
Abstract
Background: Partial conduction block has been suggested a predictor of recurrence of atrial flutter (AFL).
Aim: The aim of this study was to assess transverse conduction by the crista terminalis (CT) as a problem in evaluating isthmus block and the usefulness of differential pacing for distinguishing slow conduction (SC) and complete conduction block (CB) across the ablation line.
Methods: We assessed 14 patients who underwent radiofrequency catheter ablation of the eustachian valve/ridge–tricuspid valve isthmus for typical AFL. Activation patterns along the tricuspid annulus (TA) suggested incomplete CB across the isthmus. In these patients, atrial pacing was performed from the low posteroseptal (PS) and anteroseptal (AS) right atrium (RA) while the ablation catheter was placed at the ablation line where double potentials (DPs) could be recorded. The pattern of activation of the RA free wall was assessed by a 20-pole catheter positioned along the CT during pacing from the coronary sinus (CS) ostium (CSos) and low lateral RA (LLRA).
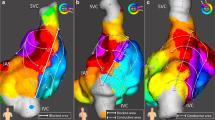
Results: Faster transverse conduction across the CT resulted in simultaneous or earlier activation of the distal halo electrodes than of the more proximal electrodes, suggesting incomplete conduction block across the isthmus. CB (13) and SC (1) were detected as changes in the activation times of the first and second components of DPs (DP1, DP2) during PS RA pacing and AS RA. Similar changes in the activation times DP1 and DP2 during AS RA pacing as compared to PS RA reflected SC through the isthmus, whereas increased DP1 activation time and decreased of DP2 activation time reflected complete conduction block across the isthmus.
Conclusions: Transverse conduction across the CT influences the sequence of activation along the TA after isthmus ablation. Differential pacing can distinguish SC from complete conduction block across the ablation line in the isthmus.
Similar content being viewed by others


References
Feld GK, Fleck RP, Chen PS, Boyce K, Bahnson TD, Stein JB, Calisi CM, Ibarra M. Radiofrequency catheter ablation for the treatment of human type 1 atrial flutter, identification of a critical zone in reentrant circuit by endocardial mapping techniques. Circulation 1992;86:1233–1240.
Cosio FG, Lopez-Gil M, Goicolea A, Arribas F, Barroso JL. Radiofrequency ablation of the inferior vena cava-tricuspid valve isthmus in common atrial flutter. Am J Cardiol 1993;71:705–709.
Poty H, Saoudi N, Abdel Aziz A, Nair M, Letac B. Radiofrequency catheter ablation of type l atrial flutter. Prediction of late success by electrophysiological criteria. Circulation1995;92:1389–1392.
Cauchemez B, Haissaguerre M, Fischer B, Thomas O, Clementy J, Coumel P. Electrophysiological effects of catheter ablation of inferior vena cava-tricuspid annulus isthmus in common atrial flutter. Circulation 1996;93:284–294.
Nakagawa H, Lazzara R, Khastgir T, Beckman KJ, McClelland JH, Imai S, Pitha JV, Becker AE, Arruda M, Gonzalez MD, Widman LE, Rome M, Neuhauser J, Wang X, Calame JD, Goudeau MD, Jackman WM. Role of the tricuspid annulus and the eustachian valve/ridge on atrial flutter. relevance to catheter ablation of the septal isthmus and a new technique for rapid identification of ablation success. Circulation 1996;94:407–424.
Poty H, Saoudi N, Nair M, Anselme F, Letac B. Radiofrequency catheter ablation of atrial flutter. Further insights into the various types of isthmus block: application to ablation during sinus rhythm. Circulation 1996;93:3204–3213.
Schwartzman D, Callans DJ, Gottlieb CD, Dillon SM, Movsowitz C, Marchlinski FE. Conduction block in the inferior vena cava-tricuspid valve isthmus: association with outcome of radiofrequency ablation of type I atrial flutter. J Am Coll Cardiol 1996;28:1519–1531.
Shah DC, Takahashi A, Jais P, Hocini M, Clementy J, Haissaguerre M. Local electrogram-based criteria of cavotricuspid isthmus block. J Cardiovasc Electrophysiol 1999;10:662–669.
Shah DC, Haissaguerre M, Jais P, Fischer B, Takahashi A, Hocini M, Clementy J. Simplified electrophysiologically directed catheter ablation of recurrent common atrial flutter. Circulation 1997;96:2505–2508.
Shah DC, Takahashi A, Jais P, Hocini M, Peng JT, Clementy J, Haissaguerre M. Tracking dynamic conduction recovery across the cavotricuspid isthmus. J Am Coll Cardiol 2000;35:1478–1484.
Olgin JE, Kalman JM, Fitzpatrick AP, Lesh MD. Role of right atrial endocardial structures as barriers to conduction during human type I atrial flutter. Activation and entrainment mapping guided by intracardiac echocardiography. Circulation 1995;92:1839–1848.
Arenal A, Almendral J, Alday JM, Villacastin J, Ormaetxe JM, Sande JL, Perez-Castellano N, Gonzalez S, Ortiz M, Delcan JL. Rate-dependent conduction block of the crista terminalis in patients with typical atrial flutter. Circulation 1999;99:2771–2778.
Schumacher B, Jung W, Schmidt H, Fischenbeck C, Lewalter T, Hagendorff A, Omran H, Wolpert C, Luderitz B. Transverse conduction capabilities of the crista terminalis in patients with atrial flutter and atrial fibrillation. J Am Coll Cardiol 1999;34:363–373.
Scaglione M, Riccardi R, Calo L, Di Donna P, Lamberti F, Caponi D, Coda L, Gaita F. Typical atrial flutter ablation: Conduction across the posterior region of the inferior vena cava orifice may mimic unidirectional isthmus block. J Cardiovasc Electrophysiol2000;11:387–395.
Shah D, Haissaguerre M, Takahashi A, Hocini M, Clementy J. Differential pacing for distinguishing block from persistent conduction through an ablation line. Circulation2000;102:1517–1522.
Jais P, Shah DC, Haissaguerre M, Hocini M, Garrigue S, Le Metayer P, Clementy J. Prospective randomized comparison of irrigated-tip versus conventional-tip catheters for ablation of common flutter. Circulation 2000;101:772–776.
Kottkamp H, Hindricks G. Catheter ablation of atrial flutter. Thorac Cardiovasc Surg1999;47:357–361.
Lesh MD. Catheter ablation of atrial flutter and tachycardia. In Zipes DP, Jalife J, eds. Cardiac Electrophysiology: From Cell to Bedside, 3rd ed. Philadelphia, PA: WB Saunders;2000:1009–1027.
Anselme F, Savoure A, Ouali S, Cribier A, Saoudi N. Transcristal conduction during isthmus ablation of typical atrial flutter: Influence on success criteria. J Cardiovasc Electrophysiol 2004;15: 184–189.
Matsushita T, Chun S, Liem LB, Friday KJ, Sung RJ. Unidirectional conduction block at cavotricuspid isthmus created by radiofrequency catheter ablation in patients with typical atrial flutter. J Cardiovasc Electrophysiol 2002;13:1098–1102.
Chen J, de Chillou C, Basiouny T, Sadoul N, Filho JD,Magnin-Poull I, Messier M, Aliot E. Cavotricuspid isthmus mapping to assess bidirectional block during common atrial flutter radiofrequency ablation. Circulation 1999;100:2507–2513.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sugimura, H., Watanabe, I., Okumura, Y. et al. Differential Pacing for Distinguishing Slow Conduction from Complete Conduction Block of the Tricuspid-Inferior Vena Cava Isthmus after Radiofrequency Ablation for Atrial Flutter—Role of Transverse Conduction through the Crista Terminalis. J Interv Card Electrophysiol 13, 125–134 (2005). https://doi.org/10.1007/s10840-005-0265-6
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s10840-005-0265-6