
Abstract
Since the publication in 2000 of the updated American College of Rheumatology (ACR) recommendations for the medical management of patients with lower limb osteoarthritis (OA), additional recommendations, newer epidemiologic studies, systematic reviews, and clinical trials have been published. The results of these reviews, studies, and trials, which highlight the greater efficacy of nonsteroidal anti-inflammatory drugs (NSAIDs) for controlling pain and the potential serious upper gastrointestinal toxicity of acetaminophen, require us to reassess the use of acetaminophen as the first-line pharmacologic agent for all patients with knee OA. Furthermore, the documented efficacy of glucosamine for pain relief and function improvement in patients with knee OA, with an effect size that is comparable with that of NSAIDs, requires us to reassess the use of glucosamine as a potential first-line agent at least for patients with knee OA who have mild-to-moderate pain. The availability of the cyclo-oxygenase 2 (COX-2)-specific inhibitors and their documented greater safety relative to traditional dual-inhibitor NSAIDs with regard to serious upper gastrointestinal toxicity lead us to reassess the use of traditional NSAIDs in patients with OA, especially in those at increased risk for such adverse events. The COX-2-specific inhibitors cost less than the combination of a generic NSAID plus a proton-pump inhibitor. The results of ongoing and future studies, especially of structure-modifying antiosteoarthritis drugs, will lead to further reassessment and updating of recommendations for the medical management of patients with knee OA. Hopefully, the use of such recommendations will improve the outcomes for patients with this debilitating chronic condition.
Similar content being viewed by others

References and Recommended Reading
American College of Rheumatology Subcommittee on Osteoarthritis Guidelines: Recommendations for the medical management of osteoarthritis of the hip and knee. Arthritis Rheum 2000, 43:1905–1915. The subcommittee updated the recommendations for the management of hip and knee osteoarthritis to take into account new treatments including COX-2-selective inhibitors, intra-articular hyaluronan injections, and the use of nutritional supplements.
Pendleton A, Arden N, Dougados M, et al.: EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2000, 59:936–944. The EULAR task force performed a systematic review and metaanalysis of the published trials of pharmacologic treatments for knee osteoarthritis. However, there were insufficient data on which to base therapeutic recommendations. Therefore, the recommendations were based on a consensus of experts from several European countries.
Tannenbaum H, Peloso PMJ, Russell AS, Marlow B:An evidence-based approach to prescribing NSAIDs in the treatment of osteoarthritis and rheumatoid arthritis: The Second Canadian Consensus Conference. Can J Clin Pharmacol 2000, 7:4A-16A.
Petrella RJ: Is exercise effective treatment of osteoarthritis of the knee? West J Med 2001, 174:191–196.
Eccles M, Freemantle N, Mason J, for the North of England Non-Steroidal Anti-Inflammatory Drug Guideline Development Group: North of England evidence based guideline development project: summary guideline for non-steroidal anti-inflammatory drugs versus basic analgesia in treating the pain of degenerative arthritis. BMJ 1998, 317:526–530.
Altman RD, for the IAP Study Group: Ibuprofen, acetaminophen and placebo in osteoarthritis of the knee: a six-day double-blind study. Arthritis Rheum 1999, 42:S403. Abstract.
Pincus T, Callahan LF, Wolfe F, et al.: Arthrotec compared to acetaminophen: a clinical trial in patients with osteoarthritis of the hip or knee. Arthritis Rheum 1999, 42:S404. Abstract.
Geba G, Weaver AL, Schnitzer TJ, et al.: A clinical trial comparing rofecoxib to celecoxib and acetaminophen in the treatment of osteoarthritis: early efficacy results. Ann Rheum Dis 2000, 59:133. Abstract.
Wolfe F, Zhao D, Lane N: Preference for nonsteroidal antiinflammatory drugs over acetaminophen by rheumatic disease patients: a survey of 1,799 patients with osteoarthritis, rheumatoid arthritis, and fibromyalgia. Arthritis Rheum 2000, 43:378–385.
Pincus T, Swearingen C, Cummins P, Callahan LF: Preference for nonsteroidal antiinflammatory drugs versus acetaminophen and concomitant use of both types of drugs in patients with osteoarthritis. J Rheumatol 2000, 27:1020–1027.
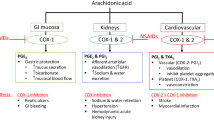
Garcia Rodriguez LA, Hernandez-Diaz S: The risk of upper gastrointestinal complications associated with nonsteroidal anti-inflammatory drugs, glucocorticoids, acetaminophen, and combinations of these agents. Arthritis Res 2001, 2:98–101. This article highlights results of analysis of data from the UK General Practice Research Database examining the association between several pharmacologic agents and the risk of serious upper gastrointestinal complications including bleeding and perforation. These data suggest that acetaminophen may not be as safe as previously believed.
Warner TD, Guiliao F, Vojnovic I, et al.: Nonsteroid drug selectivities for cyclo-oxygenase 1 rather than cyclo-oxygenase 2 are associated with human gastrointestinal toxicity: a full in vitro analysis. Proc Natl Acad Sci USA 1999, 96:7563–7568.
Watson MC, Brookes ST, Kirwan JR, Faulkner A: Non-aspirin, non-steroidal anti-inflammatory drugs for osteoarthritis of the knee (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Towheed T, Shea B, Wells G, Hochberg M: Analgesia and non-aspirin, non-steroidal anti-inflammatory drugs for osteoarthritis of the hip (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Gotzsche PC: Non-steroidal anti-inflammatory drugs. BMJ 2000, 320:1058–1061.
Hernandez-Diaz S, Garcia Rodriguez LA: Association between nonsteroidal anti-inflammatory drugs and upper gastrointestinal tract bleeding and perforation: an overview of epidemiological studies published in the 1990s. Arch Intern Med 2000, 160:2093–2099.
Griffin MR, Yared A, Ray WA: Nonsteroidal antiinflammatory drugs and acute renal failure in elderly persons. Am J Epidemiol 2000, 151:488–496.
Garcia Rodriguez LA, Hernandez-Diaz S: The epidemiology of myocardial infarction and heart failure among users of nonsteroidal anti-inflammatory drugs. Epidemiology 2000, 11:382–387. This analysis demonstrates that the use of nonsteroidal antiinflammatory drugs conveys a significant risk for hospitalization for congestive heart failure. This is another serious adverse event that may have greater import for overall morbidity and mortality than serious upper gastrointestinal complications of NSAID therapy.
Page J, Henry D: Consumption of NSAIDs and the development of congestive heart failure in elderly patients: an underrecognized public health problem. Arch Intern Med 2000, 160:777–784.
Nielsen GL, Sorensen HT, Larsen H, Pedersen L: Risk of adverse birth outcome and miscarriage in pregnant users of non-steroidal anti-inflammatory drugs: population based observational study and case-control study. BMJ 2001, 322:266–270.
Hernandez-Diaz S, Garcia Rodriguez LA: Epidemiological assessment of the safety of conventional nonsteroidal anti-inflammatory drugs. Am J Med 2001, 110:20S-27S.
Moore RA, Tramer MR, Carroll D, Wiffen PJ, McQuay HJ:Quantitative systematic review of topically applied nonsteroidal anti-inflammatory drugs. BMJ 1998, 316:333–338.
Lipsky PE, Abramson SB, Breedveld FC, et al.: Analysis of the effect of COX-2 specific inhibitors and recommendations for their use in clinical practice. J Rheumatol 2000, 27:1338–1340.
Lipsky PE: Recommendations for the clinical use of cyclooxygenase-2 specific inhibitors. Am J Med 2001, 110:3S-5S.
Simon LS, Lanza FL, Lipsky PE, et al.: Preliminary study of the safety and efficacy of SC-58365, a novel cyclooxygenase 2 inhibitor. Arthritis Rheum 1998, 41:1591–1602.
Bensen WG, Flechtner JJ, McMillen JI, et al.: Treatment of osteoarthritis with celecoxib, a cyclooxygenase-2 inhibitor: a randomized controlled trial. Mayo Clin Proc 1999, 74:1095–1105.
McKenna F, Borenstein D, Wendt H, et al.: Celecoxib versus diclofenac in the management of osteoarthritis of the knee: a placebo-controlled, randomised, double-blind comparison. Scand J Rheumatol 2001, 30:11–18.
Ehrich EW, Schnitzer TJ, McIlwain H, et al.: Effect of specific COX-2 inhibition in osteoarthritis of the knee: a 6 week double blind, placebo controlled pilot study of rofecoxib. J Rheumatol 1999, 26:2438–2447.
Saag K, van der Heijde D, Fisher C, et al.: Rofecoxib, a new cyclooxygenase-2 inhibitor, shows sustained efficacy, comparable with other nonsteroidal anti-inflammatory drugs: a 6-week and a 1-year trial in patients osteoarthritis. Arch Fam Med 2000, 9:1124–1134.
Day R, Morrison B, Luza A, et al.: A randomized trial of the efficacy and tolerability of the COX-2 inhibitor rofecoxib vs ibuprofen in patients with osteoarthritis. Arch Intern Med 2000, 160:1781–1787.
Acevedo E, Castaneda O, Ugaz M, et al.: Tolerability profiles of rofecoxib (Vioxx) and Arthrotec. Scand J Rheumatol 2001, 30:19–24.
Simon LS, Weaver AL, Graham DY, et al.: Anti-inflammatory and upper gastrointestinal effects of celecoxib in rheumatoid arthritis: a randomized controlled trial. JAMA 1999, 282:1921–1928.
Laine L, Harper S, Simon T, et al.: A randomized trial comparing the effect of rofecoxib, a cyclooxygenase 2-specific inhibitor, with that of ibuprofen on the gastroduodenal mucosa of patients with osteoarthritis. Gastroenterology 1999, 117:776–783.
Hawkey C, Laine L, Simon T, et al.: Comparison of the effect of rofecoxib (a cyclooxygenase 2 inhibitor), ibuprofen, and placebo on the gastroduodenal mucosa of patients with osteoarthritis: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2000, 43:370–377.
Langman MJ, Jensen DM, Watson WJ, et al.: Adverse upper gastrointestinal effects of rofecoxib compared with NSAIDs. JAMA 1999, 282:1929–1933.
Silverstein FE, Faich G, Goldstein JL, et al.: Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis. JAMA 2000, 284:1247–1255. The results of the CLASS trial. This trial showed that the risk of symptomatic ulcers plus complicated ulcers was lower among patients with arthritis not taking low dose aspirin but taking celecoxib than among patients taking diclofenac or ibuprofen. The results have subsequently been reexamined in light of data presented at the FDA Arthritis Advisory Committee in February 2001. The data are not included in this paper.
Bombardier C, Laine L, Reicin A, et al.: Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000, 343:1520–1528. The results of the VIGOR trial. This trial showed that the risk of confirmed clinical upper gastrointestinal events and confirmed complicated upper gastrointestinal events were lower among patients with rheumatoid arthritis not taking low dose aspirin who were randomized to rofecoxib than patients randomized to naproxen. The overall safety of rofecoxib has been debated based on a higher incidence of myocardial infarction noted in this trial.
de Abajo FJ, Garcia Rodriguez LA: Risk of upper gastrointestinal bleeding and perforation associated with low-dose aspirin as plain and enteric-coated formulations. BMC Clin Pharmacol 2001, 1:1–8.
Brater DC: Effects of nonsteroidal anti-inflammatory drugs on renal function: focus on cyclooxygenase-2 selective inhibition. Am J Med 1999, 107:65S-71S.
Whelton A: Renal aspects of treatment with conventional nonsteroidal anti-inflammatory drugs versus cyclooxygenase-2 specific inhibitors. Am J Med 2001, 110:33S-42S.
Lanza FL, and the Members of the Ad Hoc Committee on Practice Parameters of the American College of Gastroenterology: A guideline for the treatment and prevention of NSAIDinduced ulcers. Am J Gastroenterol 1998, 93:2037–2046.
Silverstein FE, Graham DY, Senior JR, et al.: Misoprostol reduces serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal antiinflammatory drugs: a randomized, double-blind, placebocontrolled trial. Ann Intern Med 1995, 123:241–249.
Ekstrom P, Carling I, Wetterhus S, et al.: Prevention of peptic ulcer and dyspeptic symptoms with omeprazole in patients receiving continuous non-steroidal anti-inflammatory drug therapy: a Nordic multicentre study. Scand J Gastroenterol 1996, 31:753–758.
Hawkey CJ, Karrasch JA, Szczepanski L, et al.: Omepraxole compared with misoprostol for ulcers associated with nonsteroidal antiinflammatory drugs. N Engl J Med 1998, 338:727–734.
McAlindon TE, LaValley MP, Gulin JP, Felson DT: Glucosamine and chondroitin for treatment of osteoarthritis: a systematic quality assessment and meta-analysis. JAMA 2000, 283:1469–1475.
Towheed TE, Anastassiades TP, Shea B, et al.: Glucosamine therapy for treating osteoarthritis (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Reginster JY, Deroisy R, Rovati LC, et al.: Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. Lancet 2001, 357:251–256.
Ezzo J, Hadhazy V, Birch S, et al.: Acupuncture for osteoarthritis of the knee: a systematic review. Arthritis Rheum 2001, 44:819–825.
Little CV, Parsons T: Herbal therapy for treating osteoarthritis (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Verhagen AP, de Vet HCW, de Bie RA, et al.: Balneotherapy for rheumatoid arthritis and osteoarthritis (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Osiri M, Welch V, Brousseau L, et al.: Transcutaneous electrical nerve stimulation for knee osteoarthritis (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Brousseau L, Welch V, Wells G, et al.: Low level laser therapy (Classes I, II and III) for treating osteoarthritis (Cochrane Review). In The Cochrane Library, Issue 1. Oxford: Update Software; 2001.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Hochberg, M.C. What a difference a year makes: Reflections on the ACR recommendations for the medical management of osteoarthritis. Curr Rheumatol Rep 3, 473–478 (2001). https://doi.org/10.1007/s11926-001-0060-z
Issue Date:
DOI: https://doi.org/10.1007/s11926-001-0060-z