
Abstract
Background
Child abuse represents a serious threat to the health and well-being of the pediatric population. Orthopaedic specialists will often become involved when child abuse is suspected as a result of the presence of bony injury. Distinguishing abuse from accidental trauma can be difficult and is often based on clinical suspicion.
Questions/purposes
We sought to determine whether accidental femur fractures in pediatric patients younger than age 4 could be distinguished from child abuse using a combination of presumed risk factors from the history, physical examination findings, radiographic findings, and age.
Methods
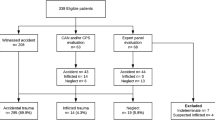
We searched our institution’s SCAN (Suspected Child Abuse and Neglect) and trauma databases. We identified 70 patients in whom the etiology of their femur fracture was abuse and compared that group with 139 patients who had a femur fracture in whom accidental trauma was the etiology.
Results
A history suspicious for abuse, physical or radiographic evidence of prior injury, and age younger than 18 months were risk factors for abuse. Patients with no risk factors had a 4% chance, patients with one risk factor had a 29% chance, patients with two risk factors had an 87% chance, and patients with all three risk factors had a 92% chance of their femur fracture being a result of abuse.
Conclusions
Clinicians can use this predictive model to guide judgment and referral to social services when seeing femur fractures in very young children in the emergency room.
Level of Evidence
Level III, diagnostic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others

Introduction
Orthopaedic surgeons play a critical role in evaluating potential cases of child abuse because fractures represent the second most common presentation of abuse behind only soft tissue injuries [23]. There are numerous studies that have focused on the characteristics of fractures considered typical of abuse, including fractures of the femur [1, 4, 5, 9, 14, 19, 28, 29], humerus [3, 12, 19, 31], tibia [4, 12, 18], and ribs [6, 33]. Yet, orthopaedic surgeons are less likely than general pediatric and emergency room colleagues to identify abuse as the potential etiology of these fractures, thus causing delay for appropriate multidisciplinary intervention [15, 26]. This is concerning because of the million children annually in the United States who are the victims of substantiated abuse, orthopaedic surgeons are often the first clinicians to evaluate these patients, and if the cause of injury is not recognized, these children will return to an abusive environment with a 50% risk for reinjury and a 10% risk of death [7, 13]. It is therefore essential orthopaedic surgeons not only treat the fractures these children present with, but also recognize the associated etiologic characteristics of the injury that may suggest child abuse.
When examining a fracture in the emergency room, the following questions should arise: What patient characteristics may be indicative of abuse versus accidental trauma? Is the history and mechanism of injury inconsistent with the presenting injury? Does this fracture type, pattern, and location represent potential abuse? Fractures of the femur in young children provide an ideal model to develop a systematic examination process to differentiate an abusive from accidental etiology.
Fracture of the femur in children is the most common musculoskeletal injury requiring hospitalization [5, 20]. Numerous studies describe fractures of the femur in young children, and many of these have attempted to identify fracture characteristics that may indicate abuse [2, 5, 8, 11, 20, 21, 24, 25, 28, 29]. The most common presentation cited is the presence of a femur fracture in a patient occurring either before walking age or before the second birthday [5, 9, 13, 20, 28, 30]. In addition, several authors have classified the radiographic appearance and location of femur fractures as predictors of abuse [2, 15, 25, 28, 29] as well as elements of the history (inconsistent history, inappropriate delay, multiple presentations), physical examination (examination inconsistent with history, head injury or fracture in a child not of walking age), and socioeconomic background [16, 22, 32]. A number of other reports previously examined fracture patterns in children younger than 48 months of age [6, 14, 16, 17, 26]. These studies do not, however, allow a clinician to decide with confidence whether a given femur fracture is likely caused by abuse.
We therefore asked whether femur fractures caused by abusive trauma could be distinguished from those caused by accidental trauma using presumed risk factors in the history, physical examination, and radiographic characteristics. We then built a predictive model based on those factors.
Materials and Methods
Our institution is a large pediatric tertiary care center with Level I trauma status with a large referral base. Institutional Review Board approval was obtained before data collection. Since 1998, we have maintained an extensive database (Suspected Child Abuse and Neglect [SCAN]) that examines all potential cases of suspected child abuse and/or neglect. This database contains information identifying child abuse victims, demographic factors, and ICD-9 and CPT codes relating to their concomitant diagnoses and treatment. From that database, we identified all children from birth to 48 months of age who had the diagnosis of child abuse (ICD-9 code 995.5x) and the diagnosis of femur fracture (ICD-9 code 820.x and 821.x). In addition, we reviewed the general trauma database from our institution for all children presenting to the emergency room and/or hospitalized with traumatic injuries for children of the same age from 2000 to 2003 with the diagnosis of femur fracture (ICD-9 code 820.x and 821.x). The general trauma database contains data identifying trauma patients that fit these characteristics, demographic information, information regarding injury diagnoses, and subsequent treatment. Information other than demographic information, injury code data and identifying information were abstracted from the electronic medical record.
We calculated a power analysis for multiple logistic regression as described by Hsieh et al. [10]. The power analysis assumes a background abuse rate of 30% [9] in patients with femur fractures in this age group with a difference in the rate in any given independent variable of 20%. The power analysis was conducted with a desired two-sided alpha of 0.05 and a desired power of 0.80. The analysis assumes a variance inflation rate (adjustment for increased variability caused by multiple regressors) of 25% for multiple regression. With these characteristics, our total sample size would need to be 196 patients. Because our analysis assumes a 30% event (abuse) [9] rate in femur fractures, we would need 30% of our total cases to be from abuse and 70% from accidental trauma (59 abuse cases and 137 accidental trauma cases).
Patients were identified in the study as a potential control (accidental) trauma case if they were found in the general trauma database and did not have a diagnosis of child abuse in their record and were not included in the SCAN database. We excluded patients from the study if they were younger than 48 months of age (except for one patient, the SCAN database contained only patients 48 months of age and younger), if we could not adequately confirm whether the case represented child abuse or accidental injury as a result of incomplete medical records (three children), and if cases were erroneously placed in either of the two databases (ie, did not represent either child abuse or accidental trauma). This was the case in one child in whom a diagnosis of femur fracture by ICD-9 code was found but no record of this injury could be identified. In addition, we excluded patients with known metabolic bone disease or osteogenesis imperfecta. Seventy femur fractures were from the child abuse cohort and 139 femur fractures were from the accidental trauma cohort. These 209 total femur fractures represented the cases and controls that would be analyzed in our study. The child abuse cohort had a median age of 4.0 months. Of these 70 patients, 63 were younger than 18 months of age and seven were older than 18 months of age. The accidental trauma cohort had a mean age of 26.2 months. Of these 139 patients, 44 were younger than 18 months of age and 95 were older than 18 months of age.
Patients were included in the SCAN database if hospital personnel determined the patient was a victim of abuse or neglect. The SCAN team consisted of an independent group of nonorthopaedic physicians, nurses, and social workers with advanced training in child abuse who examined these children independently in the emergency room and/or as inpatients and made the determination whether the patients should be diagnosed with child abuse and when child protective services should be activated. Patients were included in the general trauma database if they presented to the emergency room and/or were hospitalized with organ system trauma that necessitated an evaluation from the hospital’s trauma service, died in the emergency department as a result of their traumatic injuries, or were initially seen in the emergency department and transferred to another trauma center for management of traumatic injuries. Both databases were collected and maintained outside of the orthopaedic department at our institution and were initiated many years before the retrospective review of the data that was performed by the authors.
Data parameters collected from the patients’ medical records included age at the time of injury, gender, insurance status, presence of current polytrauma (another concurrent long bone, clavicle or axial skeletal fracture, or other body system injury that would require hospitalization), and physical and/or radiographic evidence of prior trauma. Furthermore, one of the authors (HW) who was blinded to the SCAN status of patients examined the paper and electronic medical records of the children and briefly described the history of each patient. Subsequently, this author categorized in a separate list the plausibility of each patient’s history as either suspicious for abuse (unwitnessed accident, witnessed abuse, delayed presentation greater than 48 hours, a mechanism that would not normally cause a fracture, or different stories provided by different witnesses), or consistent with accidental trauma in cases in which these criteria were not fulfilled, and then transferred the list to the database. Two other authors (NP and KB) reviewed the patient histories to determine if they were consistent with accidental trauma or suspicious for abuse. An intraclass correlation coefficient was generated based on average measures (ICC 0.902, p value < 0.001) indicating agreement. Since many of the original radiographs for patients were no longer available, we examined radiology reports to determine the location of the femur fracture in all patients. The fractures were classified as “proximal,” “diaphyseal,” or “distal” (each representing roughly one-third of the length of the femur: subtrochanteric region, shaft region, and distal metaphyseal region).
Raw data from the databases were pooled, and means, SDs, and/or percentages were calculated for age at time of injury, gender, insurance status, presence of current polytrauma, physical and/or radiographic evidence of prior trauma, history plausibility (consistent with accidental trauma or suspicious for abuse), and radiographic femur fracture location (proximal, diaphyseal, distal).
Because our age data were skewed we used the Mann Whitney U test for independent samples to determine if there was a difference in age at the time of injury between the child abuse and accidental trauma patients. The chi square test with Yates’ correction for independence or the Fisher’s exact test in cases where the assumptions of a chi square test were violated were used to determine differences in binary variables. We used binary logistic regression to calculate adjusted odds ratios for a femur fracture representing abuse as opposed to accidental trauma using age at time of injury, gender, insurance status, presence of current polytrauma, physical and/or radiographic evidence of prior trauma, history plausibility, and femur fracture location as risk factors. Ninety-five percent confidence intervals were calculated for proportions and interquartile ranges for median values.
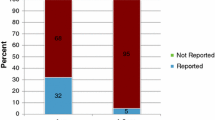
Child abuse victims were younger than accidental trauma victims (median age 4.0 months compared with 26.2 months) and were more often female (49% versus 32%) (Table 1). There was no difference (p = 0.77) between the abuse and accidental trauma groups in terms of insurance status. Patients with femur fractures who were victims of abuse had a greater frequency of current polytrauma (53% versus 8%), physical and/or radiographic evidence of prior trauma (62% versus 4%), and histories that were deemed suspicious for abuse (33% versus 4%) (Table 2). Patients with accidental trauma more often had diaphyseal femur fractures (46% versus 66%), abuse victims more often had distal femur fractures (37% versus 20%), and there was no difference in proximal femur fractures between groups (Table 3). The odds of a femur fracture being the result of abuse rather than accidental trauma was greater for children younger than 18 months (19.4 times) and patients of female gender (2.0 times) (Table 1). Furthermore, abuse was associated more frequently with current polytrauma (13.0 times), physical and/or radiographic evidence of prior trauma (37.5 times), and patients with a suspicious history (10.8 times) (Table 2).
Finally, we used a multiple logistic regression model to calculate a prediction rule for the chance of abuse given the aforementioned risk factors. All of the variables that were significant in any portion of the study were used. In addition, variables previously judged important were included in the initial multiple logistic regression model. The variables were entered using the backward likelihood ratio method for selection of variables. All variables were entered and criteria of 0.10 by the −2 log likelihood method was used for removal of variables. In the backward regression analysis, only age younger than 18 months, physical and/or radiographic evidence of prior injury, and history of plausibility were predictive of an abusive etiology for child abuse. In this model, patients with a femur fracture whose age was younger than 18 months had a 10 times greater chance of being the victim of abuse than older children. Patients who had the presence of prior trauma on physical and/or radiographic examination had a 16.8 times greater chance of having been a victim of abuse than patients who had no such findings. Finally, patients with a suspicious history had a 7.4 times greater chance of having been abused than patients with a plausible history after considering the other factors in the model.
Given these findings, a new simpler logistic regression model was built based on the outcome of the first model (Table 4). This model was built with the three significant variables in the first model. The variables entered were whether the patient had one, two, or three risk factors (risk factors from the first model: age younger than 18 months, physical and/or radiographic evidence of old trauma, and history suspicious for abuse). This final model did not differ (p = 0.69) from the old model using the −2 log likelihood method of comparison.
Results
A simple model using number of risk factors (age younger than 18 months, physical or radiographic evidence of prior injury, and suspicious history) predicted abuse in this age group. Odds ratios were calculated based on the logistic regression model versus a patient with no risk factors (Table 4).
The logistic regression equation was then solved for each number of risk factors to develop a prediction tool. In our population, patients with no risk factors had a 4% chance of having abuse as the etiology for their femur fracture, patients with one risk factor had a 24% chance abuse was the etiology of their femur fracture, patients with two risk factors had an 87% chance abuse was the etiology of their femur fracture, and patients with three risk factors had a 92% chance abuse was the etiology of their femur fracture (Fig. 1).

The figure shows our algorithm for determining whether a femur fracture stems from abuse or accidental trauma based on our regression model.
Discussion
Pediatric femur fractures are the most common musculoskeletal injury requiring hospitalization [5, 20], and their presence in children raises suspicion for abuse [2, 5, 8, 11, 20, 21, 24, 28, 29]. In fact, it has been proposed that one-third of femur fractures in children younger than age 4 years and 80% of femur fractures in children who are not yet walking have an abusive etiology [9]. Multiple studies have attempted to classify the demographic and fracture characteristics of children whose fracture may have an abusive etiology, including age (particularly before walking age or the second birthday) [5, 9, 13, 20, 28, 30], radiographic appearance and location of the fracture [2, 15, 28, 29] as well as elements of the history, physical examination, and socioeconomic background [16, 22, 32]. Because femur fractures are a common entity that the orthopaedic clinician will evaluate in the emergency room and are linked to child abuse [2, 5, 8, 11, 20, 21, 24, 28, 29], it is essential for the orthopaedic clinician to be able to differentiate an abusive from an accidental etiology so that proper multidisciplinary action can be initiated to protect children from an abusive environment. In light of this fact, and the fact that one recent investigation suggests fracture pattern may not be as useful in determining fracture etiology [29], there exists no prediction algorithm with which to help a clinician assign etiology to an injury. We presumed femur fractures resulting from accidental trauma could be differentiated from femur fractures resulting from abuse using history, physical examination, demographic factors, and radiographic findings, and a prediction model based on these parameters can be generated to allow clinicians to more accurately identify victims of abuse and distinguish abuse from accidental trauma.
There are several limitations in our study. First, our prediction rule was generated from an urban Level I pediatric trauma center. It is unclear if the prediction rule would be different for pediatric patients presenting to lower-level pediatric trauma centers in nonurban environments and/or in different countries. However, our tertiary referral status allows us to say we attract patients from a broad catchment area, hence enhancing our external validity. Second, it can be argued our assessment of history status (consistent versus suspicious) is subjective. Specifically, arguments for mitigating individual circumstances such as unwitnessed injury could be due to a momentary lapse in supervision; delay in seeking care could be due to lack of health insurance or a child who is not expressing substantial discomfort. However, our criteria for suspicion are consistent with previous reports [6, 27, 30]. In addition, although our “blinded” rater was instructed to look at only the history and physical records to determine the patient history without viewing other aspects of the medical record, she was not strictly “blind” to the SCAN status of the patient because she had access to the medical record. The use of corroborating investigators with a high intraclass correlation coefficient somewhat mitigates this risk. Third, as a result of the fact that child abuse is largely a social diagnosis, there exists no test that can confirm the presence or absence of child abuse with a high level of specificity or sensitivity. Yet, we believe evaluation by independent specialists constitutes the best method available in the current literature. Inclusion in the SCAN database is determined by an independent group of social workers, nurses, and physicians who all have advanced training in child abuse (and are independent from the authors) at the time the child presents to the emergency room, and is also used for a clinical purpose (ie, activating child protective interventions). As with any study of child abuse, the study risks circuitous logic, that is to say, child abuse is often diagnosed by “suspicious history,” physical examination findings, and other social factors. However, this could be said about any condition that is a clinical diagnosis; as such, we believe guidelines for diagnosis of this condition are helpful.
The use of age, history, physical findings, and radiographic findings to assess for child abuse is not new (Table 5). Although these multiple characteristics are essential in providing a general “picture” of a pediatric patient presenting with child abuse, the question arises as to how these characteristics can be applied in a quantifiable, objective manner to help to reliably predict etiology for a clinician. Whereas other studies have limited their analysis to descriptions of abusive and accidental femur fracture, the prediction model developed from our study allows for research to be translated into clinical action. Of the multiple demographic characteristics in our study, the multiple regression model identified the following three predictors after accounting for other confounders when differentiating abusive from accidental femur fractures in this age group: (1) age younger than 18 months; (2) physical and/or radiographic evidence of prior trauma; and (3) history suspicious for abuse. Clinicians can use this rule in the following fashion: patients with no risk factors have a 4% chance of having a femur fracture stemming from child abuse; patients with one risk factor have a 24% chance; those with two risk factors have an 87% chance; and those with three risk factors have a 92% chance of having a femur fracture stemming from abuse.
It is essential for clinicians to be able to differentiate the etiology of pediatric femur fractures as stemming from abuse or accidental trauma. Not only are femur fractures a common injury seen by orthopaedic clinicians, but identification of the etiology of the injury is vital to ensure proper multidisciplinary intervention can be initiated for the safety of the child. Prediction based on the multiple logistic regression model that was developed in our study can help determine the etiology of pediatric patients presenting with a fractured femur. Although further studies will be necessary to validate the rule prospectively, we believe the rule is a good “common sense” approach to a young patient with a femur fracture. We believe this method will help all clinicians determine whether child abuse occurred and thus enhance their approach to management.
References
Anglen JO, Choi L. Treatment options in pediatric femoral shaft fractures. J Orthop Trauma. 2005;19:724–733.
Arkader A, Friedman JE, Warner WC Jr, Wells L. Complete distal femoral metaphyseal fractures: a harbinger of child abuse before walking age. J Pediatr Orthop. 2007;27:751–753.
Caviglia H, Garrido CP, Palazzi FF, Meana NV. Pediatric fractures of the humerus. Clin Orthop Relat Res. 2005;432:49–56.
Coffey C, Haley K, Hayes J, Groner JI. The risk of child abuse in infants and toddlers with lower extremity injuries. J Pediatr Surg. 2005;40:120–123.
Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg. 2004;12:347–359.
Fong CM, Cheung HM, Lau PY. Fractures associated with non-accidental injury—an orthopaedic perspective in a local regional hospital. Hong Kong Med J. 2005;11:445–451.
Green M, Haggerty RJ. Physically Abused Children. Philadelphia PA: WB Saunders; 1968:285–289.
Greene WB. Displaced fractures of the femoral shaft in children. Unique features and therapeutic options. Clin Orthop Relat Res. 1998;353:86–96.
Gross RH, Stranger M. Causative factors responsible for femoral fractures in infants and young children. J Pediatr Orthop. 1983;3:341–343.
Hsieh FY, Bloch DA, Larsen MD. A simple method of sample size calculation for linear and logistic regression. Stat Med. 1998;17:1623–1634.
Jones JC, Feldman KW, Bruckner JD. Child abuse in infants with proximal physeal injuries of the femur. Pediatr Emerg Care. 2004;20:157–161.
King J, Diefendorf D, Apthorp J, Negrete VF, Carlson M. Analysis of 429 fractures in 189 battered children. J Pediatr Orthop. 1988;8:585–589
Kocher MS, Kasser JR. Orthopaedic aspects of child abuse. J Am Acad Orthop Surg. 2000;8:10–20.
Kowal-Vern A, Paxton TP, Ros SP, Lietz H, Fitzgerald M, Gamelli RL. Fractures in the under-3-year-old age cohort. Clin Pediatr (Phila). 1992;31:653–659.
Lane WG, Dubowitz H. What factors affect the identification and reporting of child abuse-related fractures? Clin Orthop Relat Res. 2007;461:219–225.
Lane WG, Rubin DM, Monteith R, Christian CW. Racial differences in the evaluation of pediatric fractures for physical abuse. JAMA. 2002;288:1603–1609.
Leventhal JM, Thomas SA, Rosenfield NS, Markowitz RI. Fractures in young children. Distinguishing child abuse from unintentional injuries. Am J Dis Child. 1993;147:87–92.
Loder RT, Bookout C. Fracture patterns in battered children. J Orthop Trauma. 1991;5:428–433.
Loder RT, Feinberg JR. Orthopaedic injuries in children with nonaccidental trauma: demographics and incidence from the 2000 kids’ inpatient database. J Pediatr Orthop. 2007;27:421–426.
Loder RT, O’Donnell PW, Feinberg JR. Epidemiology and mechanisms of femur fractures in children. J Pediatr Orthop. 2006;26:561–566.
Lynch JM, Gardner MJ, Gains B. Hemodynamic significance of pediatric femur fractures. J Pediatr Surg. 1996;31:1358–1361.
McKinney A, Lane G, Hickey F. Detection of non-accidental injuries presenting at emergency departments. Emerg Med J. 2004;21:562–564.
McMahon P, Grossman W, Gaffney M, Stanitski C. Soft-tissue injury as an indication of child abuse. J Bone Joint Surg Am. 1995;77:1179–1183.
Nafei A, Teichert G, Mikkelsen SS, Hvid I. Femoral shaft fractures in children: an epidemiological study in a Danish urban population, 1977–86. J Pediatr Orthop. 1992;12:499–502.
O’Connor-Read L, Teh J, Willett K. Radiographic evidence to help predict the mechanism of injury of pediatric spiral fractures in nonaccidental injury. J Pediatr Orthop. 2007;27:754–757.
Oral R, Blum KL, Johnson C. Fractures in young children: are physicians in the emergency department and orthopedic clinics adequately screening for possible abuse? Pediatr Emerg Care. 2003;19:148–153.
Pierce MC, Bertocci GE, Janosky JE, Aguel F, Deemer E, Moreland M, Boal DK, Garcia S, Herr S, Zuckerbraun N, Vogeley E. Femur fractures resulting from stair falls among children: an injury plausibility model. Pediatrics. 2005;115:1712–1722.
Rex C, Kay PR. Features of femoral fractures in nonaccidental injury. J Pediatr Orthop. 2000;20:411–413.
Scherl SA, Miller L, Lively N, Russinoff S, Sullivan CM, Tornetta P 3rd. Accidental and nonaccidental femur fractures in children. Clin Orthop Relat Res. 2000;376:96–105.
Schwend RM, Werth C, Johnston A. Femur shaft fractures in toddlers and young children: rarely from child abuse. J Pediatr Orthop. 2000;20:475–481.
Shaw BA, Murphy KM, Shaw A, Oppenheim WL, Myracle MR. Humerus shaft fractures in young children: accident or abuse? J Pediatr Orthop. 1997;17:293–297.
Sidebotham PD, Pearce AV. Audit of child protection procedures in accident and emergency department to identify children at risk of abuse. BMJ. 1997;315:855–856.
Worlock P, Stower M, Barbor P. Patterns of fractures in accidental and non-accidental injury in children: a comparative study. Br Med J (Clin Res Ed). 1986;293:100–102.
Acknowledgments
We thank Dr Cindy Christian, and the Department of Pediatrics at the Children’s Hospital of Philadelphia. In addition, we acknowledge the SCAN team and the Department of Emergency Medicine and Trauma at the Children’s Hospital of Philadelphia.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Baldwin, K., Pandya, N.K., Wolfgruber, H. et al. Femur Fractures in the Pediatric Population: Abuse or Accidental Trauma?. Clin Orthop Relat Res 469, 798–804 (2011). https://doi.org/10.1007/s11999-010-1339-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-010-1339-z