
Abstract
In metazoans apoptosis is a major physiological process of cell elimination during development and in tissue homeostasis and can be involved in pathological situations. In vitro, apoptosis proceeds through an execution phase during which cell dismantling is initiated, with or without fragmentation into apoptotic bodies, but with maintenance of a near-to-intact cytoplasmic membrane, followed by a transition to a necrotic cell elimination traditionally called “secondary necrosis”. Secondary necrosis involves activation of self-hydrolytic enzymes, and swelling of the cell or of the apoptotic bodies, generalized and irreparable damage to the cytoplasmic membrane, and culminates with cell disruption. In vivo, under normal conditions, the elimination of apoptosing cells or apoptotic bodies is by removal through engulfment by scavengers prompted by the exposure of engulfment signals during the execution phase of apoptosis; if this removal fails progression to secondary necrosis ensues as in the in vitro situation. In vivo secondary necrosis occurs when massive apoptosis overwhelms the available scavenging capacity, or when the scavenger mechanism is directly impaired, and may result in leakage of the cell contents with induction of tissue injury and inflammatory and autoimmune responses. Several disorders where secondary necrosis has been implicated as a pathogenic mechanism will be reviewed.
Similar content being viewed by others


Introduction
“Life is uncertain, death is certain”. All cells are doomed to die. Cell death processes can be passive or active. Passive cell death is the direct, acute killing of a cell by an exterior aggression damaging enough to produce irreversible alterations; these occur without the participation of the cell and can be prevented only by the absence of the aggression. This is the case, among others, of cell death due to exposure to high concentrations of detergents or antiseptics, extreme heat or repeated freeze-thawing, that is, situations without biological relevance. In this mode of cell death there is immediate, extensive and irreparable damage to the cytoplasmic membrane and this damage affects the membrane from without.
In contrast, active cell death is a suicidal process that is carried out by the doomed cell using molecules and pathways that are endogenous to the cell. The term “programmed cell death”, coined by Lockshin and Williams to qualify developmental cell death [1], has gained wide use to characterize active cell deaths. However, the term “programmed” has been used in two distinct senses to characterize either (i) cell death processes that occur at a precise local and time according to a developmental program (for example in morphogenesis) or (ii) cell deaths that, once triggered (as part of a developmental program or occasionally as in some pathologies), follow cell-intrinsic biochemical programs controlled by the doomed cell. Therefore, we will use the term “active” instead of “programmed” when referring to cell death processes that, once triggered, unroll following a course of biochemical events processed and controlled by the dying cell.
Cell death is followed by cell elimination. In multicellular animals, cell elimination is essential for development and homeostasis, and is mainly carried out by apoptosis. The initial report by Kerr, Wyllie and Currie, introducing the concept of apoptosis [2] was based on in vivo observations in mammalian tissues and described that process as comprising a terminal cell elimination stage through the removal of the apoptosing cell by phagocytosis and degradation by a scavenger cell. However, it was soon recognized by Kerr and collaborators that in vivo [3, 4] and in vitro [5, 6], when removal by scavengers does not occur, the apoptotic process continues until a transition to necrosis ensues leading to cell elimination by cell disruption. This terminal disruption of apoptotic cells was initially called “secondary degeneration” [5], a designation later changed to “secondary necrosis” [7]. This designation achieved widespread acceptance and is now part of the glossary of cell death terms, although it is prone to some confusion. Indeed, necroses that can be also labeled as secondary can occur in diverse situations; for example, necrosis following ischemia due to vascular occlusion has been frequently called secondary necrosis, as in necrotizing fasciitis.
Secondary necrosis was viewed in the initial reports as a separate process occurring after completion of apoptosis [5, 6] and, thus, it has frequently been called post-apoptotic necrosis. An alternative view is to consider that necrotic outcome as part of the apoptotic program of cell elimination, in which case it has been called late apoptosis.
Secondary necrosis also terminates the apoptotic process in eukaryotic unicellular organisms like yeasts [8, 9]. A terminal necrotic elimination can occur at the end of other active cell death processes besides apoptosis [10, 11]. Therefore, the term apoptotic secondary necrosis is used in this review to refer the terminal cell disruption that may follow apoptotic cell death.
After being initially seen as a mere biological curiosity, apoptotic secondary necrosis was soon recognized as an event with pathogenic relevance when occurring in multicellular animals. The pro-inflammatory and cytotoxic consequences of lysis of cells under secondary necrosis due to the lack of removal by scavengers have initially been repeatedly predicted or assumed, but supporting evidence for the pathogenic potential of that outcome of apoptosis has been progressively gathered as will be here reviewed.
Apoptosis as the prelude of secondary necrosis
Secondary necrosis is a process that affects cells under advanced apoptosis; thus, the characteristics of secondary necrotic cells are influenced by alterations previously occurred during the execution of apoptosis.
After the initial concept that apoptosis was the mechanism behind active cell death, advances in the knowledge in this area revealed that active cell death may assume several genetically defined programs (reviewed in Ref. [12]). In typical situations, these diverse programs dictate different phenotypes which can be used as a basis for the classification of active cell death modes [13, 14]. The presently known clear-cut forms of active cell death include, besides apoptosis, autophagic cell death [10, 15], primary necrosis (also known as programmed necrosis) [11, 16–18], mitotic catastrophe [19], and caspase 1-dependent pyroptosis [20]. These paradigmatic modes of cell death have been observed in multicellular organisms, but less clear-cut, intermediate or hybrid cell death modes have also been described as indicated by the use of terms as apoptosis-like or necrosis-like cell deaths [12], necrapoptosis [21] and necroptosis [22].
In multicellular organisms, apoptosis is a major physiological cell killing process used during embryonic morphogenesis and in adult life in tissue homeostasis and immune responses for the elimination of unnecessary, unwanted or dangerous cells [23, 24].
When a cell isolated from a metazoan and maintained in vitro responds to an apoptotic death stimulus it activates a sequence of molecular events [25] that proceeds through two phases which ultimately culminates in cell disruption [5, 25]. In the first phase, molecular alterations produce the classical apoptotic morphotype (see Table 1 and Figs. 1b, 2b and 4) that is used to identify this mode of cell death. During this phase the apoptosing cells may or may not fragment into apoptotic bodies, and, in contrast with necrosis, the membrane enveloping the apoptosing cells or the apoptotic bodies remains near-to-intact, that is, except for some structural alterations like externalization of phosphatidylserine and exposition of other “eat-me” signals for phagocytosis by scavengers, it is normal including in regards to selective permeability [7, 33, 34]. The terminal phase is secondary necrosis during which necrotic molecular alterations produce a new morphotype (see Table 1) which is more typical when there is no fragmentation into apoptotic bodies; this secondary necrotic morphotype is a mixture of alterations produced in the apoptotic phase (like nuclear fragmentation and intense chromatin condensation) and necrotic alterations (swelling of the cell and damage to the cytoplasmic membrane) [7]. Ultimately the cytoplasmic membrane ruptures and the cell (or the apoptotic bodies) is dismantled to cell debris (Fig. 1c, d). This experiment shows that the apoptotic death of an isolated cell, once triggered, is self-sufficient and leads to self-elimination by secondary necrosis.

Apoptotic cell death in vitro. Hemacolor staining of sea bass peritoneal phagocytes exposed in vitro to the apoptogenic exotoxin AIP56 of the gram-negative pathogen Photobacterium damselae ssp. piscicida [30]. (a) Normal phagocyte. (b) Phagocyte under apoptosis, showing cell rounding and shrinkage, nuclear fragmentation and intense chromatin condensation. (c) Phagocyte under apoptotic secondary necrosis, showing nuclear apoptotic changes (fragmentation and intense chromatin condensation) and a lysed cytoplasm. (d) A more advanced secondary necrosis with chromatolysis and cell swelling. Technical details in Ref. [30]

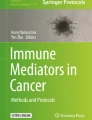
Apoptotic cell death in vivo. Transmission electron microscopy of peritoneal sea bass phagocytes that where induced to enter apoptotic death by the exotoxin AIP56 secreted by intraperitoneally injected Photobacterium damselae ssp. piscicida [31, 32]. (a) A normal looking phagocyte. (b) A phagocyte under apoptosis, showing cell shrinkage, loss of microvilli, nuclear fragmentation and intense chromatin condensation and a continuous cytoplasmic membrane. (c) A phagocyte under apoptotic secondary necrosis showing an apoptotic (hyper-condensed) nuclear fragment together with rupture of the cytoplasmic membrane and leakage of cell components. Technical details in Ref. [32]
When incorporated in the multicellular organism, that same cell will respond to an apoptotic death stimulus again by activating its endogenous apoptotic mechanism but the outcome may well be quite different from that occurring in vitro because now the cell is part of the social context of the multicellular organism [35]. Indeed, the apoptotic program triggers a mechanism for cell elimination that calls for the cooperation of a scavenger cell to engulf and digest by heterolysis the apoptosing cell before transition to secondary necrosis, that is, while the apoptosing cell still is enveloped by a near-to-intact membrane. This process of cell elimination, described in the initial report by Kerr, Wyllie and Currie as the second stage of apoptosis in mammals and as the physiological mechanism for elimination of apoptosing cells or apoptotic bodies [2] is activated in the in vitro setting but cannot operate because of the lack of the scavenger.
Biochemical events that are behind the apoptotic morphotype may include caspase activation, PARP-1 inactivation, mitochondrial permeability transition with loss of membrane potential (Δψ), release of AIF, EndoG or cytochrome c from the mitochondrial intermembrane space, moderate increased production of ROS, moderate cytosolic Ca2+ overload and internucleosomal DNA degradation (reviewed in Refs. [25, 36, 37]. There is proteolytic degradation of many substrates mainly effected by activated effector caspases [36] but caspase-independent effector mechanisms may also participate [38], and may have the participation of autophagy [39]. The degradative events occurring during the execution of apoptosis produce a partial cell dismantling which confers to apoptosis an autolytic character and is the basis of the apoptotic morphotype. This initial autolytic degradation is significantly increased when apoptosing cells are phagocytosed and heterolytically digested by scavengers or when apoptosis transits to secondary necrosis where further, extensive, autolytic degradation leads to cell disruption.
For the normal progress of the apoptotic pathways energy is required, and an initial increase in cytosolic ATP in apoptosing cells has been reported [40, 41]. ATP is required for cell shrinkage, bleb formation, caspase activation, enzymatic hydrolysis of macromolecules, chromatin condensation, DNA internucleosomal fragmentation, nuclear fragmentation, exposure of engulfment signals and apoptotic body formation (reviewed in Refs. [25, 37, 41, 42].
Apoptotic bodies may be formed during the degradation phase by the fragmentation of apoptosing cells as already described in the initial report of Kerr, Wyllie and Currie [2]. Although formation of apoptotic bodies is frequently considered as constant during apoptosis, in some otherwise typical apoptotic processes occurring in vitro or in vivo apoptotic bodies are not produced or are rare (see for example [6, 7, 26–28, 43, 44]), so that the elimination of apoptosing cells frequently affects non-fragmented cells. The non-fragmented, shrunken, apoptosing cell can be considered a single apoptotic body [45], as in the case of the so-called sunburn cells, apoptotic keratinocytes induced by UV irradiation of the skin [46]. Apoptotic bodies are produced while the apoptosing cell still has a near-to-normal cytoplasmic membrane and they are as well enveloped by a near-to-intact membrane [2, 47]. Like apoptosing cells, they express signals for engulfment and are phagocytosed by scavengers [2] or undergo secondary necrosis if not engulfed [7, 47].
In multicellular animals the timely removal of apoptosing cells through phagocytosis by scavengers is the clue for the physiological outcome of apoptosis because it prevents the occurrence of secondary necrosis [23, 48, 49]. In higher multicellular animals, phagocytosis is mainly accomplished by monocytes/macrophages and neutrophils, the professional phagocytes [50], which constitute up to 10–15% of cells in most mammalian tissues [23]. Typically, the professional scavenger of dying/dead cells is the macrophage [51, 52], which is located in all body territories and is highly phagocytic [53]. When macrophages are not available, for example due to a particular location of the dying/dead cells, neutrophils [54], or neighbor cells functioning as surrogate “amateur” phagocytes, may fulfill the role of removal of dying/dead cells; most cell types, including dendritic, epithelial, endothelial, and glomerular mesangial cells, fibroblasts, myocytes, and tumor cells, are able to perform this task [7, 49, 51, 52, 55]. This situation is the rule in simple multicellular animals, like Caenorhabditis elegans, where professional phagocytes are not present and apoptosing cells are removed by neighbor cells [56].
Although less efficiently than macrophages [49, 57–59], dendritic cells may engulf apoptosing cells, mainly when extensive apoptosis overwhelms the macrophage availability [60–62] or in territories where dendritic cells outnumber macrophages [63]. It has been reported that dendritic cells are more prone than macrophages to develop a pro-inflammatory response following the uptake of apoptosing or secondary necrotic cells [61, 62]. This point will be further discussed in ‘‘Pathogenic consequences of apoptotic secondary necrosis’’ section.
Like molecules involved in cell death processes, molecules involved in the removal by scavengers of dying/dead cells are present, and are in part similar, in worms, flies and mammals [64], indicating that such a clearance represents a crucial mechanism that has been conserved through evolution. Encounter of apoptosing cells with phagocytes may require attraction of phagocytes; specific attraction signals released by apoptosing cells in a caspase 3-dependent manner have been described [65, 66]. The recognition and engulfment of dying/dead cells by phagocytes involves the interaction between a number of molecules (reviewed in Refs. [67–70]). “Eat me” signals are exposed on the surface of apoptosing cells and are recognized by receptors on the surface of scavengers. The interactions between the engulfment signals and the receptors are facilitated by bridging molecules present in serum such as β2 glycoprotein, milk fat globule protein (MFG-E8), protein S, growth arrest-specific 6 (Gas6), thrombospondin, pentraxins and complement factors. This mechanism of attraction between apoptosing cells and scavengers is complemented by the loss by the apoptosing cells of expression of “don’t eat me” signals that normally prevent engulfment of living cells.
Much less is known about how scavengers recognize cells under active primary necrosis as compared to apoptosing cells, but it has been reported that some of the engulfment signals in necrosing cells are different from those exposed by apoptosing cells [68]. In this context, it is of note that many studies on this topic (and on the immunological effects of necrotic cells) used cells made necrotic by physical methods like heating, or exposure to detergents or fixatives. These methods produce passive necrotic cells with protein inactivation that consequently cannot be representative of cells dying in vivo due to active necrotic processes which induce proteolytic alterations and exposure of engulfment signals. It is therefore important that more studies be conducted on the process of recognition of necrosing cells by scavengers and on the pathogenic effects of necrosis using cells under active necrosis.
Elimination of apoptosing cells by a scavenger involves the degradation by the hydrolytic enzymes of the phagolysosomes of the scavenger (heterolysis). This heterolytic degradation superimposes on the autolysis ongoing in the apoptosing cell [2, 4]. Several results indicate that the role of macrophages in removal of apoptosing cells is not solely to eliminate cell corpses, but rather to degrade those cells to harmless and largely re-utilizable molecules; this dismantling can be extensive when the dying/dead cells are engulfed very early in the apoptotic process [71, 72]. Indeed, uptake of apoptosing cells can occur with different timings after death triggering, depending on the timing of exposition of surface engulfment signals and on the availability of scavengers. Therefore, the extension of the executed apoptotic curriculum can vary, manifesting different morphologies. Apoptosing cells can be engulfed so early that the typical morphological changes or DNA fragmentation have not yet occurred [73–75] which would explain why under physiological conditions cells with apoptotic indicators are rarely seen in tissues [7, 76]. The swift removal of apoptosing cells is particularly advantageous in embryogenesis.
There are important differences in the processes of removal of cells under apoptosis or under active necrosis: (i) Apoptosing and necrosing cells are phagocytosed by macrophages through different mechanisms [77, 78]. (ii) Engulfment of cells under active necrosis is delayed and quantitatively and kinetically less efficient as compared to the uptake of apoptosing cells [77, 79]. (iii) Engulfment of apoptosing cells by scavengers normally occurs before the transition to secondary necrosis, that is when the dying/dead cells or the apoptotic bodies still have a near-to-normal cytoplasmic membrane [7, 33] (Fig. 3). In contrast, engulfment of necrosing cells usually occurs after cytoplasmic membrane damage and cell rupture so that cell fragments are engulfed [77, 78, 80] (Fig. 3).

Schematic representation of the two cell elimination processes that can operate in active primary necrosis and apoptosis (heterolysis after removal by scavengers or cell burst due to autolysis). The cytoplasmic membrane of the cells under death processes is normal in the green area and damaged in the red area. A central issue is that, in apoptosis, in contrast with primary necrosis, the timely removal by scavengers of dying/dead cells is carried out before occurrence of damage to the cytoplasmic membrane. Leakage of cell contents is most extensive and involves large molecules when there is cell disruption (large blue arrows). See text in “Apoptotic secondary necrosis” section for details
Although the macrophage response to the phagocytosis of apoptosing cells may occasionally be pro-inflammatory (see discussion in Refs. [14, 52, 68], that phagocytosis typically fails to induce an inflammatory response [81] due to active inhibition of the release of pro-inflammatory mediators and to generation of anti-inflammatory factors such as transforming growth factor-beta (TGF-beta) and anti-inflammatory eicosanoids [82–84]. This contrasts with the effect of necrotic cell engulfment, which usually, but not always [77, 85], induces pro-inflammatory responses by the engulfing phagocytes [68, 69, 86, 87]. The prevailing view is that the delayed and deficient removal mechanism of cells under primary necrosis allows the persistence of leaky cells and necrotic debris which leads to activation of pro-inflammatory and immuno-stimulatory responses [11, 16] (see “Pathogenic consequences of apoptotic secondary necrosis” section). Necrotic cells may induce an inflammatory response not only by spilling their contents after lysis, but also by actively secreting inflammatory molecules, including cytokines (reviewed in Ref. [68]). However, there are reports of occurrence of extensive necrotic processes in vivo in the absence of important inflammatory responses [79, 80, 85, 88]. It is also of note that necrosis-associated inflammation, when not excessive, can be beneficial for the organism, for example during a protective immune response [17]. The removal by phagocytosis of cells under secondary necrosis will be discussed in “Pathogenic consequences of apoptotic secondary necrosis” section.
Central for the topic of this review is that, in multicellular animals, the physiological removal of apoptosing cells by scavengers may fail allowing the occurrence of secondary necrosis with potential pathogenic consequences. Failure of this process may be due to defects of the scavengers (insufficient number or functional incapacity) or of molecules involved in the recognition and engulfment of apoptosing cells, as will be reviewed later.
Apoptotic secondary necrosis
As already recognized in the initial reports on apoptosis [3, 4], when removal by scavengers fails in vivo, the apoptotic process fully unrolls and apoptosis transits to the self-elimination by secondary necrosis. A paradigmatic example is provided by apoptosis of cartilage chondrocytes; due to the avascular nature of articular cartilage and the lack of direct cell-cell contacts, apoptotic chondrocytes, induced for example in poly-arthritis [89], cannot be removed by scavenger cells and are eliminated by secondary necrosis [90]. Occurrence of in vivo secondary necrosis associated with pathology will be reviewed in “Pathogenic consequences of apoptotic secondary necrosis” section.
Contrary to the heterolytic degradation that dismantles apoptotic cells within scavengers, the hydrolytic processes of secondary necrosis involve autolytic enzymes. The available scant data regarding the molecular events in secondary necrosis suggest that this is an active necrotic process with biochemical and structural features common to those of active primary necrosis.
Recent advances in the knowledge of signaling and biochemical events in active primary necrosis are reviewed in Refs. [11, 17, 18, 91, 92]. During the degradation phase of active necrosis several biochemical alterations have been described including mitochondrial dysfunction, high production of ROS, serious ATP depletion, intense ionic imbalance, and activation of non-caspase proteases; these alterations ultimately converge in extensive lysosome rupture, which assumes a decisive role in active necrosis [93]. ATP depletion, ROS production and Ca2+ fluxes involve complex feedback and feed-forward interactive loops, some of them self-amplifying, as comprehensively reviewed by Brookes [94]. The important Ca2+ overload [95–97] induces enhanced activation of hydrolysing enzymes, including calpains [98], and leads to exaggerated energy consumption and impairment of energy production [99]; ATP depletion and activated calpains were shown to induce lysosome rupture [93, 100, 101], and released lysosomal cathepsins contribute to cytoplasmic membrane damage [102, 103], a hallmark of necrosis [7]. Thus, contrary to what happens in passive necrosis, cytoplasmic membrane damage in active necrosis is produced from within. This damage is due to the cumulative activity of hydrolytic enzymes and of ROS, and to serious energy failure; these events result in progressive membrane permeabilization to molecules of increasing size until the rupture of the membrane. This rupture is a consequence of the continuous cell swelling (oncosis or necrotic volume increase [104]) due to the maintenance within the cell of large molecules, including proteins and nucleic acids (Gibbs–Donnan effect [105–108]). Thus, the progressive deterioration of the cytoplasmic membrane of necrosing cells leads to initial leakage of small ions like K+, then leakage of small macromolecules and finally leakage of large macromolecules [105].
The essential events occurring in active primary necrosis, culminating in cytoplasmic membrane rupture, are likely to operate in secondary necrosis. As discussed, the development of apoptosis requires energy. When apoptosis progresses without engulfment of apoptosing cells, the progression eventually leads to a late depletion of the intracellular ATP pool [109–111] likely due to early ATP-consuming apoptotic reactions together with a late complete loss of mitochondrial function [109]. This endogenously originated late serious energy depletion has been considered the trigger for the transition from the end of a fully developed execution phase of apoptosis to secondary necrosis [21, 101, 112, 113]. It is known that serious ATP depletion provoked during early apoptosis induces a switch to necrosis (see below).
On the other hand, occurrence of secondary necrosis in caspase 3-dependent apoptosis induced by ultra-sounds has been found to be inhibited by the antioxidant N-acetyl-l-cysteine, suggesting the involvement of ROS in the transition to secondary necrosis [114].
During apoptosis, caspase 3 cleaves proteins involved in intracellular Ca2+ regulation including the Na+/Ca2+ exchanger, the inositol 1,4,5-trisphosphate receptors (IP3Rs), and the plasma membrane Ca2+ ATPases (PMCA) (reviewed in Ref. [115]). Caspase cleavage of the IP3R1 and of the Na+/Ca2+ exchanger has been shown to result in cytosolic Ca2+ overload [115]. On the other hand, two groups have shown that the PMCA 4b isoform is cleaved by caspase 3 during apoptosis [116, 117], but there is discrepancy regarding the reported functional consequence of that cleavage. While the results from Nicotera’s group suggest inactivation leading to a decreased rate of Ca2+ efflux from the cells and consequent cytosolic Ca2+ overload [116], the results form Enyedi’s group suggest that the cleavage product remains functionally active and would not contribute to Ca2+ overload [117–119]. An intense rise in intracellular Ca2+ was observed prior to the transition of apoptosis to secondary necrosis in prostate and bladder cancer cell lines [120], human B cell line FMO [121] or chicken B-lymphocytes [115]. In two of these studies [115, 121], the dramatic Ca2+ cytosolic overload was considered to be involved in that transition.
As in active primary necrosis, serious energy depletion, high Ca2+ cytosolic overload and high ROS production will lead to activation of calpains and to lysosome rupture, two events which have been suggested to participate in the cytoplasmic membrane damage in secondary necrosis [101, 122]. That lysosomal enzymes participate in secondary necrosis is also suggested by the observation that, in apoptosis induced in vitro in the epithelial cell line LLC-PK1 by S-(1,2-dichlorovinyl)-l-cysteine, inhibition of cathepsin B resulted in inhibition of secondary necrosis [123]. In support of this interpretation, recent results with caspase 3-associated apoptosis induced in Jurkat cells by treatment with anti-Fas showed that the terminal cell lysis due to secondary necrosis was concomitant with lysosome rupture [124].
Two frequently used assays to evaluate the cytoplasmic membrane condition during cell death processes are vital staining with the membrane impermeant propidium iodide (PI) and quantification of release of the intracellular enzyme lactate dehydrogenase (LDH). Permeability to PI (molecular mass about 0.67 kD) indicates a relatively initial cytoplasmic membrane damage [106, 108], while leakage of LDH (molecular mass about 140 kD) indicates terminal membrane rupture [107]. When apoptosing cells enter the secondary necrosis process those two assays change from negative to positive [33, 125, 126], revealing the ensuing of cytoplasmic membrane damage. Like in primary necrosis, in secondary necrosis PI-positivity precedes release of LDH and of other large molecules like activated caspase 3 (about 19 kD) (see Figs. 1D and 3C in Ref. [126]). As will be discussed in “Pathogenic consequences of apoptotic secondary necrosis” section, these observations are relevant in the context of the potential pathogenic role of secondary necrotic cells, since it is likely that only ruptured secondary necrotic cells will release large molecules like DNA, RNA and proteins including high mobility group box 1 (HMGB1) protein (about 30 kD) with inflammatory and immunogenic capacities.
The necrotic degradation in secondary necrosis affects cells that already were partially dismantled during the execution phase of the apoptotic process. The cell degradation during apoptosis involves proteolysis due to the activity of proteinases, mainly of effector caspases. During secondary necrosis there is additional proteolysis in a caspase-independent manner [127]. This late proteolysis, that contributes to the final dismantling of the apoptotic cell, may originate autoantigens that, when released by the lysing cell, send danger signals to the immune system and stimulate autoantibody responses [62, 128–130].
Serious energy failure provoked during early apoptosis by mechanisms external to the apoptotic process induces a switch to necrosis [131–133]. This switch occurs earlier than the spontaneous transition to secondary necrosis triggered by the endogenous failure of ATP associated with the complete progression of the apoptotic process. Indeed, the switch induced by ATP depletion from without interrupts the normal progression of apoptosis preventing the occurrence of biochemical events, like caspase activation, that produce the typical apoptotic morphotype. Consequently, cells under necrosis due to the switch apoptosis–necrosis do not exhibit the mixed secondary necrotic morphotype previously discussed (see Table 1 and Figs. 1c, 2c and 4) but rather that of active primary necrosis. This “switched necrosis” does not comply with the classical definition of apoptotic secondary necrosis discussed in the beginning of this review. However, it may lead to similar pathological consequences since the cells undergoing this switched necrosis autolyse and release cytotoxic or immunogenic molecules.

A group of enterocytes of sea bass under detachment-induced apoptosis (anoikis). Cells incubated ex vivo and viewed by phase contrast (panel a) and by fluorescence after double vital Hoechst 33342 and PI stainings (merged in panel b). Apoptosis is identified by the presence of fragmented and/or hyper-condensed, PI-negative nuclei in panel b. The cells labeled with asterisks in panel a are lysed as shown by the reduction in cytosol density; these cells have PI-positive fragmented and hyper-condensed nuclei (panel b), indicating that they are under apoptotic secondary necrosis. Reproduced from [134] with permission of the publisher
Apoptotic secondary necrosis was initially described in in vitro experiments [5, 6]. The frequent lack of consideration of the fact that induction of apoptosis in vitro (usually in the absence of scavengers) inevitably results in secondary necrosis can lead to misleading interpretations of induction of active primary necrosis, or of a switch from apoptosis to necrosis, when the actual event was the natural transition of an ongoing apoptosis to secondary necrosis. Confusion between the occurrence of active primary or secondary necrosis in vitro is particularly frequent when no kinetic studies are carried out, preventing the observation of apoptosis preceding secondary necrosis. The same problem arises when studying apoptosis of unicellular eukaryotic cells like yeasts because also in this case apoptosis is always followed by secondary necrosis [8, 9].
Identification of apoptotic secondary necrosis
Detailed morphological descriptions of apoptotic secondary necrosis are available [26, 27, 134].
Since typically secondary necrosis is a necrotic event affecting late apoptosing cells, the secondary necrotic morphotype (see Table 1) is characterized by the co-existence in the same cell of some apoptotic alterations (like nuclear fragmentation and/or intense chromatin condensation) and some necrotic alterations (like a damaged cytoplasmic membrane). As already discussed, before they are cleared by scavengers or enter secondary necrosis, apoptotic cells exclude membrane impermeant stains like PI [33] (it is of note that the exclusion of membrane impermeant stains is only observed when these stains are used in low concentrations and for short periods [135] as in the protocol in reference [136]). PI positivity in secondary necrotic cells can be detected after combined vital staining with Hoechst 33342/PI (see Fig. 4 and Ref. [134]). Also typical of apoptotic secondary necrotic cells is the association of nuclear apoptotic alterations and cytoplasmic membrane rupture detected by transmission electron microscopy (Fig. 2c), depicting the terminal stage of secondary necrosis. Particularly informative is the time-lapse observation by phase contrast and fluorescence microscopy of Hoechst 33342/PI stained preparations [134]. This continuous scrutiny of the same cell allows the observation of the apoptotic morphotype (with apoptotic nuclear alterations, cell shrinkage, blebbing, and production of apoptotic bodies (when it occurs) and PI-negativity) followed by entrance into the secondary necrotic process as indicated by the change to PI-positivity, followed by cell swelling with reduction in cytoplasm density (Fig. 4), chromatolysis, and finally cell burst.
Like LDH and other large molecules, activated caspases are released at the end of apoptotic secondary necrosis when membrane rupture occurs, while only procaspases are released in the case of cytolysis due to caspase-independent death processes [126]. Furthermore, the procaspases released by primary necrotic cells are not significantly processed extracellularly by proteolysis despite the presence of released proteases [126]. Therefore, when the cell death process has been characterized as caspase-dependent apoptosis, occurrence of relevant apoptotic secondary necrosis can be detected in vivo by the presence of increased levels of extracellular activated caspases which can be quantified in the blood [31, 137–139].
Non-pathogenic apoptotic secondary necrosis
Lack of removal by engulfment of apoptosing cells can occur in vivo without serious consequences. This is the case when those cells are shed into ducts or into territories topologically outside the organism (like the gut and airways lumen) where the chances of encountering or attracting scavengers are small but where release of cell contents is not critical.
For example, prostate apoptosing cells induced by castration detach and are shed in the lumina of the acini where they undergo secondary necrosis [3]. During the first days of involution of lactating breast after weaning, abundant apoptosis of epithelial cells occurs; many of these apoptosing cells are shed into the alveolar lumen [140, 141] and undergo secondary necrosis [140].
In a mechanism of clearance, neutrophils and eosinophils in lung tissue can be removed through egression across the epithelial lining into the airway lumen where they may undergo apoptosis with engulfment by scavengers or progress to secondary necrosis [142, 143]. These granulocytes or their remnants are eventually eliminated with airway mucus and expectoration.
Pathogenic consequences of apoptotic secondary necrosis
Introduction
In physiological situations, the apoptotic mode of cell elimination is useful since it is triggered when appropriate, is silent, induces a safe mechanism for cell disposal by scavengers, and, although spending energy, is economical in terms of re-utilization of the products of this disposal [2]. Implicit in that perspective of apoptosis in multicellular organisms is that “the individual cellular fate is sacrificed for the benefit of a higher order of life—the organism” [144]. However, this perspective of apoptosis as a physiological, and sometimes programmed, process is restrictive since this mode of cell elimination can be subverted, leading to pathological situations that are harmful to the organism where it occurs. Apoptosis turns pathological when the killed cells are necessary and functional, for example when pathogens evade phagocytic defense mechanisms by inducing apoptotic destruction of macrophages, neutrophils or both, or in neurodegenerative disorders with apoptotic elimination of functional neurons. Or, within the frame of this review, pathological apoptosis may also result when the timely elimination of apoptosing cells by scavengers fails in vivo and secondary necrosis ensues.
The acquisition during evolution of the apoptotic cell death process [145], with the inherent mechanism for the elimination of cell corpses through removal by scavengers before damage to the cytoplasmic membrane, represented a crucial step forward for multicellular organisms because it avoids the potentially dangerous secondary necrosis. However, the normally efficient and non-pathogenic mechanism of assisted cell elimination associated with apoptosis can be overridden in vivo in pathological situations with the occurrence of secondary necrosis. The constraint associated with the process of removal by scavengers is that it is not self-sufficient: depending on a functional scavenger cell, that process fails if this cell is not available despite exposition of engulfment signals, as is known to occur in several pathological situations to be reviewed below.
Failure of timely removal of apoptosing cells with occurrence of secondary necrosis may lead to two types of pathological consequences: (i) progress of secondary necrosis until cell disruption will result in leakage of cell contents which may be cytotoxic and induce tissue injury or (ii) secondary necrotic cells or their debris may be taken up by antigen presenting cells, mainly dendritic cells, and induce inflammation and autoimmunity. As discussed in “Apoptosis as the prelude of secondary necrosis” section, when macrophages fail to clear apoptosing cells, a second route can operate for the uptake using dendritic cells. Macrophages completely degrade ingested cells without antigen presentation, but when that uptake is by dendritic cells, these present antigens and activate the immune system, which may lead to autoimmunity [57, 58, 60, 146]. Phagosomes containing phagocytosed cells mature more rapidly in macrophage than in dendritic cells; in these cells, low levels of lysosomal proteases and a decreased ability to degrade internalized protein favors their ability to present antigen [69, 147].
Removal by scavengers of apoptotic secondary necrotic cells in vivo does not usually occur because those cells typically originate due to lack of functional scavengers or of molecules involved in the removal process. If engulfment does occur, for example because secondary necrosis resulted from delayed instead of absent clearance, or because dendritic cells replace the lacking macrophages as scavengers, the engulfment affects cells with damaged cytoplasmic membranes or even ruptured cells and involves mechanisms that would be similar to those operating with cells under active primary necrosis. It has been suggested that efficient removal of apoptosing cells versus deficient removal of primary or secondary necrosing cells depends on the presence of an intact or a damaged cytoplasmic membrane, respectively [77]. When injected into the peritoneal cavity of mice, cells under apoptotic secondary necrosis were found to be phagocytosed by macrophages [148]. Removal of secondary necrotic cells co-cultured with macrophages in vitro was found to be less efficient and slower than removal of apoptosing cells [77]. It is thus likely that, in the in vivo situations, if engulfment of cells under apoptotic secondary necrosis occurs, it would be a deficient process as in the case of primary necrotic cells. Moreover, as discussed in “Apoptosis as the prelude of secondary necrosis” section, phagocytosis of necrosing cells, in contrast to phagocytosis of apoptosing cells, usually results in pro-inflammatory and pro-immunogenic responses with potential to induce autoimmunity, as will be reviewed later.
Disruption of non-engulfed cells under apoptotic secondary necrosis may therefore ensue in vivo and it may aggravate the consequences of the generalized, irreparable cytoplasmic membrane damage that occurs during the secondary necrotic process previous to cell rupture, because it causes the additional release of larger molecules with higher cytotoxic or immunogenic potential. Release of toxic molecules like elastase, myeloperoxidase and HMGB1 protein from cells under secondary necrosis has been demonstrated [149–154]. Although some reports suggest that phagocytosis by macrophages of secondary necrotic cells, like phagocytosis of early apoptosing cells, is not pro-inflammatory [59, 86, 87, 155], there are several publications showing that engulfment of secondary necrotic cells may be pro-inflammatory and immunogenic [60, 62, 129, 156–160]. The discrepant results may be explained by the use of secondary necrotic cells at early (non-ruptured cytoplasmic membrane) or terminal (ruptured cytoplasmic membrane) phases and/or by the use of different types of engulfing cells (macrophages, dendritic cells or other cell types).
As it will be reviewed in this section, the available data furnishes compelling evidence indicating that extensive or persistent in vivo secondary necrosis may have relevant pathogenic consequences.
Several mechanisms may lead to relevant in vivo secondary necrosis [76]. One regards situations of induction of excessive apoptosis that overwhelms the available scavenging capacity; this may occur in hyper-inflammation associated or not with infection. Other possibility is when the scavenging capacity is directly impaired by intrinsic defects in the phagocytic function of scavengers or by extrinsic defects in signaling molecules involved in the engulfment process; in this case accumulation of apoptotic cells and transition to secondary necrosis may occur even in situations of normal levels of apoptosis. Observation of high numbers of apoptosing cells in tissues implies a deficiency in their removal [7, 161, 162] with the likely occurrence of secondary necrosis. Examples of pathological situations generated by these different ways of induction of secondary necrosis will be now reviewed.
Deficiency in the clearance of apoptosing cells due to extensive apoptosis occurs particularly in solid organs [163]. Secondary necrosis of hepatocytes resulting in severe hepatitis has been described in rodents with extensive hepatocyte apoptosis induced by LPS [164], Fas antibody [138, 165], galactosamine [166] or carbon tetrachloride [137]. Apoptotic secondary necrosis was also reported in brains subjected to focal ischemia [167], in hepatic [112] and renal [168] ischemia-reperfusion, in acute myocardial infarction [169, 170], and in other heart pathologies [171].
Failure of removal of cells that entered an apoptotic process can also occur in vivo because of lack of exposure of engulfment signals when the ongoing apoptotic process is interrupted by lack of activation of effector caspases before the caspase-dependent exposure of engulfment signals on the apoptosing cell [172, 173]. This interruption can be induced by impairment of energy metabolism [131–133], by defects due to genetic alterations or by generation of inhibitors in injured areas [173], and, as already discussed, leads to a switch to necrosis. These non-cleared, necrosing cells undergo lysis that may have pathogenic implications [174] as in the case of apoptotic secondary necrosis. The switch apoptosis–necrosis has been reported in several ischemic pathologies including in the brain [173–175] and heart [170, 176]. ATP dependence of apoptosis and (almost) independence of active necrosis [37, 40, 177] might explain the frequent appearance of necrotic and apoptotic cells in pathological areas in vivo, such as the center of solid tumors and ischemic regions in solid organs; indeed, limitation of blood flow in those areas leads to ATP exhaustion due to insufficient oxygenation and reduced glycolysis by lack of glucose [178] and may result in the switch apoptosis–necrosis.
In neurodegenerative disorders there is an increased rate of neuronal apoptosis [179]. As in other pathologies discussed above, this apoptosis may be blocked and switched to necrosis [173], again with possible pathogenic implications.
Secondary necrosis of monocytes/macrophages, eosinophils and neutrophils in acute and chronic inflammation
Tissue injury due to secondary necrosis of apoptosing cells may be particularly serious when it involves cells rich in cytotoxic molecules like monocytes/macrophages, eosinophils and mainly neutrophils, in situations of intense inflammation.
In the protective inflammatory response there is migration of neutrophils from the reserve pools to infectious and noninfectious inflammatory foci, where they accumulate in large numbers for in situ elimination of invading microorganisms or damaged tissues [180]. For these activities, neutrophils use phagocytosis and are stimulated to release effector molecules upon exposure to various cytokines and chemoattractants [181]. Neutrophils are very rich in inflammatory mediators and in proteases and oxidants which, if released in high amounts, can damage many types of cells, with the potential to produce tissue injury [182–184]. Released neutrophil contents also induce the secretion of pro-inflammatory cytokines and chemokines which may amplify leukocyte infiltration and associated tissue injury [185, 186]. Release of noxious neutrophil components may occur during neutrophil degranulation in inflammatory foci and after lysis due to apoptotic secondary necrosis.
Under normal conditions, neutrophil activities at inflammatory foci are tightly controlled. Mobilization of neutrophil cytoplasmic granules and secretory vesicles is regulated, minimizing the risk of externalization of excessive amounts of cytotoxic molecules [187]. Additionally, under physiological conditions, neutrophil cytotoxic proteases, including elastase, one of the most tissue destructive enzymes known [185], have their potentially dangerous activity tightly regulated by endogenous protease inhibitors [188]. Moreover, neutrophils have a short lifespan and are constitutively programmed to undergo apoptosis, which induces the exposure of engulfment signals and leads to their rapid recognition and removal by macrophages; this limits their pro-inflammatory and tissue injury potential and leads to resolution of inflammation with restitution of tissue homeostasis soon after the neutrophils have accomplished their task [76, 189, 190]. Pneumococcal pneumonia is a paradigm for complete resolution of inflammation without relevant subsequent lung injury indicating that, in some situations, extensive neutrophil accumulation can be adequately resolved [76]. Neutrophil apoptosis with timely removal of apoptosing neutrophils by lung macrophages was shown to be a mechanism for that resolution in a murine model of pneumococcal pneumonia [191]. However, this control of neutrophil activity and physiological resolution of inflammation by clearance of apoptotic neutrophils can fail and release of cytotoxic components by neutrophils accumulated at inflammatory foci can occur with the potential to produce collateral tissue damage; for instance, elimination of alveolar macrophages in the above model of pneumococcal pneumonia affected the clearance of accumulated neutrophils and resulted in extensive apoptotic secondary necrosis of neutrophils and in an exaggerated lung inflammation and increased lethality [191].
Several mechanisms can delay neutrophil apoptosis at inflammatory foci as has been observed in acute and chronic inflammatory diseases [192, 193]. This delay extends the time frame of neutrophil intervention but at the same time increases the chances of tissue injury. When accumulation of activated neutrophils at the inflammatory foci is massive, as is the case in several diseases, release of cytotoxic neutrophil molecules due to degranulation or lysis can be extensive [149, 150], overcoming the activity of the endogenous inhibitors [181, 188, 194]. Consequently, tissue injury ensues [195–197]. Removal by scavengers of accumulated apoptosing neutrophils can be deficient leading to neutrophil secondary necrosis. This occurs when neutrophil accumulation is massive and disproportionate compared to the availability of scavengers or when neutrophil apoptosis is accelerated by microbial products [198, 199]. Impairment of scavenger macrophages by bacterial products [31] or by functional defects (see later) also causes excessive neutrophil secondary necrosis.
The bypass of the balanced, physiological control of neutrophil pro-inflammatory activities due to extensive degranulation or secondary necrosis switches to pathogenic a beneficial defense mechanism. Neutrophil-mediated tissue injury can affect several organs like the liver [200, 201], the brain [202, 203], and the lung (see below).
A variety of severe infectious and noninfectious insults can result in the systemic inflammatory response syndrome (SIRS) [204]. Frequent complications of SIRS are the development of acute lung injury (ALI) and its more severe form acute respiratory distress syndrome (ARDS), and of multiple organ dysfunction syndrome (MODS) [205, 206]. Neutrophil accumulation has been associated with the above serious clinical situations [206], and released phagocyte proteinases have been implicated in the development of MODS [207].
Severe ALI with extensive accumulation of neutrophils can complicate human and experimental infection by the most virulent strains of influenza virus, including H1N1 [208] and H5N1 [209, 210]. However, no studies on the possible occurrence of neutrophil secondary necrosis in these infections have been conducted.
In patients with chronic lung inflammatory disorders like obstructive pulmonary disease (COPD) [211, 212], emphysema [213], chronic bronchitis [214], severe asthma [215, 216] or cystic fibrosis [217] there is accumulation of leukocytes including high numbers of neutrophils; there is evidence that these granulocytes release excessive amounts of proteinases including elastase [218, 219], a variety of inflammatory cytokines, and reactive oxygen species [212], which may cause airway tissue injury. Released proteinases overcome the activity of natural anti-proteases [194] and impair the anti-microbial activity of neutrophils [220]. Besides egression to the airway lumen [142, 143], an efficient mechanism for removal of neutrophils accumulated in the inflamed lung is through neutrophil apoptosis and removal by macrophages [76, 191]. Alveolar macrophages from patients with COPD are deficient in the capacity to engulf apoptotic cells [221], deficiency that is aggravated by smoking [222]. This clearance defect contributes to the accumulation of apoptotic cells in the lungs of COPD patients and in animal models of COPD [223], and the occurrence of pathogenic neutrophil apoptotic secondary necrosis associated with lung neutrophil accumulation has been considered in chronic lung inflammatory diseases including COPD and cystic fibrosis [186, 219, 220]. Secondary necrosis of neutrophils was also implicated in human [198, 199] and murine [224] lung infections by gram-negatives and in a mouse model of lung inflammation induced by nasal instillation of LPS [225, 226].
In accordance with a role of released neutrophil cytotoxic molecules in the above reviewed situations, the level of plasma neutrophil elastase or of products of elastase activity were found to be significantly elevated in patients with SIRS and even more when this was complicated with ALI/ARDS [227, 228]. Active neutrophil elastase was also detected in increased levels in the blood of fish with massive neutrophil accumulation and neutrophil apoptotic secondary necrosis in advanced septicemic pasteurellosis [31].
Liu et al. [149] showed that neutrophils undergoing apoptotic secondary necrosis release active elastase with cytotoxic activity, indicating that this potent proteinase is not destroyed by the apoptotic and secondary necrotic proteolysis and directly demonstrating that neutrophil apoptotic secondary necrosis is prone to induce tissue damage. Moreover, topical or systemic administration of neutrophil elastase produced lung injury in rodents [185]. There is evidence in cystic fibrosis that neutrophil elastase, released by accumulated neutrophils possibly through apoptotic secondary necrosis, can impair apoptotic cell clearance [229] thus leading to a vicious circle that promotes further neutrophil secondary necrosis.
The effect of elastase inhibitors has been investigated in several situations with lung hyper inflammation, and some reports described beneficial results in patients with ALI/ARDS or in rodent models of ALI further supporting the pathogenic role of released elastase (see for example [230–232] and references herein).
Accumulation of eosinophils in airways occurs in patients with asthma or COPD (reviewed in Ref. [143]), and secondary necrosis of these leukocytes has been found in airways in patients with asthma [143] and in lung tissue of mouse models of the disease [233]. Eosinophil granules contain cytotoxic molecules [234] and apoptotic secondary necrosis of eosinophils was shown to induce inflammatory responses [156].
Although to a lesser degree as compared with neutrophils and eosinophils, monocytes/macrophages also contain tissue-damaging molecules including several proteases [235], which are released upon cell disruption due to secondary necrosis. Pathogenic macrophage secondary necrosis has been described in several situations including infection [31]. Besides inducing pro-inflammatory responses and tissue injury, macrophage secondary necrosis is a self-amplifying process with accumulation of apoptotic cells and further secondary necrosis because macrophages are the main scavenger cell [31].
Secondary necrosis in bacterial infection
Acute fish pasteurellosis is a lethal septicemic infection due to Photobacterium damselae ssp. piscicida (Phdp) and characterized by massive extracellular multiplication of the pathogen with extensive tissue necrosis [31]. One mechanism of the necrotic alterations typical of the advanced phase of this septicemia is systemic secondary necrosis of accumulated neutrophils and macrophages induced by an apoptogenic exotoxin (AIP56) secreted by virulent Phdp [30, 31]. The AIP56-induced fish phagocyte apoptosis involves activation of caspase 8, 9 and 3, and mitochondrial dysfunction with loss of Δψm and cytochrome c translocation to the cytosol [30, 31, 236] (C. Costa-Ramos et al. unpublished results). That the AIP56-induced phagocyte apoptosis proceeds to secondary necrosis and cytolysis is directly demonstrated by the occurrence of lysing phagocytes with apoptotic nuclear alterations in advanced infection (Fig. 2c; see also Fig. 3b, c in Ref. [32]). The simultaneous apoptotic destruction of macrophages and neutrophils by AIP56 leads to reduction in the number of available phagocytes that accumulated during the initial phase of the infection and efficient evasion of the pathogen from the host phagocytic defense; moreover, that destruction seriously decreases the host capacity to clear apoptosing cells. This phagocyte destruction has additional pathogenic consequences for the host: AIP56 exotoxin secreted by Phdp in infected fish is systemically distributed and induces disseminated phagocyte apoptosis that proceeds to secondary necrosis with extensive lysis of the phagocytes and release of cytotoxic molecules including neutrophil elastase [31]. Two concurrent mechanisms operate in the induction of the secondary necrotic outcome of the apoptotic process induced in phagocytes by AIP56: first, the exotoxin-induced phagocyte apoptosis is extensive leading to the production of great numbers of apoptosing leukocytes and, most importantly, it affects the principal scavenger cell, the macrophage, thus impairing the capacity to clear apoptosing cells by a self-amplifying process. This is an example of cell elimination adding more pathogenic consequences to those associated with the loss of function accompanying cell death. The “clever” nature of this pathogenicity mechanism is that it uses the intrinsic apoptotic machinery of the host cells, which is put at work by the pathogen to its own advantage.
Extensive phagocyte secondary necrosis was also described in the skin of mice with experimental infection by Mycobacterium ulcerans [237]. This pathogen, agent of the human disease Buruli ulcer, secretes an apoptogenic exotoxin, mycolactone, which is a key virulence factor [238]. As in fish pasteurellosis, the secondary necrosis observed in M. ulcerans infection was considered as resulting from the mycolactone-induced apoptotic destruction of both neutrophils and macrophages and to contribute to the tissue necrosis typical of this mycobacteriosis [237].
Other acute and serious infections with necrotic lesions and destruction of host phagocytes have been reported. For example, septicemic plague is a rapidly fatal septicemia, with massive accumulations of extracellular Yersinia pestis and occurrence of apoptotic cell destruction with cell lysis and tissue necrosis [239]. The finding that in septicemic plague, Y. pestis targets macrophages and neutrophils [240] suggests the possibility of occurrence of apoptotic secondary necrosis of phagocytes as in acute fish pasteurellosis, but such a possibility has not been assessed.
In a mouse model of lung infection by pyocyanin-producing Pseudomonas aeruginosa with extensive pulmonary accumulation of neutrophils and occurrence of neutrophil apoptotic secondary necrosis, a defect in the macrophage phagocytosis of apoptosing cells was recently described [224]; this defect was shown to be mediated by a non-apoptogenic effect of pyocyanin on macrophage phagocytic function.
In vivo studies on the role of apoptotic secondary necrosis of macrophages and neutrophils in the pathogenesis of infectious diseases have been neglected. New in vivo studies on bacteria-induced apoptotic phagocyte destruction may well reveal other situations where the pathogens use virulence mechanisms based on the induction of apoptotic secondary necrosis as in acute fish pasteurellosis and Buruli ulcer. In particular, infections caused by bacteria that, like Phdp and M. ulcerans, are known to produce apoptogenic molecules that target host phagocytes [241, 242], should be studied under this perspective.
Secondary necrosis in autoimmune diseases
Another possible consequence of in vivo occurrence of secondary necrosis due to increased rates of apoptosis [243, 244] and, mainly, failure of clearance of apoptotic cells is induction of autoimmune responses associated with disease. Several factors have been implicated in the pathogenesis of autoimmune disorders, including altered apoptosis [245]. Although autoimmunity may not follow impaired clearance of apoptosing cells [70, 246, 247], many studies show that such an impairment may result in immunogenicity and autoimmune disorders. There is a large body of evidence for the existence of a deficiency in clearance of apoptotic cells in autoimmune disorders including systemic lupus erythematosus (SLE), both in mouse models [61, 248] and in humans [58, 129, 244, 249–253]. Several genetically modified mice with defective apoptotic cell clearance have been developed and most of them show signs of autoimmune disease [52, 159, 254–256]. The defect in clearance of apoptosing cells in SLE and likely in other autoimmune disorders may have several mechanisms, including intrinsic impairment of engulfment capacity of phagocytes combined with extrinsic defects in bridging molecules involved in the recognition and engulfment of apoptosing cells by scavengers, like complement factors [61, 129, 253, 257, 258].
Apoptosis and secondary necrosis of neutrophils from blood of patients with SLE cultivated in vitro were found to be increased as compared to neutrophils from controls; moreover, a poor ability of macrophages from patients with SLE to phagocytose apoptotic neutrophils was observed [251]. Although an alternative has been proposed [87], apoptotic secondary necrosis has been implicated in the pathogenesis of autoimmune disorders including SLE through the release of autoantigens and cytotoxic molecules which induce pro-inflammatory and autoimmune responses [48, 62, 129, 159, 244, 259].
One important molecule involved in cytolysis-associated pro-inflammatory situations is HMGB1 protein, a prototypical alarmin [260]. This non-histone nuclear protein with a role in transcriptional regulation, functions as a potent pro-inflammatory cytokine when released in the extracellular space [261]. This protein is released during primary necrosis [262] and, contrary to initial reports, was found to be also released during secondary necrosis of several cell types [11, 151–154] and has been considered to participate in the pathogenesis of autoimmune diseases [151, 152]. HMGB1 is a protein of about 30 kD, and its release during secondary necrosis follows a kinetics similar to that of LDH release [152, 154], suggesting that progress of secondary necrosis until cell lysis is required for its externalization (see in “Apoptotic secondary necrosis” section discussion on membrane damage in secondary necrosis).
Autoantigens cleaved during the execution phase of apoptosis [263] undergo an additional wave of caspase-independent proteolysis during secondary necrosis, with the production of lower molecular weight products [127]. If released during secondary necrosis, these products might induce inflammation and stimulate pathogenic autoimmune responses [127].
Nucleosomes produced during the apoptotic death process by internucleosomal DNA degradation can be released when secondary necrosis occurs [244]. Nucleosomes are present in increased amounts in the circulation of patients with SLE and are targets of anti-DNA and anti-histone autoantibodies (reviewed in Ref. [257]). Serum levels of nucleosomes were found to be increased in various autoimmune diseases besides SLE [139]; the fact that blood caspase levels were increased together with nucleosomes in those diseases, favors the interpretation that apoptotic secondary necrosis is involved in the release of nucleosomes. Autoantigens in SLE patients are composed of or are intimately associated with RNA and DNA sequences that are endogenous ligands, respectively, for toll-like receptor (TLR) 7 and/or TLR9 present in plasmacytoid dendritic cells and B lymphocytes, contributing to autoimmune disease [159, 264, 265]. TLR9 activation by DNA-containing immune complexes was found to require an interaction of the complexes with HMGB1 [265].
Conclusions
Active suicidal death programs are intrinsic to cells in unicellular and multicellular organisms. Activation of these programs not only kills cells but additionally promotes mechanisms for elimination of the dying/dead cells. In multicellular animals, cells under apoptotic death can be eliminated by two processes with contrasting physiopathological consequences. One is the safe, physiological clearance by phagocytosis of the dying/dead cell or of apoptotic bodies through the timely assistance of a partner cell (the scavenger); this intervention of the scavenger removes the apoptosing cells or the apoptotic bodies while they still have a near-to-intact cytoplasmic membrane thus preventing leakage of dangerous molecules. However, this physiologically convenient mechanism is not self-sufficient because it depends on the participation of other cell and can be overridden in vivo when the scavenging mechanism fails. In this situation cell elimination is by transition of full-blown apoptosis to secondary necrosis that leads to cytoplasmic membrane damage and cell disintegration. This has potential pathogenic consequences and available data provides evidence suggesting that secondary necrosis is implicated in the pathogenesis of several diseases including autoimmune and neurodegenerative disorders, ischemia, and infection. The pathogenic consequences of extensive or persistent apoptotic secondary necrosis result from (i) the leakage of cytotoxic molecules (mainly when involving neutrophils) that induce tissue injury and pro-inflammatory responses; (ii) the uptake by macrophages and dendritic cells of secondary necrotic cell debris and released autoantigens, which may be pro-inflammatory and immunogenic. Apoptotic secondary necrosis may therefore produce acute and chronic pathology, thus being a mechanism for apoptosis turning pathogenic. It is important to recognize that cell disruption due to a necrotic process can be an outcome of apoptosis in vivo so that pathological consequences of this outcome may be inhibitable by anti-apoptotic interventions, prompting the use of (and research on) therapeutic interventions based on anti-apoptotic drugs. Contrasting with the available extensive studies on apoptosis and on the clearance of apoptosing cells by scavengers, the study of apoptotic secondary necrosis has been largely neglected and is much needed to better understand the full potential of this outcome of apoptosis in promotion of pathology.
References
Lockshin RA, Williams CM (1965) Programmed cell death. I. Cytology of degeneration in the intersegmental muscles of the Pernyi Silkmoth. J Insect Physiol 11:123–133
Kerr JF, Wyllie AH, Currie AR (1972) Apoptosis: a basic biological phenomenon with wide-ranging implications in tissue kinetics. Br J Cancer 26:239–257
Kerr JF, Searle J (1973) Deletion of cells by apoptosis during castration-induced involution of the rat prostate. Virchows Arch 13:87–102
Searle J, Lawson TA, Abbott PJ, Harmon B, Kerr JFR (1975) An electron-microscopic study of the mode of cell death induced by cancer-chemotherapeutic agents in populations of proliferating and neoplastic cells. J Pathol 116:129–138
Don MM, Ablett G, Bishop CJ et al (1977) Death of cells by apoptosis following attachment of specifically allergized lymphocytes in vitro. Aust J Exp Biol Med Sci 55:407–417
Robertson AM, Bird CC, Waddell AW, Currie AR (1978) Morphological aspects of glucocorticoid-induced cell death in human lymphoblastoid cells. J Pathol 126:181–187
Wyllie AH, Kerr JF, Currie AR (1980) Cell death: the significance of apoptosis. Int Rev Cytol 68:251–306
Silva RD, Sotoca R, Johansson B et al (2005) Hyperosmotic stress induces metacaspase- and mitochondria-dependent apoptosis in Saccharomyces cerevisiae. Mol Microbiol 58:824–834
Ludovico P, Madeo F, Silva M (2005) Yeast programmed cell death: an intricate puzzle. IUBMB Life 57:129–135
Bursch W (2001) The autophagosomal-lysosomal compartment in programmed cell death. Cell Death Differ 8:569–581
Festjens N, Vanden Berghe T, Vandenabeele P (2006) Necrosis, a well-orchestrated form of cell demise: signalling cascades, important mediators and concomitant immune response. Biochim Biophys Acta 1757:1371–1387
Leist M, Jaattela M (2001) Four deaths and a funeral: from caspases to alternative mechanisms. Nat Rev Mol Cell Biol 2:589–598
Kroemer G, El-Deiry WS, Golstein P et al (2005) Classification of cell death: recommendations of the Nomenclature Committee on Cell Death. Cell Death Differ 12(Suppl):1463–1467
Galluzzi L, Maiuri MC, Vitale I et al (2007) Cell death modalities: classification and pathophysiological implications. Cell Death Differ 14:1237–1243
Gozuacik D, Kimchi A (2007) Autophagy and cell death. Curr Top Dev Biol 78:217–245
Proskuryakov SY, Konoplyannikov AG, Gabai VL (2003) Necrosis: a specific form of programmed cell death? Exp Cell Res 283:1–16
Zong WX, Thompson CB (2006) Necrotic death as a cell fate. Genes Dev 20:1–15
Golstein P, Kroemer G (2007) Cell death by necrosis: towards a molecular definition. Trends Biochem Sci 32:37–43
Castedo M, Perfettini JL, Roumier T, Andreau K, Medema R, Kroemer G (2004) Cell death by mitotic catastrophe: a molecular definition. Oncogene 23:2825–2837
Fink SL, Cookson BT (2007) Pyroptosis and host cell death responses during Salmonella infection. Cell Microbiol 9:2562–2570
Lemasters JJV (1999) Necrapoptosis and the mitochondrial permeability transition: shared pathways to necrosis and apoptosis. Am J Physiol 276:G1–G6
Degterev A, Huang Z, Boyce M et al (2005) Chemical inhibitor of nonapoptotic cell death with therapeutic potential for ischemic brain injury. Nat Chem Biol 1:112–119
Henson PM, Hume DA (2006) Apoptotic cell removal in development and tissue homeostasis. Trends Immunol 27:244–250
Domingos PM, Steller H (2007) Pathways regulating apoptosis during patterning and development. Curr Opin Genet Devel 17:294–299
Kroemer G, Petit P, Zamzami N, Vayssiere JL, Mignotte B (1995) The biochemistry of programmed cell death. FASEB J 9:1277–1287
Payne CM, Glasser L, Tischler ME et al (1994) Programmed cell death of the normal human neutrophil: an in vitro model of senescence. Microsc Res Tech 28:327–344
Hebert MJ, Takano T, Holthofer H, Brady HR (1996) Sequential morphologic events during apoptosis of human neutrophils. Modulation by lipoxygenase-derived eicosanoids. J Immunol 157:3105–3115
Hacker G (2000) The morphology of apoptosis. Cell Tissue Res 301:5–17
Skulachev VP, Bakeeva LE, Chernyak BV et al (2004) Thread-grain transition of mitochondrial reticulum as a step of mitoptosis and apoptosis. Mol Cell Biochem 256–257:341–358
do Vale A, Silva MT, dos Santos NM et al (2005) AIP56, a novel plasmid-encoded virulence factor of Photobacterium damselae subsp. piscicida with apoptogenic activity against sea bass macrophages and neutrophils. Mol Microbiol 58:1025–1038
do Vale A, Costa-Ramos C, Silva A et al (2007) Systemic macrophage and neutrophil destruction by secondary necrosis induced by a bacterial exotoxin in a Gram-negative septicaemia. Cell Microbiol 9:988–1003
do Vale A, Marques F, Silva MT (2003) Apoptosis of sea bass (Dicentrarchus labrax L.) neutrophils and macrophages induced by experimental infection with Photobacterium damselae subsp. piscicida. Fish Shellfish Immunol 15:129–144
Darzynkiewicz Z, Bruno S, Del Bino G et al (1992) Features of apoptotic cells measured by flow cytometry. Cytometry 13:795–808
Zamai L, Canonico B, Luchetti F et al (2001) Supravital exposure to propidium iodide identifies apoptosis on adherent cells. Cytometry 44:57–64
Raff MC (1992) Social controls on cell survival and cell death. Nature 356:397–400
Hengartner MO (2000) The biochemistry of apoptosis. Nature 407:770–776
Skulachev VP (2006) Bioenergetic aspects of apoptosis, necrosis, mitoptosis. Apoptosis 11:473–485
Hail N Jr, Carter BZ, Konopleva M, Andreeff M (2006) Apoptosis effector mechanisms: a requiem performed in different keys. Apoptosis 11:889–904
Maiuri MC, Zalckvar E, Kimchi A, Kroemer G (2007) Self-eating and self-killing: crosstalk between autophagy and apoptosis. Nat Rev Mol Cell Biol 8:741–752
Atlante A, Giannattasio S, Bobba A et al (2005) An increase in the ATP levels occurs in cerebellar granule cells en route to apoptosis in which ATP derives from both oxidative phosphorylation and anaerobic glycolysis. Biochim Biophys Acta 1708:50–62
Zamaraeva MV, Sabirov RZ, Manabe K, Okada Y (2007) Ca(2+)-dependent glycolysis activation mediates apoptotic ATP elevation in HeLa cells. Biochem Biophys Res Commun 363:687–693
Nicotera P, Melino G (2004) Regulation of the apoptosis–necrosis switch. Oncogene 23:2757–2765
Majno G, Joris I (1995) Apoptosis, oncosis, and necrosis. An overview of cell death. Am J Pathol 146:3–15
Sladek Z, Rysanek D (2005) Tissue pool neutrophils of the bovine mammary gland: ultrastructural features during in vitro senescence. Anat Histol Embryol 34:159–166
Orlando KA, Stone NL, Pittman RN (2006) Rho kinase regulates fragmentation and phagocytosis of apoptotic cells. Exp Cell Res 312:5–15
Sheehan JM, Young AR (2002) The sunburn cell revisited: an update on mechanistic aspects. Photochem Photobiol Sci 1:365–377
Sheridan JW, Bishop CJ, Simmons RJ (1981) Biophysical and morphological correlates of kinetic change and death in a starved human melanoma cell line. J Cell Sci 49:119–137
Savill J, Fadok V (2000) Corpse clearance defines the meaning of cell death. Nature 407:784–788
Fadok VA (1999) Clearance: the last and often forgotten stage of apoptosis. J Mammary Gland Biol Neoplasia 4:203–211
Rabinovitch M (1995) Professional and non-professional phagocytes: an introduction. Trends Cell Biol 5:85–87
Parnaik R, Raff MC, Scholes J (2000) Differences between the clearance of apoptotic cells by professional and non-professional phagocytes. Curr Biol 10:857–860
Gregory CD, Devitt A (2004) The macrophage and the apoptotic cell: an innate immune interaction viewed simplistically? Immunology 113:1–14
van Furth R (1981) Current view of the mononuclear phagocyte system. Haematol Blood Transfus 27:3–10
Rydell-Tormanen K, Uller L, Erjefalt JS (2006) Neutrophil cannibalism–a back up when the macrophage clearance system is insufficient. Respir Res 7:143
Wiegand UK, Corbach S, Prescott AR, Savill J, Spruce BA (2001) The trigger to cell death determines the efficiency with which dying cells are cleared by neighbours. Cell Death Differ 8:734–746
Mangahas PM, Zhou Z (2005) Clearance of apoptotic cells in Caenorhabditis elegans. Semin Cell Dev Biol 16:295–306
Albert ML, Sauter B, Bhardwaj N (1998) Dendritic cells acquire antigen from apoptotic cells and induce class I-restricted CTLs. Nature 392:86–89
Rovere P, Sabbadini MG, Fazzini F et al (2000) Remnants of suicidal cells fostering systemic autoaggression. Apoptosis in the origin and maintenance of autoimmunity. Arthritis Rheum 43:1663–1672
Sauter B, Albert ML, Francisco L, Larsson M, Somersan S, Bhardwaj N (2000) Consequences of cell death: exposure to necrotic tumor cells, but not primary tissue cells or apoptotic cells, induces the maturation of immunostimulatory dendritic cells. J Exp Med 191:423–434
Rovere P, Vallinoto C, Bondanza A et al (1998) Bystander apoptosis triggers dendritic cell maturation and antigen-presenting function. J Immunol 161:4467–4471
Taylor PR, Carugati A, Fadok VA et al (2000) A hierarchical role for classical pathway complement proteins in the clearance of apoptotic cells in vivo. J Exp Med 192:359–366
Ip WK, Lau YL (2004) Distinct maturation of, but not migration between, human monocyte-derived dendritic cells upon ingestion of apoptotic cells of early or late phases. J Immunol 173:189–196
Albert ML (2004) Death-defying immunity: do apoptotic cells influence antigen processing and presentation? Nat Rev 4:223–231
Franc NC (2002) Phagocytosis of apoptotic cells in mammals, Caenorhabditis elegans and Drosophila melanogaster: molecular mechanisms and physiological consequences. Front Biosci 7:d1298–d1313
Lauber K, Bohn E, Krober SM et al (2003) Apoptotic cells induce migration of phagocytes via caspase-3-mediated release of a lipid attraction signal. Cell 113:717–730
Mueller RB, Sheriff A, Gaipl US, Wesselborg S, Lauber K (2007) Attraction of phagocytes by apoptotic cells is mediated by lysophosphatidylcholine. Autoimmunity 40:342–344
Lauber K, Blumenthal SG, Waibel M, Wesselborg S (2004) Clearance of apoptotic cells: getting rid of the corpses. Mol Cell 14:277–287
Krysko DV, D’Herde K, Vandenabeele P (2006) Clearance of apoptotic and necrotic cells and its immunological consequences. Apoptosis 11:1709–1726
Erwig LP, Henson PM (2008) Clearance of apoptotic cells by phagocytes. Cell Death Differ 15:243–250
Ravichandran KS, Lorenz U (2007) Engulfment of apoptotic cells: signals for a good meal. Nat Rev 7:964–974
Aliprantis AO, Diez-Roux G, Mulder LC, Zychlinsky A, Lang RA (1996) Do macrophages kill through apoptosis? Immunol Today 17:573–576
Diez-Roux G, Lang RA (1997) Macrophages induce apoptosis in normal cells in vivo. Development (Cambridge, England) 124:3633–3638
Durrieu F, Belloc F, Lacoste L et al (1998) Caspase activation is an early event in anthracycline-induced apoptosis and allows detection of apoptotic cells before they are ingested by phagocytes. Exp Cell Res 240:165–175
McIlroy D, Tanaka M, Sakahira H et al (2000) An auxiliary mode of apoptotic DNA fragmentation provided by phagocytes. Genes Dev 14:549–558
Kurosaka K, Takahashi M, Watanabe N, Kobayashi Y (2003) Silent cleanup of very early apoptotic cells by macrophages. J Immunol 171:4672–4679
Haslett C (1999) Granulocyte apoptosis and its role in the resolution and control of lung inflammation. Am J Respir Crit Care Med 160:S5–S11
Brouckaert G, Kalai M, Krysko DV et al (2004) Phagocytosis of necrotic cells by macrophages is phosphatidylserine dependent and does not induce inflammatory cytokine production. Mol Biol Cell 15:1089–1100
Krysko DV, Denecker G, Festjens N et al (2006) Macrophages use different internalization mechanisms to clear apoptotic and necrotic cells. Cell Death Differ 13:2011–2022
Chung S, Gumienny TL, Hengartner MO, Driscoll M (2000) A common set of engulfment genes mediates removal of both apoptotic and necrotic cell corpses in C. elegans. Nat Cell Biol 2:931–937
Hirt UA, Gantner F, Leist M (2000) Phagocytosis of nonapoptotic cells dying by caspase-independent mechanisms. J Immunol 164:6520–6529
Meagher LC, Savill JS, Baker A, Fuller RW, Haslett C (1992) Phagocytosis of apoptotic neutrophils does not induce macrophage release of thromboxane B2. J Leukoc Biol 52:269–273
Voll RE, Herrmann M, Roth EA, Stach C, Kalden JR, Girkontaite I (1997) Immunosuppressive effects of apoptotic cells. Nature 390:350–351
Fadok VA, Bratton DL, Konowal A, Freed PW, Westcott JY, Henson PM (1998) Macrophages that have ingested apoptotic cells in vitro inhibit proinflammatory cytokine production through autocrine/paracrine mechanisms involving TGF-beta, PGE2, and PAF. J Clin Invest 101:890–898
Freire-de-Lima CG, Xiao YQ, Gardai SJ, Bratton DL, Schiemann WP, Henson PM (2006) Apoptotic cells, through transforming growth factor-beta, coordinately induce anti-inflammatory and suppress pro-inflammatory eicosanoid and NO synthesis in murine macrophages. J Biol Chem 281:38376–38384
Hirt UA, Leist M (2003) Rapid, noninflammatory and PS-dependent phagocytic clearance of necrotic cells. Cell Death Differ 10:1156–1164
Fadok VA, Bratton DL, Guthrie L, Henson PM (2001) Differential effects of apoptotic versus lysed cells on macrophage production of cytokines: role of proteases. J Immunol 166:6847–6854
Patel VA, Longacre A, Hsiao K et al (2006) Apoptotic cells, at all stages of the death process, trigger characteristic signaling events that are divergent from and dominant over those triggered by necrotic cells: Implications for the delayed clearance model of autoimmunity. J Biol Chem 281:4663–4670
Chautan M, Chazal G, Cecconi F, Gruss P, Golstein P (1999) Interdigital cell death can occur through a necrotic and caspase-independent pathway. Curr Biol 9:967–970
Polzer K, Schett G, Zwerina J (2007) The lonely death: chondrocyte apoptosis in TNF-induced arthritis. Autoimmunity 40:333–336
Redman SN, Khan IM, Tew SR, Archer CW (2007) In situ detection of cell death in articular cartilage. Methods Mol Med 135:183–200
Xu Y, Huang S, Liu ZG, Han J (2006) Poly(ADP-ribose) polymerase-1 signaling to mitochondria in necrotic cell death requires RIP1/TRAF2-mediated JNK1 activation. J Biol Chem 281:8788–8795
Festjens N, Vanden Berghe T, Cornelis S, Vandenabeele P (2007) RIP1, a kinase on the crossroads of a cell’s decision to live or die. Cell Death Differ 14:400–410
Artal-Sanz M, Samara C, Syntichaki P, Tavernarakis N (2006) Lysosomal biogenesis and function is critical for necrotic cell death in Caenorhabditis elegans. J Cell Biol 173:231–239
Brookes PS, Yoon Y, Robotham JL, Anders MW, Sheu SS (2004) Calcium, ATP, and ROS: a mitochondrial love-hate triangle. Am J Physiol Cell Physiol 287:C817–C833
Orrenius S, Zhivotovsky B, Nicotera P (2003) Regulation of cell death: the calcium-apoptosis link. Nat Rev Mol Cell Biol 4:552–565
Castro J, Bittner CX, Humeres A, Montecinos VP, Vera JC, Barros LF (2004) A cytosolic source of calcium unveiled by hydrogen peroxide with relevance for epithelial cell death. Cell Death Differ 11:468–478
Castro J, Ruminot I, Porras OH et al (2006) ATP steal between cation pumps: a mechanism linking Na+ influx to the onset of necrotic Ca2+ overload. Cell Death Differ 13:1675–1685
Syntichaki P, Tavernarakis N (2002) Death by necrosis. Uncontrollable catastrophe, or is there order behind the chaos? EMBO Rep 3:604–609
Nicotera P, Orrenius S (1998) The role of calcium in apoptosis. Cell Calcium 23:173–180
Yamashima T, Kohda Y, Tsuchiya K et al (1998) Inhibition of ischaemic hippocampal neuronal death in primates with cathepsin B inhibitor CA-074: a novel strategy for neuroprotection based on ‘calpain-cathepsin hypothesis’. Eur J Neurosci 10:1723–1733
Ono K, Kim SO, Han J (2003) Susceptibility of lysosomes to rupture is a determinant for plasma membrane disruption in tumor necrosis factor alpha-induced cell death. Mol Cell Biol 23:665–676
Zahrebelski G, Nieminen AL, al-Ghoul K, Qian T, Herman B, Lemasters JJ (1995) Progression of subcellular changes during chemical hypoxia to cultured rat hepatocytes: a laser scanning confocal microscopic study. Hepatology (Baltimore, MD) 21:1361–1372
Brunk UT, Dalen H, Roberg K, Hellquist HB (1997) Photo-oxidative disruption of lysosomal membranes causes apoptosis of cultured human fibroblasts. Free Radic Biol Med 23:616–626
Barros LF, Hermosilla T, Castro J (2001) Necrotic volume increase and the early physiology of necrosis. Comp Biochem Physiol 130:401–409
Buja LM, Eigenbrodt ML, Eigenbrodt EH (1993) Apoptosis and necrosis. Basic types and mechanisms of cell death. Arch Pathol Lab Med 117:1208–1214
Chen J, Liu X, Mandel LJ, Schnellmann RG (2001) Progressive disruption of the plasma membrane during renal proximal tubule cellular injury. Toxicol Appl Pharmacol 171:1–11
Nishimura Y, Lemasters JJ (2001) Glycine blocks opening of a death channel in cultured hepatic sinusoidal endothelial cells during chemical hypoxia. Cell Death Differ 8:850–858
Liu X, Schnellmann RG (2003) Calpain mediates progressive plasma membrane permeability and proteolysis of cytoskeleton-associated paxillin, talin, and vinculin during renal cell death. J Pharmacol Exp Ther 304:63–70
Bossy-Wetzel E, Newmeyer DD, Green DR (1998) Mitochondrial cytochrome c release in apoptosis occurs upstream of DEVD-specific caspase activation and independently of mitochondrial transmembrane depolarization. EMBO J 17:37–49
Gleiss B, Gogvadze V, Orrenius S, Fadeel B (2002) Fas-triggered phosphatidylserine exposure is modulated by intracellular ATP. FEBS Lett 519:153–158
Zamaraeva MV, Sabirov RZ, Maeno E, Ando-Akatsuka Y, Bessonova SV, Okada Y (2005) Cells die with increased cytosolic ATP during apoptosis: a bioluminescence study with intracellular luciferase. Cell Death Differ 12:1390–1397
Jaeschke H, Lemasters JJ (2003) Apoptosis versus oncotic necrosis in hepatic ischemia/reperfusion injury. Gastroenterology 125:1246–1257
Kim JS, He L, Lemasters JJ (2003) Mitochondrial permeability transition: a common pathway to necrosis and apoptosis. Biochem Biophys Res Commun 304:463–470
Honda H, Kondo T, Zhao QL, Feril LB Jr, Kitagawa H (2004) Role of intracellular calcium ions and reactive oxygen species in apoptosis induced by ultrasound. Ultrasound Med Biol 30:683–692
Assefa Z, Bultynck G, Szlufcik K et al (2004) Caspase-3-induced truncation of type 1 inositol trisphosphate receptor accelerates apoptotic cell death and induces inositol trisphosphate-independent calcium release during apoptosis. J Biol Chem 279:43227–43236
Schwab BL, Guerini D, Didszun C et al (2002) Cleavage of plasma membrane calcium pumps by caspases: a link between apoptosis and necrosis. Cell Death Differ 9:818–831
Paszty K, Verma AK, Padanyi R, Filoteo AG, Penniston JT, Enyedi A (2002) Plasma membrane Ca2+ATPase isoform 4b is cleaved and activated by caspase-3 during the early phase of apoptosis. J Biol Chem 277:6822–6829
Paszty K, Antalffy G, Penheiter AR et al (2005) The caspase-3 cleavage product of the plasma membrane Ca2+-ATPase 4b is activated and appropriately targeted. Biochem J 391:687–692
Paszty K, Antalffy G, Hegedus L et al (2007) Cleavage of the plasma membrane Ca+ATPase during apoptosis. Ann NY Acad Sci 1099:440–450
Tombal B, Denmeade SR, Gillis JM, Isaacs JT (2002) A supramicromolar elevation of intracellular free calcium ([Ca(2+)](i)) is consistently required to induce the execution phase of apoptosis. Cell Death Differ 9:561–573
Oshimi Y, Miyazaki S (1995) Fas antigen-mediated DNA fragmentation and apoptotic morphologic changes are regulated by elevated cytosolic Ca2+ level. J Immunol 154:599–609
Neumar RW, Xu YA, Gada H, Guttmann RP, Siman R (2003) Cross-talk between calpain and caspase proteolytic systems during neuronal apoptosis. J Biol Chem 278:14162–14167
Zhan Y, van de Water B, Wang Y, Stevens JL (1999) The roles of caspase-3 and bcl-2 in chemically-induced apoptosis but not necrosis of renal epithelial cells. Oncogene 18:6505–6512
Wattiaux R, Wattiaux-de Coninck S, Thirion J, Gasingirwa MC, Jadot M (2007) Lysosomes and Fas-mediated liver cell death. Biochem J 403:89–95
Vermes I, Haanen C, Reutelingsperger C (2000) Flow cytometry of apoptotic cell death. J Immunol Methods 243:167–190
Denecker G, Vercammen D, Steemans M et al (2001) Death receptor-induced apoptotic and necrotic cell death: differential role of caspases and mitochondria. Cell Death Differ 8:829–840
Wu X, Molinaro C, Johnson N, Casiano CA (2001) Secondary necrosis is a source of proteolytically modified forms of specific intracellular autoantigens: implications for systemic autoimmunity. Arthritis Rheum 44:2642–2652
Mahoney JA, Rosen A (2005) Apoptosis and autoimmunity. Curr Opin Immunol 17:583–588
Gaipl US, Munoz LE, Grossmayer G et al (2007) Clearance deficiency and systemic lupus erythematosus (SLE). J Autoimmun 28:114–121
Berg CP, Stein GM, Keppeler H et al (2008) Apoptosis-associated antigens recognized by autoantibodies in patients with the autoimmune liver disease primary biliary cirrhosis. Apoptosis 13:63–75
Eguchi Y, Shimizu S, Tsujimoto Y (1997) Intracellular ATP levels determine cell death fate by apoptosis or necrosis. Cancer Res 57:1835–1840
Leist M, Single B, Castoldi AF, Kuhnle S, Nicotera P (1997) Intracellular adenosine triphosphate (ATP) concentration: a switch in the decision between apoptosis and necrosis. J Exp Med 185:1481–1486
van der Toorn M, Slebos DJ, de Bruin HG et al (2007) Cigarette smoke-induced blockade of the mitochondrial respiratory chain switches lung epithelial cell apoptosis into necrosis. Am J Physiol 292:L1211–L1218
do Vale A, Costa-Ramos C, Silva DS et al (2007) Cytochemical and ultrastructural study of anoikis and secondary necrosis in enterocytes detached in vivo. Apoptosis 12:1069–1083
Vitale M, Zamai L, Mazzotti G, Cataldi A, Falcieri E (1993) Differential kinetics of propidium iodide uptake in apoptotic and necrotic thymocytes. Histochemistry 100:223–229
Belloc F, Dumain P, Boisseau MR et al (1994) A flow cytometric method using Hoechst 33342 and propidium iodide for simultaneous cell cycle analysis and apoptosis determination in unfixed cells. Cytometry 17:59–65
Sun F, Hamagawa E, Tsutsui C, Ono Y, Ogiri Y, Kojo S (2001) Evaluation of oxidative stress during apoptosis and necrosis caused by carbon tetrachloride in rat liver. Biochim Biophys Acta 1535:186–191
Hentze H, Schwoebel F, Lund S et al (2001) In vivo and in vitro evidence for extracellular caspase activity released from apoptotic cells. Biochem Biophys Res Commun 283:1111–1117
Holdenrieder S, Eichhorn P, Beuers U et al (2006) Nucleosomal DNA fragments in autoimmune diseases. Ann NY Acad Sci 1075:318–327
Walker NI, Bennett RE, Kerr JF (1989) Cell death by apoptosis during involution of the lactating breast in mice and rats. Am J Anat 185:19–32
Baxter FO, Neoh K, Tevendale MC (2007) The beginning of the end: death signaling in early involution. J Mammary Gland Biol Neoplasia 12:3–13
Erjefalt J (2005) Transepithelial migration, necrosis and apoptosis as silent and pro-inflammatory fates of airway granulocytes. Curr Drug Targets 4:425–431
Uller L, Persson CG, Erjefalt JS (2006) Resolution of airway disease: removal of inflammatory cells through apoptosis, egression or both? Trends Pharmacol Sci 27:461–466
Huettenbrenner S, Maier S, Leisser C et al (2003) The evolution of cell death programs as prerequisites of multicellularity. Mut Res 543:235–249
Golstein P, Kroemer G (2005) Redundant cell death mechanisms as relics and backups. Cell Death Differ 12(Suppl 2):1490–1496
Albert ML, Pearce SF, Francisco LM et al (1998) Immature dendritic cells phagocytose apoptotic cells via alphavbeta5 and CD36, and cross-present antigens to cytotoxic T lymphocytes. J Exp Med 188:1359–1368
Erwig LP, McPhilips KA, Wynes MW, Ivetic A, Ridley AJ, Henson PM (2006) Differential regulation of phagosome maturation in macrophages and dendritic cells mediated by Rho GTPases and ezrin-radixin-moesin (ERM) proteins. Proc Natl Acad Sci USA 103:12825–12830
Misawa R, Kawagishi C, Watanabe N, Kobayashi Y (2001) Infiltration of neutrophils following injection of apoptotic cells into the peritoneal cavity. Apoptosis 6:411–417
Liu CY, Liu YH, Lin SM et al (2003) Apoptotic neutrophils undergoing secondary necrosis induce human lung epithelial cell detachment. J Biomed Sci 10:746–756
Naylor EJ, Bakstad D, Biffen M et al (2007) Haemophilus influenzae induces neutrophil necrosis: a role in chronic obstructive pulmonary disease? Am J Respir Cell Mol Biol 37:135–143
Bell CW, Jiang W, Reich CF III, Pisetsky DS (2006) The extracellular release of HMGB1 during apoptotic cell death. Am J Physiol Cell Physiol 291:C1318–C1325
Jiang W, Bell CW, Pisetsky DS (2007) The relationship between apoptosis and high-mobility group protein 1 release from murine macrophages stimulated with lipopolysaccharide or polyinosinic-polycytidylic acid. J Immunol 178:6495–6503
Apetoh L, Ghiringhelli F, Tesniere A et al (2007) The interaction between HMGB1 and TLR4 dictates the outcome of anticancer chemotherapy and radiotherapy. Immunol Rev 220:47–59
Ito N, DeMarco RA, Mailliard RB et al (2007) Cytolytic cells induce HMGB1 release from melanoma cell lines. J Leukoc Biol 81:75–83
Ren Y, Stuart L, Lindberg FP et al (2001) Nonphlogistic clearance of late apoptotic neutrophils by macrophages: efficient phagocytosis independent of beta 2 integrins. J Immunol 166:4743–4750
Stern M, Savill J, Haslett C (1996) Human monocyte-derived macrophage phagocytosis of senescent eosinophils undergoing apoptosis. Mediation by alpha v beta 3/CD36/thrombospondin recognition mechanism and lack of phlogistic response. Am J Pathol 149:911–921
Rovere P, Sabbadini MG, Vallinoto C et al (1999) Delayed clearance of apoptotic lymphoma cells allows cross-presentation of intracellular antigens by mature dendritic cells. J Leukoc Biol 66:345–349
Gough MJ, Melcher AA, Ahmed A et al (2001) Macrophages orchestrate the immune response to tumor cell death. Cancer Res 61:7240–7247
Viorritto IC, Nikolov NP, Siegel RM (2007) Autoimmunity versus tolerance: can dying cells tip the balance? Clin Immunol (Orlando, FL) 122:125–134
Kim HS, Han MS, Chung KW et al (2007) Toll-like receptor 2 senses beta-cell death and contributes to the initiation of autoimmune diabetes. Immunity 27:321–333
Scott RS, McMahon EJ, Pop SM et al (2001) Phagocytosis and clearance of apoptotic cells is mediated by MER. Nature 411:207–211
Tuder RM, Petrache I, Elias JA, Voelkel NF, Henson PM (2003) Apoptosis and emphysema: the missing link. Am J Respir Cell Mol Biol 28:551–554
Maher JJ, Gores GJ (1998) Apoptosis: silent killer or neutron bomb? Hepatology (Baltimore, MD) 28:865–867
Farghali H, Canova N, Kucera T, Martinek J, Masek K (2003) Nitric oxide synthase inhibitors modulate lipopolysaccharide-induced hepatocyte injury: dissociation between in vivo and in vitro effects. Int Immunopharmacol 3:1627–1638
Ogasawara J, Watanabe-Fukunaga R, Adachi M et al (1993) Lethal effect of the anti-Fas antibody in mice. Nature 364:806–809
Gujral JS, Farhood A, Jaeschke H (2003) Oncotic necrosis and caspase-dependent apoptosis during galactosamine-induced liver injury in rats. Toxicol Appl Pharmacol 190:37–46
Unal-Cevik I, Kilinc M, Can A, Gursoy-Ozdemir Y, Dalkara T (2004) Apoptotic and necrotic death mechanisms are concomitantly activated in the same cell after cerebral ischemia. Stroke 35:2189–2194
Daemen MA, van’t Veer C, Denecker G et al (1999) Inhibition of apoptosis induced by ischemia-reperfusion prevents inflammation. J Clin Invest 104:541–549
James TN (1999) Apoptosis in cardiac disease. Am J Med 107:606–620
Scarabelli TM, Gottlieb RA (2004) Functional and clinical repercussions of myocyte apoptosis in the multifaceted damage by ischemia/reperfusion injury: old and new concepts after 10 years of contributions. Cell Death Differ 11(Suppl 2):S144–S152
Goldspink DF, Burniston JG, Tan LB (2003) Cardiomyocyte death and the ageing and failing heart. Exp Physiol 88:447–458
Leist M, Single B, Naumann H et al (1999) Inhibition of mitochondrial ATP generation by nitric oxide switches apoptosis to necrosis. Exp Cell Res 249:396–403
Nicotera P, Leist M, Fava E, Berliocchi L, Volbracht C (2000) Energy requirement for caspase activation, neuronal cell death. Brain Pathol (Zurich, Switzerland) 10:276–282
Nicotera P (2003) Molecular switches deciding the death of injured neurons. Toxicol Sci 74:4–9
Benchoua A, Guegan C, Couriaud C et al (2001) Specific caspase pathways are activated in the two stages of cerebral infarction. J Neurosci 21:7127–7134
Veinot JP, Gattinger DA, Fliss H (1997) Early apoptosis in human myocardial infarcts. Hum Pathol 28:485–492
Ankarcrona M, Dypbukt JM, Bonfoco E et al (1995) Glutamate-induced neuronal death: a succession of necrosis or apoptosis depending on mitochondrial function. Neuron 15:961–973
Denecker G, Vercammen D, Declercq W, Vandenabeele P (2001) Apoptotic and necrotic cell death induced by death domain receptors. Cell Mol Life Sci 58:356–370
Bredesen DE, Rao RV, Mehlen P (2006) Cell death in the nervous system. Nature 443:796–802
Lehrer RI, Ganz T, Selsted ME, Babior BM, Curnutte JT (1988) Neutrophils and host defense. Ann Intern Med 109:127–142
Lee WL, Downey GP (2001) Leukocyte elastase: physiological functions and role in acute lung injury. Am J Respir Crit Care Med 164:896–904
Henson PM, Johnston RB Jr (1987) Tissue injury in inflammation. Oxidants, proteinases, and cationic proteins. J Clin Invest 79:669–674
Weiss SJ (1989) Tissue destruction by neutrophils. N Engl J Med 320:365–376
Smith JA (1994) Neutrophils, host defense, and inflammation: a double-edged sword. J Leukoc Biol 56:672–686
Kawabata K, Hagio T, Matsuoka S (2002) The role of neutrophil elastase in acute lung injury. Eur J Pharmacol 451:1–10
Stockley RA (2006) Neutrophilic inflammation: “don’t you go to pieces on me! Eur Respir J 28:257–258
Faurschou M, Borregaard N (2003) Neutrophil granules and secretory vesicles in inflammation. Microbes Infect 5:1317–1327
Owen CA, Campbell EJ (1999) The cell biology of leukocyte-mediated proteolysis. J Leukoc Biol 65:137–150
Savill JS, Wyllie AH, Henson JE, Walport MJ, Henson PM, Haslett C (1989) Macrophage phagocytosis of aging neutrophils in inflammation. Programmed cell death in the neutrophil leads to its recognition by macrophages. J Clin Invest 83:865–875
Brazil TJ, Dagleish MP, McGorum BC, Dixon PM, Haslett C, Chilvers ER (2005) Kinetics of pulmonary neutrophil recruitment and clearance in a natural and spontaneously resolving model of airway inflammation. Clin Exp Allergy 35:854–865
Knapp S, Leemans JC, Florquin S et al (2003) Alveolar macrophages have a protective antiinflammatory role during murine pneumococcal pneumonia. Am J Respir Crit Care Med 167:171–179
Simon HU (2003) Neutrophil apoptosis pathways and their modifications in inflammation. Immunol Rev 193:101–110
Bianchi SM, Dockrell DH, Renshaw SA, Sabroe I, Whyte MK (2006) Granulocyte apoptosis in the pathogenesis and resolution of lung disease. Clin Sci (Lond) 110:293–304
Stockley RA (1999) Neutrophils and protease/antiprotease imbalance. Am J Respir Crit Care Med 160:S49–S52
Konstan MW, Berger M (1997) Current understanding of the inflammatory process in cystic fibrosis: onset and etiology. Pediatr Pulmonol 24:137–142; discussion 159–161
Fujie K, Shinguh Y, Inamura N, Yasumitsu R, Okamoto M, Okuhara M (1999) Release of neutrophil elastase and its role in tissue injury in acute inflammation: effect of the elastase inhibitor, FR134043. Eur J Pharmacol 374:117–125
Bank U, Ansorge S (2001) More than destructive: neutrophil-derived serine proteases in cytokine bioactivity control. J Leukoc Biol 69:197–206
Usher LR, Lawson RA, Geary I et al (2002) Induction of neutrophil apoptosis by the Pseudomonas aeruginosa exotoxin pyocyanin: a potential mechanism of persistent infection. J Immunol 168:1861–1868
Watt AP, Courtney J, Moore J, Ennis M, Elborn JS (2005) Neutrophil cell death, activation and bacterial infection in cystic fibrosis. Thorax 60:659–664
Jaeschke H, Smith CW (1997) Mechanisms of neutrophil-induced parenchymal cell injury. J Leukoc Biol 61:647–653
Jaeschke H (2006) Mechanisms of Liver Injury. II. Mechanisms of neutrophil-induced liver cell injury during hepatic ischemia-reperfusion and other acute inflammatory conditions. Am J Physiol Gastrointest Liver Physiol 290:G1083–G1088
Barone FC, Feuerstein GZ (1999) Inflammatory mediators and stroke: new opportunities for novel therapeutics. J Cereb Blood Flow Metab 19:819–834
Feuerstein G (2006) Inflammation and stroke: therapeutic effects of adenoviral expression of secretory Leukocyte Protease Inhibitor. Front Biosci 11:1750–1757
Bone RC, Balk RA, Cerra FB et al (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101:1644–1655
Vincent JL, Zambon M (2006) Why do patients who have acute lung injury/acute respiratory distress syndrome die from multiple organ dysfunction syndrome? Implications for management. Clin Chest Med 27:725–731; abstract x–xi
Wheeler AP, Bernard GR (2007) Acute lung injury and the acute respiratory distress syndrome: a clinical review. Lancet 369:1553–1564
Jochum M, Gippner-Steppert C, Machleidt W, Fritz H (1994) The role of phagocyte proteinases and proteinase inhibitors in multiple organ failure. Am J Respir Crit Care Med 150:S123–S130
Tumpey TM, Garcia-Sastre A, Taubenberger JK et al (2005) Pathogenicity of influenza viruses with genes from the 1918 pandemic virus: functional roles of alveolar macrophages and neutrophils in limiting virus replication and mortality in mice. J Virol 79:14933–14944
Shinya K, Hamm S, Hatta M, Ito H, Ito T, Kawaoka Y (2004) PB2 amino acid at position 627 affects replicative efficiency, but not cell tropism, of Hong Kong H5N1 influenza A viruses in mice. Virology 320:258–266
Rimmelzwaan GF, van Riel D, Baars M et al (2006) Influenza A virus (H5N1) infection in cats causes systemic disease with potential novel routes of virus spread within and between hosts. Am J Pathol 168:176–183; quiz 364
Stockley RA (2002) Neutrophils and the pathogenesis of COPD. Chest 121:151S–155S
Barnes PJ (2003) New concepts in chronic obstructive pulmonary disease. Annu Rev Med 54:113–129
Shapiro SD, Ingenito EP (2005) The pathogenesis of chronic obstructive pulmonary disease: advances in the past 100 years. Am J Respir Cell Mol Biol 32:367–372
Stockley RA (1994) The role of proteinases in the pathogenesis of chronic bronchitis. Am J Respir Crit Care Med 150:S109–S113
Ordonez CL, Shaughnessy TE, Matthay MA, Fahy JV (2000) Increased neutrophil numbers and IL-8 levels in airway secretions in acute severe asthma: Clinical and biologic significance. Am J Respir Crit Care Med 161:1185–1190
Palmqvist C, Wardlaw AJ, Bradding P (2007) Chemokines and their receptors as potential targets for the treatment of asthma. Brit J Pharmacol 151:725–736
Doring G (1994) The role of neutrophil elastase in chronic inflammation. Am J Respir Crit Care Med 150:S114–S117
Birrer P, McElvaney NG, Rudeberg A et al (1994) Protease-antiprotease imbalance in the lungs of children with cystic fibrosis. Am J Respir Crit Care Med 150:207–213
Taggart CC, Greene CM, Carroll TP, O’Neill SJ, McElvaney NG (2005) Elastolytic proteases: inflammation resolution and dysregulation in chronic infective lung disease. Am J Respir Crit Care Med 171:1070–1076
Hartl D, Latzin P, Hordijk P et al (2007) Cleavage of CXCR1 on neutrophils disables bacterial killing in cystic fibrosis lung disease. Nat Med 13:1423–1430
Hodge S, Hodge G, Scicchitano R, Reynolds PN, Holmes M (2003) Alveolar macrophages from subjects with chronic obstructive pulmonary disease are deficient in their ability to phagocytose apoptotic airway epithelial cells. Immunol Cell Biol 81:289–296
Hodge S, Hodge G, Ahern J et al (2007) Smoking alters alveolar macrophage recognition and phagocytic ability: implications in chronic obstructive pulmonary disease. Amer J Resp Cell Mol Biol 37:748–755
Vandivier RW, Henson PM, Douglas IS (2006) Burying the dead: the impact of failed apoptotic cell removal (efferocytosis) on chronic inflammatory lung disease. Chest 129:1673–1682
Bianchi SM, Prince LR, McPhillips K et al (2008) Impairment of apoptotic cell engulfment by pyocyanin, a toxic metabolite of Pseudomonas aeruginosa. Amer J Resp Crit Care Med 177:35–43
Medan D, Wang L, Yang X, Dokka S, Castranova V, Rojanasakul Y (2002) Induction of neutrophil apoptosis and secondary necrosis during endotoxin-induced pulmonary inflammation in mice. J Cell Physiol 191:320–326
Rydell-Tormanen K, Uller L, Erjefalt JS (2006) Direct evidence of secondary necrosis of neutrophils during intense lung inflammation. Eur Respir J 28:268–274
Kodama T, Yukioka H, Kato T, Kato N, Hato F, Kitagawa S (2007) Neutrophil elastase as a predicting factor for development of acute lung injury. Intern Med (Tokyo, Japan) 46:699–704
Fujishima S, Morisaki H, Ishizaka A et al (2007) Neutrophil elastase and systemic inflammatory response syndrome in the initiation and development of acute lung injury among critically ill patients. Biomed Pharmacother. Available online July 31 2007
Vandivier RW, Fadok VA, Hoffmann PR et al (2002) Elastase-mediated phosphatidylserine receptor cleavage impairs apoptotic cell clearance in cystic fibrosis and bronchiectasis. J Clin Invest 109:661–670
Zeiher BG, Matsuoka S, Kawabata K, Repine JE (2002) Neutrophil elastase and acute lung injury: prospects for sivelestat and other neutrophil elastase inhibitors as therapeutics. Crit Care Med 30:S281–S287
Sakashita A, Nishimura Y, Nishiuma T et al (2007) Neutrophil elastase inhibitor (sivelestat) attenuates subsequent ventilator-induced lung injury in mice. Eur J Pharmacol 571:62–71
Uchida Y, Kaibori M, Hijikawa T et al (2008) Protective effect of neutrophil elastase inhibitor (FR136706) in lethal acute liver failure induced by d-galactosamine and lipopolysaccharide in rats. J Surg Res 145:57–65
Uller L, Rydell-Tormanen K, Persson CG, Erjefalt JS (2005) Anti-Fas mAb-induced apoptosis and cytolysis of airway tissue eosinophils aggravates rather than resolves established inflammation. Respir Res 6:90
Walsh GM (2001) Eosinophil granule proteins and their role in disease. Curr Opin Hematol 8:28–33
Campbell EJ, Cury JD, Shapiro SD, Goldberg GI, Welgus HG (1991) Neutral proteinases of human mononuclear phagocytes. Cellular differentiation markedly alters cell phenotype for serine proteinases, metalloproteinases, and tissue inhibitor of metalloproteinases. J Immunol 146:1286–1293
Reis MI, do Vale A, Pinto C et al (2007) First molecular cloning and characterisation of caspase-9 gene in fish and its involvement in a gram negative septicaemia. Mol Immunol 44:1754–1764
Oliveira MS, Fraga AG, Torrado E et al (2005) Infection with Mycobacterium ulcerans induces persistent inflammatory responses in mice. Infect Immun 73:6299–6310
George KM, Chatterjee D, Gunawardana G et al (1999) Mycolactone: a polyketide toxin from Mycobacterium ulcerans required for virulence. Science 283:854–857
Sebbane F, Gardner D, Long D, Gowen BB, Hinnebusch BJ (2005) Kinetics of disease progression and host response in a rat model of bubonic plague. Am J Pathol 166:1427–1439
Marketon MM, DePaolo RW, DeBord KL, Jabri B, Schneewind O (2005) Plague bacteria target immune cells during infection. Science (New York, NY) 309:1739–1741
Narayanan SK, Nagaraja TG, Chengappa MM, Stewart GC (2002) Leukotoxins of gram-negative bacteria. Vet Microbiol 84:337–356
DeLeo FR (2004) Modulation of phagocyte apoptosis by bacterial pathogens. Apoptosis 9:399–413
Kaplan MJ (2004) Apoptosis in systemic lupus erythematosus. Clin Immunol (Orlando, FL) 112:210–218
Decker P (2006) Nucleosome autoantibodies. Clin Chim Acta 366:48–60
Mackay IR, Leskovsek NV, Rose NR (2008) Cell damage and autoimmunity: a critical appraisal. J Autoimmun 30:5–11
Devitt A, Parker KG, Ogden CA et al (2004) Persistence of apoptotic cells without autoimmune disease or inflammation in CD14−/− mice. J Cell Biol 167:1161–1170
Stuart LM, Takahashi K, Shi L, Savill J, Ezekowitz RA (2005) Mannose-binding lectin-deficient mice display defective apoptotic cell clearance but no autoimmune phenotype. J Immunol 174:3220–3226
Asano K, Miwa M, Miwa K et al (2004) Masking of phosphatidylserine inhibits apoptotic cell engulfment and induces autoantibody production in mice. J Exp Med 200:459–467
Herrmann M, Voll RE, Zoller OM, Hagenhofer M, Ponner BB, Kalden JR (1998) Impaired phagocytosis of apoptotic cell material by monocyte-derived macrophages from patients with systemic lupus erythematosus. Arthritis Rheum 41:1241–1250
Baumann I, Kolowos W, Voll RE et al (2002) Impaired uptake of apoptotic cells into tingible body macrophages in germinal centers of patients with systemic lupus erythematosus. Arthritis Rheum 46:191–201
Ren Y, Tang J, Mok MY, Chan AW, Wu A, Lau CS (2003) Increased apoptotic neutrophils and macrophages and impaired macrophage phagocytic clearance of apoptotic neutrophils in systemic lupus erythematosus. Arthritis Rheum 48:2888–2897
Hanayama R, Tanaka M, Miyasaka K et al (2004) Autoimmune disease and impaired uptake of apoptotic cells in MFG-E8-deficient mice. Science (New York, NY) 304:1147–1150
Gaipl US, Voll RE, Sheriff A, Franz S, Kalden JR, Herrmann M (2005) Impaired clearance of dying cells in systemic lupus erythematosus. Autoimmun Rev 4:189–194
Mitchell DA, Pickering MC, Warren J et al (2002) C1q deficiency and autoimmunity: the effects of genetic background on disease expression. J Immunol 168:2538–2543
Cohen PL, Caricchio R, Abraham V et al (2002) Delayed apoptotic cell clearance and lupus-like autoimmunity in mice lacking the c-mer membrane tyrosine kinase. J Exp Med 196:135–140
Nagata S (2007) Autoimmune diseases caused by defects in clearing dead cells and nuclei expelled from erythroid precursors. Immunol Rev 220:237–250
Munoz LE, Gaipl US, Franz S et al (2005) SLE—a disease of clearance deficiency? Rheumatology (Oxford, England) 44:1101–1107
Gaipl US, Kuhn A, Sheriff A et al (2006) Clearance of apoptotic cells in human SLE. Curr Dir Autoimmun 9:173–187
Gaipl US, Sheriff A, Franz S et al (2006) Inefficient clearance of dying cells and autoreactivity. Curr Top Microbiol Immunol 305:161–176
Oppenheim JJ, Yang D (2005) Alarmins: chemotactic activators of immune responses. Curr Opin Immunol 17:359–365
Yang H, Wang H, Czura CJ, Tracey KJ (2005) The cytokine activity of HMGB1. J Leukoc Biol 78:1–8
Scaffidi P, Misteli T, Bianchi ME (2002) Release of chromatin protein HMGB1 by necrotic cells triggers inflammation. Nature 418:191–195
Hall JC, Casciola-Rosen L, Rosen A (2004) Altered structure of autoantigens during apoptosis. Rheum Dis Clin North Am 30:455–471, vii
Marshak-Rothstein A (2006) Toll-like receptors in systemic autoimmune disease. Nature Rev 6:823–835
Krieg AM, Vollmer J (2007) Toll-like receptors 7, 8, and 9: linking innate immunity to autoimmunity. Immunol Rev 220:251–269
Acknowledgements
We are grateful to Drs. Andrew H. Wyllie, Richard A. Lockshin, Luisa Minghetti, Ágnes Enyedi, David S. Pisetsky, Yasunobu Okada and in particular L. Felipe Barros for helpful discussions, to Drs. Frank Madeo, Paula Ludovico and Manuela Côrte-Real for helpful discussions and for reviewing the text and to Anabela Costa for editorial assistance. This work was supported by FCT project POCI/MAR/56111/2004 funded by POCI 2010 and co-funded by FEDER, and grant SFRH/BPD/26816/2006.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Silva, M.T., do Vale, A. & dos Santos, N.M.N. Secondary necrosis in multicellular animals: an outcome of apoptosis with pathogenic implications. Apoptosis 13, 463–482 (2008). https://doi.org/10.1007/s10495-008-0187-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10495-008-0187-8