
Abstract
Objective
To identify trends in a residual category of cancers not typically associated with tobacco, screening, or human immunodeficiency virus (HIV) infection.
Methods
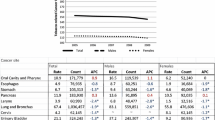
For persons aged 20–84, we used sex- and race-specific age-period-cohort (APC) models to describe temporal patterns of incidence (1975–2004) and mortality (1970–2004) in the U.S. for a residual cancer category that excluded non-Hodgkin lymphoma, Kaposi sarcoma, and cancer of the oral cavity and pharynx, esophagus, pancreas, larynx, lung and bronchus, urinary bladder, kidney and renal pelvis, colon and rectum, prostate, female breast, and cervix uteri.
Results
Age-specific incidence rose (0.1–0.9% per year, on average) in every sex-race group, with factors related to both time period and birth cohort membership appearing to accelerate the increases in women. Age-specific mortality fell (0.6–0.9% per year, on average) for black and white men and women, with the declines decelerating in white women but accelerating in the other sex-race groups. Extrapolations of APC models predicted higher age-adjusted incidence rates in white women (11%), black women (5%), and white men (4%) in 2005–2009, relative to 2000–2004, and lower rates in black men (−3%), accompanied by lower age-adjusted mortality rates in every sex-race group (−8% in black men, −3% in black women, −1% in white men, and −1% in white women).
Conclusions
The possibility that increased incidence in women over time reflects changes in underlying risks, diagnostic practices, or better case ascertainment should be actively explored. Declining mortality may signify improvements in cancer care.



Similar content being viewed by others


References
Espey DK, Wu X-C, Swan J et al (2007) Annual report to the nation on the status of cancer, 1975–2004, featuring cancer in American Indians and Alaska Natives. Cancer 110(10):2119–2152
55-Year trends in U.S. cancer death rates. http://seer.cancer.gov/csr/1975_2004/results_merged/topic_historical_mort_trends.pdf. Accessed 18 Jan 2008
US death rates 1975–2004. http://seer.cancer.gov/csr/1975_2004/results_merged/topic_graph_heartdis_cancer.pdf. Accessed 18 Jan 2008
Wingo PA, Ries LA, Giovino GA et al (1999) Annual report to the nation on the status of cancer, 1973–1996, with a special section on lung cancer and tobacco smoking. J Natl Canc Inst 91(8):675–690
Chu KC, Tarone RE, Freeman HP (2003) Trends in prostate cancer mortality among black men and white men in the United States. Cancer 97(6):1507–1516
Weir HK, Thun MJ, Hankey BF et al (2003) Annual report to the nation on the status of cancer, 1975–2000, featuring the uses of surveillance data for cancer prevention and control. J Natl Canc Inst 95(17):1276–1299
Ries LA, Wingo PA, Miller DS et al (2000) The annual report to the nation on the status of cancer, 1973–1997, with a special section on colorectal cancer. Cancer 88(10):2398–2424
Fisher SG, Fisher RI (2004) The epidemiology of non-Hodgkin’s lymphoma. Oncogene 23(38):6524–6534
Bailar JC 3rd, Gornik HL (1997) Cancer undefeated. N Engl J Med 336(22):1569–1574
Holford TR (1983) The estimation of age, period and cohort effects for vital rates. Biometrics 39(2):311–324
Dinse GE, Umbach DM, Sasco AJ, Hoel DG, Davis DL (1999) Unexplained increases in cancer incidence in the United States from 1975 to 1994: possible sentinel health indicators? Annu Rev Public Health 20:173–209
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat database: incidence—SEER 9 Regs limited-use, Nov 2006 Sub (1973–2004)—linked to county attributes—total U.S., 1969–2004 counties, National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2007, based on the November 2006 submission
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat database: mortality—all COD, public-use with state, total U.S. (1969–2004), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2007. Underlying mortality data provided by NCHS (www.cdc.gov/nchs)
Cancer query systems: delay-adjusted SEER incidence rates http://srab.cancer.gov/delay/canques.html. Accessed 2 Aug 2007
Midthune DN, Fay MP, Clegg LX, Feuer EJ (2005) Modeling reporting delays and reporting corrections in cancer registry data. J Am Stat Assoc 100(469):61–70
Breslow NE (1984) Extra-Poisson variation in log-linear models. Appl Stat 33(1):38–44
Toossi M (2002) A century of change: the U.S. labor force from 1950 to 2050. Mon Labor Rev 125:15–28
Zahm SH, Blair A (2003) Occupational cancer among women: where have we been and where are we going? Am J Ind Med 44(6):565–575
Donovan M, Tiwary CM, Axelrod D et al (2007) Personal care products that contain estrogens or xenoestrogens may increase breast cancer risk. Med Hypotheses 68(4):756–766
The health consequences of smoking: a report of the Surgeon General. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, Washington, DC, 2004
Lee DJ, Voti L, MacKinnon J et al (2008) Gender- and race-specific comparison of tobacco-associated cancer incidence trends in Florida with SEER regional cancer incidence data. Cancer Causes Control 19(7):711–723
Carbone A, Gloghini A, Serraino D, Spina M (2009) HIV-associated Hodgkin lymphoma. Curr Opin HIV AIDS 4(1):3–10
Jemal A, Thun MJ, Ries LAG et al (2008) Annual report to the nation on the status of cancer, 1975–2005, featuring trends in lung cancer, tobacco use, and tobacco control. J Natl Canc Inst 100(23):1672–1694
Acknowledgments
This research was supported in part by the Center for Environmental Oncology of the University of Pittsburgh Cancer Institute and the Intramural Research Program of the NIH, National Institute of Environmental Health Sciences. The authors appreciate the helpful comments provided by Dr. Walter Rogan and Dr. Grace Kissling.
Conflicts of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Appendix
Suppose cancer data (incidence or mortality) are cross-classified into Na age groups and Np time periods of equal width, thereby determining Nc birth cohorts. Assume cancer events (new cases or deaths) follow a Poisson distribution and consider the age-period-cohort (APC) model:
where ln[E(R ijk )] is the natural logarithm of the expected value of the cancer rate, R ijk , associated with the ith age group (i = 1,…,Na), jth time period (j = 1,…,Np), and kth birth cohort (k = 1,…,Nc). This full APC model includes an overall mean (μ) and separate main effects for age group (A i ), time period (P j ), and birth cohort (C k ). The relationship among these three temporal factors dictates that Nc = Na + Np − 1 and k = Na + j − i.
Using the approach of Dinse et al. [11] as originally proposed by Holford [10], we reparameterized the APC model in terms of trend lines and deviations from the trend lines. For each temporal factor (i.e., age, period, cohort), imagine fitting a straight line to the main effects and then representing each main effect as a point along that line plus the vertical distance (or deviation) from that line. Within this framework, the main effects in model (1) can be expressed as follows:
where \( \delta_{i}^{a} = \sum_{m = 1}^{{N^{a} - 1}} {H_{im}^{a} \theta_{m}^{a} } \), \( \delta_{j}^{p} = \sum_{m = 1}^{{N^{p} - 1}} {H_{jm}^{p} \theta_{m}^{p} } \), and \( \delta_{k}^{c} = \sum_{m = 1}^{{N^{c} - 1}} {H_{km}^{c} \theta_{m}^{c} } \). The β and θ terms are unknown regression parameters and the H terms are elements of design matrices of orthogonal polynomials (see Holford [10] for details). The first component in each of these three equations uses the slope parameter for age (βa), period (βp), or cohort (βc) to determine the ith, jth, or kth point along the appropriate trend line, respectively. Each second component represents a deviation from the appropriate trend line that is specifically associated with the ith age group (\( \delta_{i}^{a} \)), jth time period (\( \delta_{j}^{p} \)), or kth birth cohort (\( \delta_{k}^{c} \)), respectively.
Because of the interdependency of age, period, and cohort, some parameters in the full APC model, such as the three individual slopes (βa, βp, βc), are not uniquely estimable [10]. One function of the APC parameters that is estimable, however, is the sum of the period and cohort slopes, which is known as the drift and is denoted by D = βp + βc. For any age group, D summarizes the long-term linear temporal trend in the log cancer rates. From the drift, we can calculate the average annual percent change (AAPC):
which is the age-independent relative change in cancer rates associated with a temporal change of 1 year. Our APC analysis used 5-year age and time period groupings. Equation 5 divides D by 5 to rescale from 5-year time units to 1-year time units.
Analogously, the main effects (A i , P j , C k ) in the full APC model are not uniquely estimable, but their deviations from linearity (\( \delta_{i}^{a} \), \( \delta_{j}^{p} \), and \( \delta_{k}^{c} \)) are estimable. Deviations provide information about how well the log cancer rates are summarized by the trend lines and whether any discrepancies are attributable specifically to age, period, or cohort effects. Under model (1), the ratio of the expected cancer rates for a fixed age group i and consecutive time periods and birth cohorts is:
which does not appear to be uniquely estimable. However, substituting from Eqs. 3 and 4 for the period and cohort effects, this ratio can be rewritten in terms of estimable quantities:
Furthermore, taking the ratio of two adjacent expected rate ratios for a fixed age group i yields:
where the exponent in (8) is the sum of two second-order differences, one involving only period deviations and the other involving only cohort deviations. The constant-curvature model holds these second-order differences constant in j and k, respectively. Hence, the ratio of adjacent rate ratios in (8) reduces to a constant, which we call the constant curvature index (CCI). In this case, we write \( \delta_{j + 1}^{p} - 2\delta_{j}^{p} + \delta_{j - 1}^{p} \equiv \Updelta^{p} \) for j = 2,…,Np − 1 and \( \delta_{k + 1}^{c} - 2\delta_{k}^{c} + \delta_{k - 1}^{c} \equiv \Updelta^{c} \) for k = 2,…,Nc − 1, and we express the CCI in terms of the constants Δp and Δc:
Thus, the constant curvature index can be written as the product CCI = CCIp · CCIc, where the period component is CCIp = exp(Δp) and the cohort component is CCIc = exp(Δc). Unlike the AAPC, the CCI retains the 5-year time unit of analysis.
Rights and permissions
About this article
Cite this article
Han, YY., Dinse, G.E., Umbach, D.M. et al. Age-period-cohort analysis of cancers not related to tobacco, screening, or HIV: sex and race differences. Cancer Causes Control 21, 1227–1236 (2010). https://doi.org/10.1007/s10552-010-9550-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-010-9550-5