
Abstract
Background
Laparoscopic sleeve gastrectomy (LSG) is increasingly popular with surgeons because of its apparent technical ease. However, performing LSG safely is sometimes not possible during laparoscopy. The objectives of the present study were to (i) describe the context of LSG failure and (ii) suggest preoperative care options or strategies that enable secondary LSG to be performed safely.
Methods
We studied patients having undergone primary and secondary LSG between January 2008 and July 2013. The primary efficacy criterion was the LSG success rate. The secondary efficacy criteria were preoperative care procedures, the complication rate, the failure rate, and the frequency of conversion to open surgery.
Results
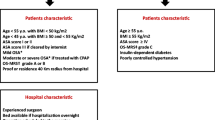
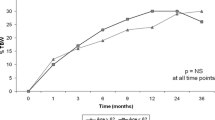
During the study period, 954 patients underwent first- or second-line LSG. Laparoscopic sleeve gastrectomy was technically impossible in 12 patients (1.2 %). The cause of failure was a large left liver lobe in seven cases (58.3 %) and a lack of space in five cases. Of these 12 patients, nine underwent secondary LSG. The median preoperative BMI before the first LSG was 51.5 kg/m2. The median (range) time interval between the two LSG attempts was 6 months (3–37). Prior to secondary LSG, the preoperative weight reduction measure was a diet in seven cases (78 %), an intragastric balloon in one case, and no treatment in one case. The median preoperative excess weight loss (EWL) before the second LSG was 10 % (0–20). Five LSGs were successful, two required conversion to open surgery, and two failed again. There were two postoperative complications (22 %), both of which concerned the two patients with conversion to laparotomy.
Conclusions
In the event of LSG technical failure, preoperative weight loss may enable a second attempt at laparoscopic treatment. A preoperative EWL of at least 10 % appears to be required for the avoidance of conversion to laparotomy.

Similar content being viewed by others

References
Silecchia G, Boru C, Pecchia A, et al. Effectiveness of laparoscopic sleeve gastrectomy (first stage of biliopancreatic diversion with duodenal switch) on co-morbidities in super-obese high-risk patients. Obes Surg. 2006;16:1138–44.
Topart P, Becouarn G, Ritz P. Comparative early outcomes of three laparoscopic bariatric procedures: sleeve gastrectomy, Roux-en-Y gastric bypass, and biliopancreatic diversion with duodenal switch. Surg Obes Relat Dis. 2012;8:250–4.
Boza C, Gamboa C, Salinas J, et al. Laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy: a case–control study and 3 years of follow-up. Surg Obes Relat Dis. 2012;8:243–9.
Gastrectomie Longitudinale [sleeve gastrectomy] pour obésité. Hautes autorité de la santé. Recommandations 2008.
Verhaeghe P, Dhahri A, Qassemyar Q, Regimbeau JM. Technique de la gastrectomie longitudinal (sleeve gastrectomy) par laparoscopie. EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales–Appareil digestif, 40–385, 2011.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Deitel M, Greenstein RJ. Recommendations for reporting weight loss. Obes Surg. 2003;13:159–60.
Kissane NA, Pratt JS. Medical and surgical treatment of obesity. Best Pract Res Clin Anaesthesiol. 2011;25:11–25.
Sjöström L, Lindroos AK, Peltonen M, et al. Swedish Obese Subjects Study Scientific Group. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–93.
Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012;366:1567–76.
Ikramuddin S, Korner J, Lee WJ, et al. Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes, hypertension, and hyperlipidemia: the Diabetes Surgery Study randomized clinical trial. JAMA. 2013;309:2240–9.
Kaul A, Sharma J. Impact of bariatric surgery on comorbidities. Surg Clin N Am. 2011;91:1295–312. ix.
Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240:416–23. discussion 423–4.
Kehagias I, Spyropoulos C, Karamanakos S, et al. Efficacy of sleeve gastrectomy as sole procedure in patients with clinically severe obesity (BMI ≤50 kg/m(2)). Surg Obes Relat Dis. 2013;9:363–9.
Fuks D, Verhaeghe P, Brehant O, et al. Results of laparoscopic sleeve gastrectomy: a prospective study in 135 patients with morbid obesity. Surgery. 2009;145:106–13.
Pequignot A, Fuks D, Verhaeghe P, et al. Is there a place for pigtail drains in the management of gastric leaks after laparoscopic sleeve gastrectomy? Obes Surg. 2012;22:712–20.
Rebibo L, Mensah E, Verhaeghe P, et al. Simultaneous gastric band removal and sleeve gastrectomy: a comparison with front-line sleeve gastrectomy. Obes Surg. 2012;22:1420–6.
Luyckx FH, Desaive C, Thiry A, et al. Liver abnormalities in severely obese subjects: effect of drastic weight loss after gastroplasty. Int J Obes Relat Metab Disord. 1998;22:222–6.
Rebibo L, Gerin O, Verhaeghe P, et al. Laparoscopic sleeve gastrectomy in patients with NASH-related cirrhosis: a case-matched study. Surg Obes Relat Dis. 2014. doi:10.1016/j.soard.2013.09.015.
Schwartz ML, Drew RL, Chazin-Caldie M. Factors determining conversion from laparoscopic to open Roux-en-Y gastric bypass. Obes Surg. 2004;14:1193–7.
Fris RJ. Preoperative low energy diet diminishes liver size. Obes Surg. 2004;14:1165–70.
Iannelli A, Martini F, Schneck AS, et al. Preoperative 4-week supplementation with omega-3 polyunsaturated fatty acids reduces liver volume and facilitates bariatric surgery in morbidly obese patients. Obes Surg. 2013;23:1761–5.
Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia. 2001;56:1024–6.
Sinha A, Jayaraman L, Punhani D. Efficacy of ultrasound-guided transversus abdominis plane block after laparoscopic bariatric surgery: a double blind, randomized, controlled study. Obes Surg. 2013;23:548–53.
Banka G, Woodard G, Hernandez-Boussard T, et al. Laparoscopic vs open gastric bypass surgery: differences in patient demographics, safety, and outcomes. Arch Surg. 2012;147:550–6.
Khan O, Irukulla S, Sanmugalingam N, et al. Simultaneous intra-gastric balloon removal and laparoscopic sleeve gastrectomy for the super-super obese patients—a prospective feasibility study. Obes Surg. 2013;23:585–7.
Mohamed ZK, Kalbassi MR, Boyle M, et al. Intra-gastric balloon therapy and weight reduction. Surgeon. 2008;6:210–2.
Leeman MF, Ward C, Duxbury M, et al. The intra-gastric balloon for pre-operative weight loss in bariatric surgery: is it worthwhile? Obes Surg. 2013;23:1262–5.
Zerrweck C, Sepúlveda EM, Maydón HG, et al. Laparoscopic gastric bypass vs. sleeve gastrectomy in the super obese patient: early outcomes of an observational study. Obes Surg. 2014;24:712–7.
Conflict of Interest
None of the authors have any conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Rebibo, L., Dhahri, A., Verhaeghe, P. et al. What to Do When It Is Technically Impossible to Perform Laparoscopic Sleeve Gastrectomy. OBES SURG 24, 2069–2074 (2014). https://doi.org/10.1007/s11695-014-1320-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1320-0