
Abstract
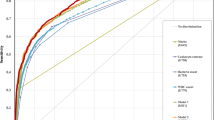
Objective: To investigate the accuracy of history taking to diagnose asymptomatic bacteriuria (ASB) in diabetic women, and the added value of leukocyturia. Methods: Data were obtained from a multicenter study including 465 women with diabetes. Many patient characteristics were considered as potential diagnostic determinants. A urinary leukocyte count and a urine culture (the criterion standard) were performed. Logistic regression analyses were performed and areas under the receiver operating characteristic curves (AUC) were calculated. Results: For women with type 1 diabetes (n=236; ASB 11%), duration of diabetes and glycosylated hemoglobin (GHb) were powerful predictors of ASB. The AUC of the model including these two variables was 0.66 (95% confidence interval (CI) 0.53–0.78). After addition of leukocyturia, the AUC increased considerably to 0.78 (95% CI 0.68–0.88; p = 0.018). For women with type 2 diabetes (n = 229; ASB 19%), age and the number of symptomatic urinary tract infections (UTIs) in the previous year were the strongest predictors of ASB. The AUC of the model including these variables was 0.70 (95% CI 0.61–0.80). After addition of leukocyturia, the AUC increased to 0.79 (95% CI 0.71–0.86; p=0.023). Conclusion: In diabetic women, ASB can be diagnosed using two easily obtainable variables (duration of diabetes and GHb for women with type 1 diabetes, and age and the number of UTIs in the previous year for women with type 2 diabetes) in combination with a urinary leukocyte count. This results in a model with sufficient accuracy (AUC > 0.75).
Similar content being viewed by others

References
Wheat LJ. Infection and diabetes mellitus. Diabetes Care 1980; 3: 187–197.
Schmitt JK, Fawcett CJ, Gullickson G. Asymptomatic bacteriuria and hemoglobin A1. Diabetes Care 1986; 9: 518–520.
Keane EM, Boyko EJ, Barth Reller L, Hamman RF. Prevalence of asymptomatic bacteriuria in subjects with NIDDM in San Luis Valley of Colorado. Diabetes Care 1988; 11: 708–712.
Geerlings SE, Stolk RP, Camps MJL, et al. Asymptomatic bacteriuria may be considered a complication in women with diabetes. Diabetes Care 2000; 23: 744–749.
Nicolle LE. Asymptomatic bacteriuria in diabetic women. Diabetes Care 2000; 23: 722–723.
Geerlings SE, Stolk RP, Camps MJL, et al. Conse-quences of asymptomatic bacteriuria in women with diabetes mellitus. Arch Intern Med 2001; 161: 1421–1427.
Harding GK, Zhanel GG, Nicolle LE, Cheang M. Antimicrobial treatment in diabetic women with asymptomatic bacteriuria. New Engl J Med 2002; 347: 1576–1583.
Geerlings SE, Meiland R, Hoepelman AI. Treatment of asymptomatic bacteriuria in diabetic women. New Engl J Med 2003; 348: 957–958.
Nelson RG, Knowler WC, Pettitt DJ, Bennett PH. National Diabetes Data Group (eds). Kidney diseases in diabetes, 2nd edn. Bethesda: National Institute of Health, Diabetes in America 1995; (16): 349–401.
Members of the medical research council bacteriuria committee. Recommended terminology of urinary tract infection. Br Med J 1979; 2: 717–719.
Van der Schouw YT, Verbeek AL, Ruijs JH. ROC curves for the initial assessment of new diagnostic tests. Fam Pract 1992; 9: 506–511.
De Long ER, De Long DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988; 44: 837–845.
Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this women have an acute uncomplicated urinary tract infection? JAMA 2002; 287: 2701–2710.
Hurlbut TA, Littenberg B, The diagnostic technology assessment consortium. The diagnostic accuracy of rapid dipstick tests to predict urinary tract infection. Am J Clin Pathol 1991; 96: 582–588.
Wigton RS, Hoellerich VL, Ornato JP, Leu V, Mazz-otta LA, Cheng IH. Use of clinical ndings in the 1026. diagnosis of urinary tract infection in women. Arch Intern Med 1985; 145: 2222–2227.
Stamm WE. Measurement of pyuria and its relation to bacteriuria. Am J Med 1983; 75(1B): 53–58.
Geerlings SE, Brouwer EC, Van Kessel KCPM, Gaa-stra W, Stolk RP, Hoepelman AIM. Cytokine secretion is impaired in women with diabetes mellitus. Eur J Clin Invest 2000; 30: 995–1001.
Zhanel GG, Harding GK, Nicolle LE. Asymptomatic bacteriuria in patients with diabetes mellitus. Rev Infect Dis 1991; 13: 150–154.
Kass EH. Asymptomatic infections of the urinary tract. T Assoc Am Physicians 1956; 69: 56–64.
Geerlings SE, Brouwer EC, Gaastra W, Hoepelman AIM. Is a second urine necessary for the diagnosis of asymptomatic bacteriuria? Clin Infect Dis 2000; 31: E3–4.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Meiland, R., Geerlings, S.E., Stolk, R.P. et al. History taking and leukocyturia predict the presence of asymptomatic bacteriuria in women with diabetes mellitus. Eur J Epidemiol 19, 1021–1027 (2004). https://doi.org/10.1007/s10654-004-2254-y
Issue Date:
DOI: https://doi.org/10.1007/s10654-004-2254-y