
Abstract
Background
The request to lose weight is expanding not only in obese and morbidly obese patients but also in overweight patients affected by co-morbidities as diabetes and hypertension and who do not tolerate diet regimen or lifestyle changes. The aim of this study is a multicenter evaluation of outcomes of intragastric balloon in overweight patients.
Methods
Patients (BMI 27–30 kg/m2) treated with a BioEnterics Intragastric Balloon (BIB) between 1996 and 2010 were extracted from the database of the participating centres in Rome (Italy), Liège (Belgium) and Madrid (Spain). Primary endpoints were the efficacy and safety at 6 and 42 months from balloon positioning. Secondary endpoints included resolution of co-morbidities.
Results
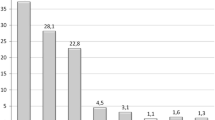
A total of 261 patients were included in this study. The most common indication for balloon placement was a psychological disorder (54 %). Mean body mass index (BMI) fell from 28.6 ± 0.4 at baseline to 25.4 ± 2.6 kg/m2 at 6 months and to 27.0 ± 3.1 kg/m2 at 3 years from BIB removal. The mean %EWL was 55.6 % at 6 months and 29.1 % at 3 years. Forty-seven patients (18 %) had complications associated with placement of the intragastric balloon (leak = 28, intolerance = 14, duodenal ulcer = 2, gastritis = 1, oesophagitis = 1, duodenal polyps = 1). The rate of patients with hypertension decreased from 29 % at baseline to 16 % at 3 years. Diabetes decreased from 15 to 10 %, dyslipidaemia decreased from 20 to 18 %, hypercholesterolaemia decreased from 32 to 21 % and osteoarthropathy decreased from 25 to 13 %.
Conclusions
The intragastric balloon is safe and effective in overweight patients, helping to reduce progression to obesity and decreasing the prevalence of a number of important co-morbidities.

Similar content being viewed by others


References
World Health Organization. Factsheet: obesity and overweight. http://www.who.int/hpr/NPH/docs/gs_obesity.pdf.
Seidell JC. The impact of obesity on health status: some implications for health care costs. Int J Obesity. 1996;19 Suppl 6:S13–6.
Adams KF, Schatzkin A, Harris TB, et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355:763–78.
Manson JE, Willett WC, Stampfer MJ, et al. Body weight and mortality among women. N Engl J Med. 1995;333:677–85.
Jung RT. Obesity as a disease. Br Med Bull. 1997;53:307–21.
Colditz GA, Willett WC, Rotnitsky A, et al. Weight gain as a risk factor for clinical diabetes in women. Arch Intern Med. 1995;122:481–6.
Chan JM, Rimm EB, Colditz GA, et al. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care. 1994;17:961–9.
Hubert HB, Feinleib M, McNamara PM, et al. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation. 1983;67:968–77.
Willet WC, Manson JE, Stampfer MJ, et al. Weight, weight change, and coronary heart disease in women. JAMA. 1995;273:461–5.
NIH Conference. Gastrointestinal surgery for severe obesity. Consensus development conference panel. Ann Intern Med. 1991;115:956–61.
Messina T, Genco A, Favaro R, et al. Intragastric balloon positioning and removal: sedation or general anesthesia? Surg Endosc. 2011;25:3811–4.
Sallet JA, Marchesini JB, Paiva DS, et al. Brazilian multicenter study of the intragastric balloon. Obes Surg. 2004;14:991–8.
Genco A, Bruni T, Doldi SB, et al. BioEnterics Intragastric Balloon: the Italian experience with 2,515 patients. Obes Surg. 2005;15:1161–4.
Lopez-Nava G, Rubio MA, Prados S, et al. BioEnterics® Intragastric Balloon (BIB®): single ambulatory center Spanish experience with 714 consecutive patients treated with one or two consecutive balloons. Obes Surg. 2011;21:5–9.
Angrisani L, Lorenzo M, Borrelli V, et al. Is bariatric surgery necessary after intragastric balloon treatment? Obes Surg. 2006;16:1135–7.
Genco A, Cipriano M, Bacci V, et al. BioEnterics Intragastric Balloon (BIB): a short-term, double-blind, randomised, controlled, crossover study on weight reduction in morbidly obese patients. Int J Obes. 2006;30:129–33.
Genco A, Balducci S, Bacci V, et al. Intragastric balloon or diet alone? A retrospective evaluation. Obes Surg. 2008;18:989–92.
Genco A, Cipriano M, Bacci V, et al. Intragastric balloon followed by diet vs intragastric balloon followed by another balloon: a prospective study on 100 patients. Obes Surg. 2010;20:1496–500.
Wadden TA, Sternberg JA, Letizia KA, et al. Treatment of obesity by a very low calorie diet, behaviour therapy, and their combination: a five-year perspective. Int J Obes. 1989;13 Suppl 2:39–46.
Patrick K, Calfas KJ, Norman GJ, et al. Outcomes of a 12-month web-based intervention for overweight and obese men. Ann Behav Med. 2011;42(3):391–401.
Loveman E, Frampton GK, Shepherd J, et al. The clinical effectiveness and cost-effectiveness of long-term weight management schemes for adults: a systematic review. Health Technol Assess. 2011;15(2):1–182.
Pappachan JM, Chacko EC, Arunagirinathan G, et al. Management of hypertension and diabetes in obesity: non-pharmacological measures. Int J Hypertens. 2011;3:98–105.
Williamson DF, Pamuk E, Thun M, et al. Prospective study of intentional weight loss and mortality in never-smoking overweight US white women aged 40–64 years. Am J Epidemiol. 1995;141:1128–41.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Genco, A., López-Nava, G., Wahlen, C. et al. Multi-Centre European Experience with Intragastric Balloon in Overweight Populations: 13 Years of Experience. OBES SURG 23, 515–521 (2013). https://doi.org/10.1007/s11695-012-0829-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-012-0829-3