
Abstract
Introduction
This study evaluated outcomes for the first 100 bariatric surgical procedures in a single, publicly funded Irish centre.
Methods
This was a retrospective, chart-based study. Demographics and comorbidities of patients, peri- and post-operative outcomes and health benefits obtained by surgery were assessed.
Results
In total, 87 patients underwent Roux-en-Y gastric bypass procedures, 11 underwent sleeve gastrectomies and 2 underwent duodenal switch. The first 13 operations were done as open procedures. Of the remaining 87 cases, 85 were started laparoscopically. Postoperatively, 2 laparotomies were performed for bleeding and 2 patients developed incarcerated incisional hernias that required repair. The 30-day readmission rate was 6% of which 2 patients required emergency surgery. There was one postoperative mortality from cardio-respiratory failure.
Conclusions
This series audits the introduction of a publicly funded bariatric service in Ireland and reports a high percentage of procedures completed laparoscopically with an acceptable morbidity and mortality.
Similar content being viewed by others

Introduction
Obesity, defined as a BMI > 30, has become prevalent in Irish society in recent years. The problem has been formally recognised at governmental level with the publication of The Report of the National Taskforce on Obesity in 2005 [1]. Data collated in this document found that 39% of Irish adults were overweight and 18% were obese. It also found that there were over 300,000 overweight and obese children in Ireland, and estimated that this rate was rising at 10,000 per annum.
Obesity itself has a huge impact on health, contributing to and exacerbating a plethora of illnesses including hypertension, type 2 diabetes, hypercholesterolaemia, stroke, cardiovascular disease, hypertension, gallstones, osteoarthritis, obstructive sleep apnoea and some types of cancer [2–4]. Psychological and serious psychosocial disorders are also common amongst obese people. The resulting indirect cost of obesity in Ireland is estimated at €0.4 billion per annum [1].
There is good evidence that bariatric surgery is the most enduring and efficacious means of tackling morbid obesity in terms of weight loss [5]. Furthermore, a study by Adams et al. [6] found that adjusted long-term mortality from any cause decreased by 40% in patients who had undergone bariatric surgery compared to overweight controls. This study also found that cause-specific mortality was also seen to decrease by 56% for coronary artery disease, 92% for diabetes and by 60% for cancer in those patients who had undergone bariatric surgery.
Whilst well established internationally, access to bariatric surgery is still limited in Ireland. A bariatric service was established in our institution in January 2001. All new referrals to this service are seen by a multi-disciplinary team including endocrinology, dietetics, physiotherapy, psychology and surgery. This approach complies with the recently published Royal College of Surgeons of Ireland Guidelines on Surgery for Morbid Obesity [7].
The aim of this study was to audit the demographics, inpatient and outpatient outcomes of the first 100 bariatric surgery cases performed between 2001 and 2008. The general status and comorbidities of patients, peri- and post-operative outcomes and health benefits obtained by surgery were all assessed.
Materials and methods
A retrospective, chart-based review of the first hundred bariatric surgery cases was performed. Patients were identified using a dedicated bariatric database. In order to ensure accuracy and to generate further information, charts from all 100 patients were reviewed. General demographic information collected included age, sex, pre-operative weight (kg), BMI, year of surgery, co-morbidities, medications, and data from preoperative medical evaluation. Operative information collected included type of operation, open or laparoscopic, length of operation, intra-op complications and length of bypass limb. All postoperative complications were recorded in both the long and short term. In addition, changes in the average percentage of excess weight loss over time, medications and co-morbidities. Metabolic indices including glucose and lipid profiles were also assessed.
Results
Demographics
There were 32 males and 68 females with an average age of 45 (range 20–69). Figure 1 shows the age distribution of these patients. The average BMI for all patients was 55 (range 40–70) with the average BMI being higher in females (55.5 compared to males 48.5). Where possible, note was made of the age at which the patients actually became obese. Of the 63 patients where this information had been recorded 23 (37%) had been obese since childhood, 17 (27%) since their teens, 18 (29%) since their 20s and 5 (7%) since their 30s.

Bar chart illustrating age of patients in study
Preoperative co-morbidities
Many of the hundred patients included in this study had comorbid diseases. The most common comorbidities were: osteoarthritis (n = 38), hypertension (n = 37), respiratory disease (n = 36), depression (n = 30), diabetes (n = 22) and cardiac disease (n = 10). In addition, most patients were on multiple medications. The average number of medications per patient was 4 (range 0–16).
Preoperative workup
All patients underwent routine preoperative investigations including routine blood tests, ECG and departmental chest X-ray. Of these, six patients underwent preoperative echocardiography and eight required prolonged preoperative admission for a very low calorie diet. In the latter part of this series, OGD was performed routinely. In total, 66 patients underwent an OGD prior to surgery and of these 23 (35%) were CLO positive and were treated with triple therapy. In addition, nine patients had a hiatus hernia, one had oesophagitis and one had a pre-pyloric ulcer which was proven benign on biopsy.
Operative details
The first procedures were carried out in 2001(n = 2) and volume increased progressively to a current level of over 20 per year (Fig. 2). The majority of patients (n = 87) underwent Roux-en-Y gastric bypass (RNYGB) procedures. Of the remaining 13 patients, 11 underwent sleeve gastrectomies and 2 underwent duodenal switch. Of the 11 patients who initially underwent sleeve gastrectomies, 7 went on to be converted to RNYGB. The average length of operation was 227 min (range 150–420 min).

Bar chart illustrating number of cases/year. Asterisk denotes incomplete data for 2008 as hundredth patiet was reached
The first 13 operations were performed as open procedures. Thereafter, of the remaining 87 cases, 85 (98%) were started laparoscopically. Only 2 (2%) of these were converted to open procedures. The first was converted as a result of a large intra-operative bleed that could not be controlled laparoscopically and the second was converted because of adhesions from previous surgery.
The average bypass length was 130 cm (range 100–160). In more recent years, samples of omentum, small bowel, subcutaneous fat and liver core biopsies have been procured from 28 patients for research purposes.
Complications: intra-operative
In total there were five recorded intraoperative complications. The first and most serious one involved very heavy bleeding from left gastric artery whilst creating the pouch-jejunostomy. This was converted to open and this patient required an intra-operative blood transfusion. Further complications included the nasogastric tube accidentally getting caught in the staple line (n = 2), a stapler misfiring (n = 1) and difficulty in fashioning the gastric pouch due to adhesions from previous surgery (n = 1).
Complications: postoperative
In total four patients developed complications in the immediate postoperative period. Two patients required re-operation as they developed incarcerated hernias in pre-existing abdominal wall hernias. Both of these patients underwent emergency surgery and were discharged home well after 6 and 11 days, respectively. One patient who had undergone a laparoscopic sleeve gastrectomy developed a bleed with haemodynamic instability that required a laparotomy and oversewing of the staple line. He required a prolonged postoperative hospital stay (36 days), but went on to make a full recovery. The last complication was a respiratory arrest day 1 (n = 1) which was thought to result from opiate hypersensitivity. This patient made a full recovery.
Complications: inpatient mortality
There was one death in this series. This was in a 37-year-old super-obese male patient (BMI = 60) with pre-existing respiratory disease. His procedure was converted from laparoscopic to open because of poor access. He subsequently developed rapidly progressive cardio-respiratory failure and died 72 h postoperatively. His post mortem examination found the cause of death to be secondary to a previously undiagnosed cardiomyopathy.
Complications: <30 days readmissions
In total six patients were readmitted within 30 days of discharge. Four of these were for relatively minor reasons including nausea and vomiting, non-specific chest pain, Clostridium difficile infection and a port site abscess. The first major complication was an incarcerated port site hernia that necessitated a laparotomy and small bowel resection. The second was a large anastomotic bleed that required an emergency laparotomy and oversewing of the left gastric artery. It was later discovered that the bleed was as a result of an erosion from a sealed anastomotic leak.
Complications: >30 days post discharge
Many patients developed relatively minor and often transient postoperative symptoms that did not require surgical intervention (Table 1). Five patients developed incisional hernias that required elective repair and one patient had a non-fatal pulmonary embolus 2 months postoperatively.
The most serious complication was a volvulus of the entire small bowel through a mesenteric defect in a patient who had undergone laparoscopic RNYGB 3 years previously. This patient underwent a laparotomy, reduction of the volvulus and plication of the mesenteric defect. She went on to require a second laparotomy 3 days later where necrosis of the Roux loop and entero-enterostomy were found. The necrotic area was excised and the anastomosis refashioned. Her recovery was further complicated by an adhesional small bowel obstruction which required a further laparotomy. Her total inpatient stay was 9 weeks; however, she went on to make a slow but full recovery.
Postoperative weight loss
All patients lost weight postoperatively (Fig. 3). In the first postoperative year, rapid weight loss was seen to occur in all patients with an average weight loss of 58% of excess weight. In subsequent years of follow-up, on average, patients’ weight remained stable at 60% excess weight loss (Fig. 3). On an individual level, some patients were noted to start putting on weight after the first year, but usually this was up to only 5% of excess body weight.

Average percentage of excess weight loss postoperatively
Effects of bariatric surgery on morbidity and metabolic indices
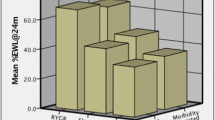
In terms of direct health benefits of surgery, all patients who were previously prescribed CPAP for obstructive sleep apnoea had discontinued its use in the first postoperative year. Similarly, many patients were able to discontinue the use of anti-hypertensive medications and inhalers. From a metabolic perspective, marked improvements in HBA1C, cholesterol, LDL, HDL and triglycerides were seen (Fig. 4). Figure 4a shows the improvements seen in HbA1C levels over time. Preoperatively, levels were normal in only 42% of patients, but even 6–8 weeks postoperatively 84% of patients had levels within the normal range. This improvement was then maintained over time with over 90% of patients having normal HbA1C at 1 and 2 years postoperatively. Figure 4b shows the improvements in HDL over time. Preoperatively only 65% of patients had levels within the normal range. At 6 months postoperatively, however, 80% of patients had levels within the normal range and from 1 year onwards, 100% of patients had normal HDL levels. Figure 4c shows the improvements seen in serum triglyceride levels over time. Preoperatively only 40% of patients were in the normal range. At 6–8 weeks postoperatively, this level had increased to 50% and by 1 year 75% of patients were in the normal range. Interestingly, these values deteriorated slightly at 2 years postoperatively with only 60% of patients being in the normal range. Figure 4d shows the improvements in serum cholesterol over time. Preoperatively, only 60% of patients were in the normal range. At 6–8 weeks postoperatively, this level had increased to 83% and by 1 year 86% of patients were in the normal range. Similar to the trend seen in serum triglyceride levels, serum cholesterol had deteriorated slightly by 2 years postoperatively with 79% of patients being in the normal range. LDL was also measured but was found to be within normal limits at all time points.

Metabolic indices: percentage of patients in normal range over time
Positive impact on quality of life
Data on postoperative quality of life was available for 44 patients. All patients reported a noticeable increase in their ability to exercise and in their general mobility. Patients directly attributed this to their weight loss and to reduced symptoms from mechanical comorbidities such as osteoarthritis of the back and knees. From a psycho-social perspective the majority of patients reported notable improvements in their self-confidence and mood and some no longer required antidepressant medications. One interesting finding was that 13 patients developed new addictive behaviours including secretive binge eating (n = 6), alcoholism (n = 4), heavy smoking (n = 2) and compulsive oil painting (n = 1).
Discussion
This report audits the early experiences of a publicly funded bariatric surgery service in Ireland. Initially this service started with a small number of open cases and evolved to provide around 20 laparoscopic cases per year. The average patient in this series had a BMI of 55, many had multiple comorbidities and 28% were over 50 years old. These adverse characteristics reflect the fact that a public service of this type will inevitably attract a relatively high-risk cohort of patients. Despite the adverse characteristics of the patients in this series, the overall morbidity and 30-day re-admission rates in this series are equivalent to those reported from other centres internationally [8–10]. With the development of the programme, gastric banding is also being provided in addition to RNYGB.
One important aspect of this data is the prevalence of incisional hernias. In this series two patients developed incarcerated hernias in the immediate postoperative period in pre-existing defects in the abdominal wall. These could not have been closed intraoperatively and so it is difficult to see how these could be avoided. One further patient developed a port site hernia 2 weeks post-discharge that necessitated small bowel resection and a further five patients developed incisional hernias in long-term follow-up that required elective repair. Of the true port site hernias that resulted from RNYGB, again it is difficult to see how these could be avoided as all 10- and 12-mm port sites were closed as routine.
Positive aspects of this data include the vast range of benefits seen in patients postoperatively. Patients sustained an average of 60% excess weight loss that was maintained years after their original operation. In addition, improvements were seen in serum cholesterol, HDL and triglyceride levels that again were maintained during follow-up. This phenomenon mirrors that seen in the international literature [11].
Of particular interest is that whilst only 42% of patients had normal fasting HBA1C preoperatively, this had normalised in over 80% of patients by 6–8 weeks post-operatively and in over 90% of patients by 1 year. Again the fact that bariatric surgery can reverse diabetes has previously been described in the international literature [12]. Additional benefits were an increased ability to exercise, improvement in psychosocial status and the ability to stop medications for chronic disease.
The results of this audit show that weight loss and metabolic parameters all improve within the first year postoperatively but that after this point, in certain instances they start to deteriorate again. As such, all patients need lifelong follow-up.
Conclusions
The data derived from this series clearly demonstrates the benefits of bariatric surgery. All patients experienced significant and continued weight loss with a concomitant improvement in metabolic profiles and psychosocial wellbeing. On a cautionary note, before being considered for surgical management these benefits need to be carefully weighed against the potentially severe and occasionally fatal operative outcomes. It is therefore essential that the decision to operate is based on both rigorous preoperative multi-disciplinary review and fully informed consent from patients themselves.
References
http://www.dohc.ie/publications/report_taskforce_on_obesity.html
Ogden CL, Yanovski SZ, Carroll MD et al (2007) The epidemiology of obesity. Gastroenterology 132(6):2087–2102
Kenchaiah S, Evans JC, Levy D et al (2002) Obesity and the risk of heart failure. N Engl J Med 347(5):305–313
Sinha R, Fisch G, Teague B et al (2002) Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med 346(11):802–810
Elder KA, Wolfe BM (2007) Bariatric surgery: a review of procedures and outcomes. Gastroenterology 132(6):2253–2271
Adams KF, Schatzkin A, Harris TB et al (2006) Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med 355(8):763–778
Guidelines for the delivery of obesity surgery, Royal College of Surgeons in Ireland. http://www.rcsi.ie
Saunders JK, Ballantyne GH, Belsley S et al (2007) 30-day readmission rates at a high volume bariatric surgery center: laparoscopic adjustable gastric banding, laparoscopic gastric bypass, and vertical banded gastroplasty-Roux-en-Y gastric bypass. Obes Surg 17(9):1171–1177
Morino M, Toppino M, Forestieri P et al (2007) Mortality after bariatric surgery: analysis of 13,871 morbidly obese patients from a national registry. Ann Surg 246(6):1002–1007 (discussion 1007-1009)
Flancbaum L, Belsley S (2007) Factors affecting morbidity and mortality of Roux-en-Y gastric bypass for clinically severe obesity: an analysis of 1,000 consecutive open cases by a single surgeon. J Gastrointest Surg 11(4):500–507
Brizzi P, Angius MF, Carboni A et al (2003) Plasma lipids and lipoprotein changes after biliopancreatic diversion for morbid obesity. Dig Surg 20(1):18–23
Rubino F, Gagner M (2002) Potential of surgery for curing type 2 diabetes mellitus. Ann Surg 236(5):554–559
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Smith, F.M., Gallagher, H., O’Connell, J. et al. Laparoscopic bariatric surgery for morbid obesity: the first hundred cases in an Irish centre. Ir J Med Sci 179, 17–22 (2010). https://doi.org/10.1007/s11845-009-0413-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-009-0413-6