidences than the US general population (Table 2). The highest incidences were recorded among patients with cancer of the vertebral column (38 per 100,000 person-years; SMR, 2.89; 95% CI, 2.13–3.83; p < 0.001), pelvic bones (36 per 100,000 person-years; SMR, 2.75; 95% CI, 2.00–3.65; p < 0.001), and spinal cord (34 per 100,000 person-years; SMR, 2.62; 95% CI, 1.87–3.47; p < 0.001).
Time Since Diagnosis
Suicide incidence was only significantly higher than the age-, gender-, and race-adjusted incidence in the US general population within the first 5 years of cancer diagnosis (SMR, 10.75; 95% CI, 9.19–12.61; p < 0.001) (Table 3).
Discussion
The incidence of suicide in the population with cancer is known to be approximately twice that of the general US population [3, 17]. Given the high levels of depression and demoralization in patients with bone and soft tissue cancer [20, 23, 24, 27] and the changes in gait, function, and strength after treatment of these malignancies [9, 10, 22], suicide incidence among these patients may be higher than that of the entire cancer population. However, most of the previous studies on suicide incidence in patients with cancer excluded patients with bone and soft tissue cancer or did not highlight them as a subgroup [3, 14, 17]. Therefore, we examined the suicide incidence in the population with bone and soft tissue cancer, compared that incidence with the suicide incidence in the general US population, and determined what factors were associated with higher suicide incidence. Higher suicide incidences were seen in men, patients of white race, patients who had cancer of the pelvis or vertebral column, and patients within the first 5 years of diagnosis.
The limitations to this study are inherent to large retrospective databases such as the SEER registries. First, suicide as a cause of death may be over- or underreported in the SEER database owing to errors in coding. However, given the extensive set of field edits that the SEER database goes through on a regular basis to prevent and correct data errors, these errors are likely to be rare [18]. Second, comorbidities such as substance abuse and preexisting depression or psychiatric illness are not available in the SEER registries. Given that the diagnosis of depression is relatively common in the population with these forms of cancer [20, 23, 27], this presents an important area for future research on this topic as depression is highly correlated to suicidal incidence [4, 7, 24]. Staging for bone cancer was unavailable for most patients in the way that it was coded in the SEER program, therefore we were unable to discern whether disease extent was associated with suicide incidence.
Additionally, there is no way to determine whether the patient had no evidence of disease, local recurrence, or metastasis at followup. Therefore, it cannot be determined whether these recurrences, which likely indicate worse prognosis, were associated with higher suicide incidences. Other studies have shown that more advanced disease was associated with greater suicide incidence [17, 21] and therefore with more available data, our study might have shown similar trends. Moreover, the use of chemotherapy is not reported by the SEER database and thus the association of this treatment cannot be assessed in this dataset. Chemotherapy is used in the treatment of some bone and soft tissue tumors and therefore, knowledge of the use of this treatment modality may have offered insight into whether the patients in this study who were coded to have not received radiation or surgery in fact received no treatment or they received only chemotherapy. Patients who truly receive no treatment often have the worst prognosis and therefore, the incidence of suicide in this population may have been even higher owing to the previously stated prevalence of higher incidence of suicide in patients with poor prognoses. Finally, the number of events analyzed was insufficient to separate bone from soft tissue sarcomas in terms of their association with suicide, and this might have been interesting to do because patients with sarcomas of bone often undergo more extensive surgical resections than do patients with soft tissue sarcomas. Along a similar line, it is possible that confounding variables may have influenced our results (for instance, there may have been more women in the older patient demographics, and it was not possible to tease out whether the observed association was driven more by age or gender). Multivariate analysis was not performed to assess for these confounders and therefore future studies might consider these associations.
The suicide incidence in the population with bone and soft tissue cancer was more than twice that of the general US population. A study of the suicide incidence among all patients with cancer showed that the incidence was approximately 1.9 times that of the general US population [17]. Compared with subpopulations examined in other studies, the suicide incidence of patients with bone and soft tissue cancer ranked below the incidence of suicide in patients with cancer of the lung and bronchus, stomach, oral cavity and pharynx, larynx, and ovary [17]. If bone and soft tissue cancer were examined in that previous study, it would rank fifth in terms of suicide incidence. The patients with cancers that rank above it have very poor prognoses, high rates of depression, and their own set of life-altering consequences of treatment [13, 17].
Men had a higher incidence of suicide than did women in our study. This is in concordance with the trends in the general population and those of the population with cancer [13]. Kendal [14] analyzed the SEER registries from 1973 to 2001 and found a hazard ratio for suicides in men relative to suicides in women of 6.2. Nock et al. [19] examined nonfatal self-injury rates from 1997 to 2007 and determined that rates were higher in women, but the suicide incidence among men was higher. This trend often is attributed to the more lethal and violent suicidal methods used by men compared with women [11]. It therefore is possible that women with bone and soft tissue cancer who attempt suicide are underrepresented because the SEER database does not record unsuccessful suicide attempts. Additionally, the incidence of suicide was highest in patients of white race and lowest in patients of black race. This is reflective of trends in the US population as a whole. The incidence of suicide in people of white race, black race, and other is 13 per 100,000 person-years, six per 100,000 person-years, and eight per 100,000 person-years, respectively [28]. Suicide incidences were highest in patients 21 to 30 years old and 61 to 70 years old. Some studies have reported an increased incidence of suicide in elderly patients with cancer [3, 6]. Cole et al. [6] analyzed 334 suicides of patients with cancer who were older than 65 years in North Carolina. Patients who successfully committed suicide were more likely to be white men older than 71 years.
Patients with cancer of the vertebral column and the pelvis also had a higher incidence of suicide. Compared with tumors of other sites, pelvic and vertebral sarcomas have a worse prognosis likely attributable to delayed diagnosis, more complicated resections, and higher recurrence rates although we could not analyze complications and recurrences because these data are not available in the SEER database. The symptoms associated with these tumors also can have an important effect on the lives of the patients. Spinal tumors are associated with pain, limb weakness and numbness, and loss of bowel control [5]. Yin et al. [29] reported 98 cases of spinal chondrosarcoma with a recurrence rate of 43% and mortality rate of 33% during a mean followup of 49.7 months. Farfalli et al. [8] analyzed the outcomes of 52 patients with primary pelvic sarcomas and reported a 5-year survival of 37.5% and a local recurrence rate of 30%. This poor outlook combined with the symptomology of the disease and the extensive resections involved in treating these sarcomas can take a toll on patients’ quality of life and psychologic health. The incidence of suicide was highest during the first 5 years after diagnosis. Ahn et al. [1] reported that 40% of suicides in their cohort of 164,497 Korean patients with cancer occurred during the first year after diagnosis. These high initial incidences are likely the result of difficulty dealing with the cancer diagnosis.
Depression, distress, and anxiety are frequently observed in the population with sarcoma [20, 23, 27]. Patients with the characteristics identified in our study as having increased incidence of suicide should be screened for depression, distress, and suicidal ideation as there is a high correlation between these neuropsychologic diagnoses and completed suicide [4, 7, 24]. Despite that suicide may be an uncomfortable topic of discussion for physicians practicing outside the mental health field, Trevino et al. [25] reported fewer suicidal ideations in patients with advanced cancer who had strong therapeutic alliances with their oncologists. Leung et al. [16] had success using the Distress Assessment and Response Tool (DART) to identify suicidal ideation and suicidal intention in patients with cancer. The use of tools such as the DART can help healthcare professionals identify patients at high risk for suicide early during the treatment process. On discovery of a patient’s suicidal ideations or actions, physicians often provide referrals to mental health professionals. However, patients often fail to attend these referral appointments rendering this technique inadequate at preventing suicide [26]. Therefore, it may be the physicians treating these patients for cancer who can have the largest effect on preventing suicide.
Patients with bone and soft tissue cancer have a higher incidence of suicide than the general US population. Specifically, patients with cancer of the vertebral column and pelvis have the highest incidence. Additionally, patients who are men or of white race also showed an increased incidence of suicide after receiving a diagnosis of bone or soft tissue cancer. Physicians should consider screening patients with these characteristics throughout the cancer treatment process and beyond for suicidal thoughts or actions to prevent suicides and identify those most in need of mental health treatment. Future research is needed to further assess the psychologic ramifications of cancer diagnosis, treatment, and persisting morbidity and how best to treat these effects clinically. Additionally, research is needed to fill the gaps that this study lacks owing to limitations of the SEER database including the association of cancer stage, complication rates, and recurrence rates on the incidence of suicide in the population with bone and soft tissue cancer.
References
Ahn MH, Park S, Lee HB, Ramsey CM, Na R, Kim SO, Kim JE, Yoon S, Hong JP. Suicide in cancer patients within the first year of diagnosis. Psychooncology. 2015;24:601–607.
American Joint Committee on Cancer. The AJCC Cancer Staging Manual. Available at: https://cancerstaging.org/references-tools/deskreferences/Pages/default.aspx. Accessed October 26, 2016.
Anguiano L, Mayer DK, Piven ML, Rosenstein D. A literature review of suicide in cancer patients. Cancer Nurs. 2012;35:E14–26.
Balci Sengul MC, Kaya V, Sen CA, Kaya K. Association between suicidal ideation and behavior, and depression, anxiety, and perceived social support in cancer patients. Med Sci Monit. 2014;20:329–336.
Bhatia R, Beckles V, Fox Z, Tirabosco R, Rezajooi K, Casey AT. Osteosarcoma of the spine: dismal past, any hope for the future? Br J Neurosurg. 2014;28:495–502.
Cole TB, Bowling JM, Patetta MJ, Blazer DG. Risk factors for suicide among older adults with cancer. Aging Ment Health. 2014;18:854–860.
Fang CK, Chang MC, Chen PJ, Lin CC, Chen GS, Lin J, Hsieh RK, Chang YF, Chen HW, Wu CL, Lin KC, Chiu YJ, Li YC. A correlational study of suicidal ideation with psychological distress, depression, and demoralization in patients with cancer. Support Care Cancer. 2014;22:3165–3174.
Farfalli GL, Albergo JI, Ritacco LE, Ayerza MA, Muscolo DL, Aponte-Tinao LA. Oncologic and clinical outcomes in pelvic primary bone sarcomas treated with limb salvage surgery. Musculoskelet Surg. 2015;99:237–242.
Fauske L, Bruland OS, Grov EK, Bondevik H. Cured of primary bone cancer, but at what cost: a qualitative study of functional impairment and lost opportunities. Sarcoma. 2015;2015:484196. doi:10.1155/2015/484196.
Fauske L, Lorem G, Grov EK, Bondevik H. Changes in the body image of bone sarcoma survivors following surgical treatment: a qualitative study. J Surg Oncol. 2016;113:229–234.
Fisher LB, Overholser JC, Dieter L. Methods of committing suicide among 2,347 people in Ohio. Death Stud. 2015;39:39–43.
Heron M. Deaths: leading causes for 2013. National Vital Statistics Reports. 2016;65. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_02.pdf. Accessed September 20, 2016.
Kam D, Salib A, Gorgy G, Patel TD, Carniol ET, Eloy JA, Baredes S, Park RC. Incidence of suicide in patients with head and neck cancer. JAMA Otolaryngol Head Neck Surg. 2015;141:1075–1081.
Kendal WS. Suicide and cancer: a gender-comparative study. Ann Oncol. 2007;18:381–387.
Koepsell TD, Weiss NS. Epidemiologic Methods: Studying the Occurrence of Illness. New York, NY: Oxford University Press; 2003.
Leung YW, Li M, Devins G, Zimmermann C, Rydall A, Lo C, Rodin G. Routine screening for suicidal intention in patients with cancer. Psychooncology. 2013;22:2537–2545.
Misono S, Weiss NS, Fann JR, Redman M, Yueh B. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731–4738.
NIH National Cancer Institute. Overview of the SEER Program. Available at: http://seer.cancer.gov/about/overview.html. Accessed July 8, 2016.
Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiol Rev. 2008;30:133–154.
Paredes T, Canavarro MC, Simoes MR. Anxiety and depression in sarcoma patients: emotional adjustment and its determinants in the different phases of disease. Eur J Oncol Nurs. 2011;15:73–79.
Robson A, Scrutton F, Wilkinson L, MacLeod F. The risk of suicide in cancer patients: a review of the literature. Psychooncology. 2010;19:1250–1258.
Schreiber D, Bell RS, Wunder JS, O’Sullivan B, Turcotte R, Masri BA, Davis AM. Evaluating function and health related quality of life in patients treated for extremity soft tissue sarcoma. Qual Life Res. 2006;15:1439–1446.
Tang MH, Castle DJ, Choong PF. Identifying the prevalence, trajectory, and determinants of psychological distress in extremity sarcoma. Sarcoma. 2015;2015:745163. doi:10.1155/2015/745163.
Tanriverdi D, Cuhadar D, Ciftci S. Does the impairment of functional life increase the probability of suicide in cancer patients? Asian Pac J Cancer Prev. 2014;15:9549–9553.
Trevino KM, Abbott CH, Fisch MJ, Friedlander RJ, Duberstein PR, Prigerson HG. Patient-oncologist alliance as protection against suicidal ideation in young adults with advanced cancer. Cancer. 2014;120:2272–2281.
Van Heeringen C, Jannes S, Buylaert W, Henderick H, De Bacquer D, Van Remoortel J. The management of non-compliance with referral to out-patient after-care among attempted suicide patients: a controlled intervention study. Psychol Med. 1995;25:963–970.
Wiener L, Battles H, Bernstein D, Long L, Derdak J, Mackall CL, Mansky PJ. Persistent psychological distress in long-term survivors of pediatric sarcoma: the experience at a single institution. Psychooncology. 2006;15:898–910.
Xu JQ, Murphy SL, Kochanek KD, Bastian BA. Deaths: final data for 2013. National Vital Statistics Reports. 2016; 64. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr64/nvsr64_02.pdf. Accessed October 27, 2016.
Yin H, Zhou W, Meng J, Zhang D, Wu Z, Wang T, Wang J, Wang P, Shi X, Wu S, Zhao J, Xiao J. Prognostic factors of patients with spinal chondrosarcoma: a retrospective analysis of 98 consecutive patients in a single center. Ann Surg Oncol. 2014;21:3572–3578.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article

Cite this article
Siracuse, B.L., Gorgy, G., Ruskin, J. et al. What is the Incidence of Suicide in Patients with Bone and Soft Tissue Cancer?. Clin Orthop Relat Res 475, 1439–1445 (2017). https://doi.org/10.1007/s11999-016-5171-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-016-5171-y