
Abstract
Various countries have permanent research bases in Antarctica that are manned year-round by a few members of an expedition team, facing extremes of temperature with the associated hardships. Acclimatisation to such an environment is associated with pyschophysiological changes along with alterations in sleep patterns. The present study was undertaken to explore the changes in sleep patterns of six members of the Indian expedition team during their winter stay at Maitri, the permanent research station of India in Antarctica. The mean (± SEM) age, height and weight of the subjects were 35.7 ± 2.32 years, 168.3 ± 2.37 cm and 71.0 ± 1.88 kg, respectively. Polysomnographic sleep recordings were obtained as baseline data in November 2004 in Delhi (altitude 260 m, latitude 29° N, longitude 77° E); data on the same parameters were collected at Maitri, Antarctica (altitude 120 m, latitude 70° 45′ 39″ S, longitude 11° 44′ 49″ E) from January to December 2005. A one-way analysis of variance with repeated measures showed a significant variation with time (month effect) in most of the sleep parameters recorded. Total sleep time decreased from Delhi baseline values in all months, sleep efficiency decreased significantly during winter months, duration of waking period after sleep onset increased significantly in winter, sleep latency increased immediately after exposure in January, stages 3 and 4 (slow wave sleep) reduced during dark winter months, whereas stages 1 and 2 and rapid eye movement sleep increased during dark winter months. This study observed a prevailing general trend of sleep disturbances amongst overwintering members in a modern Antarctic station.
Similar content being viewed by others

Introduction
The Antarctic environment comprises extreme cold, low humidity, almost continuous snowstorms, strong downdraughts and hurricane force winds, long polar days and nights, a high level of cosmic radiation, magnetic storms and increased ionisation. In addition to these environmental factors, the marked sensory deprivation, social isolation and sexual deprivation create a combination of psycho-social factors that influence human activities at polar stations. The fields of human biology and medicine can attempt to help people live and work more safely and effectively in such difficult conditions by researching the vulnerabilities of such a totally isolated human population.
Adaptation of overwintering members during prolonged stays in Antarctica is manifested by changes in various physiological variables (Broadway and Arendt 1988; Broadway et al. 1987; Kennaway and Van Dorp 1991; Sawhney et al. 1995, 1998; Malhotra et al. 1998; Yoneyama et al. 1999) along with changes in sleep patterns (Joern et al. 1970; Natani et al. 1970; Paterson 1975; Palinkas et al. 2000). Sleep studies carried out in previous Antarctic expeditions yielded two sets of observations. A first group of investigators (Taylor 1960; Gunderson 1963; Joern et al. 1970; Natani et al. 1970; Paterson 1975; Palinkas et al. 2000) observed that prolonged stay in Antarctica leads to changes in sleep patterns. Gunderson (1963) stated that sleep-related problems are a common complaint among sojourners in Antarctica. In early Antarctic expeditions, “polar insomnia” was a frequent complaint. The so-called “Big Eye” was qualified as epidemic by Taylor (1960), who linked it to the polar night and homesickness. It is classically accompanied by headaches and light depression, along with irritability and increased sensitivity to social and physical stimuli. Sleep studies in the Antarctic were first conducted using questionnaires (Shurley et al. 1970; Polosatov 1973). Insomnia was found to be rare, but sleep at night was light and frequently interrupted, with an increase in daytime sleepiness. These problems prevailed during winter and were attributed to the rigorous climate, polar night, and/or the emotional and psychological reactions elicited by isolation (Polosatov 1973).
Seasonal variations in sleep characteristics and their associations with changes in mood were examined in American men and women who spent the 1991 austral winter at three different research stations in Antarctica. It was observed that changes in mood during the austral winter are preceded by changes in sleep characteristics (Palinkas et al. 2000). Polysomnographic studies by Joern et al. (1970) reported loss of delta sleep (stages 3 and 4) as an immediate change towards acclimatisation to Antarctica in two subjects upon their arrival at the South Pole. A similar study was carried out by Natani et al. (1970) on four subjects (aged 23–32) at the South Pole station to monitor long-term changes in their sleep pattern. Recordings were carried out in three phases: before and after the Antarctic sojourn, and four times in the field with three recording sessions during winter. Each session lasted for three nights. The polysomnograms showed a decrease in delta sleep, diminution of paradoxical or rapid eye movement (REM) sleep and an increase in sleep latency in Antarctica. Paterson (1975) also reported a decrease in delta sleep in ten subjects wintering at the British Antarctic coastal station of Halley Bay.
In contrast, a second group of investigators (Bogolovskii 1974; Buguet et al. 1987) failed to observe any change in sleep patterns during prolonged stay in Antarctica. Bogolovskii (1974) stated that polar insomnia is no longer found in modern, comfortable Antarctic stations. Buguet et al. (1987) conducted polysomnographic sleep recordings on eight subjects who wintered at the French Antarctic coastal station of Dumont d’ Urville (140° 01′ E, 66° 40′ S) during the 21st French Polar Expedition in Adelie Land. The results of their study also failed to show any significant changes in all sleep variables. They concluded that improved physical fitness and cold-acclimatisation, which probably occurred, may have played a role.
Using questionnaire methods, Bhargava et al. (2000) reported that wintering members of the Indian Antarctic Expedition suffered from sleep disturbances and other behavioural adjustments during midwinter months. In view of the evidence from previous sleep studies carried out in the Antarctic, and subjective reports of sleep disturbances in the Indian station, the present study was undertaken with the aim of using polysomnographic techniques to objectively evaluate the sleep pattern of six wintering members of the 24th Indian Antarctic Expedition with respect to their prolonged stay in the harsh Antarctic environment.
Materials and methods
Subjects
The study was carried out on six healthy males (1 doctor, 2 meteorologists, 1 communications officer, 1 drilling engineer, 1 cook). The mean (± SEM) age, height and weight of the subjects were 35.7 ± 2.32 years, 168.3 ± 2.37 cm and 71.0 ± 1.88 kg, respectively. A sleep history of all subjects was recorded using standard questionnaire method. None of the subjects suffered from any sleep disorder problem on the mainland prior to their departure for Antarctica. They were briefed about the experimental procedures prior to the commencement of the study and their consent to extend maximum cooperation in the study was also obtained. None of the subjects had any night-shift obligations during their entire period of stay in Antarctica. The experimental procedures conformed to the principals outlined by the Declaration of Helsinki 1964.
Procedure
Baseline sleep measurements were carried out in Delhi (altitude 260 m, latitude 29° N, longitude 77° E) in November 2004 under controlled laboratory conditions [22–24°C, 50% relative humidity (RH)], with maximum and minimum ambient temperatures of 22° ± 1.2°C and 15° ± 2.0°C, respectively. On their journey to Antarctica, the expedition members were initially airlifted from Mumbai, India to Capetown, South Africa (38° S, 12° E), during the 2nd week of December 2004. They were then taken to India Bay (Antarctica) by ship, this voyage lasting 13 days. The subjects were then airlifted to the permanent Indian Antarctic station, Maitri. Maitri is located at the Schimarcher Oasis (altitude 120 m, latitude 70° 45′ 39″ S, longitude 11° 44′ 49″ E) on moraine soil, and is about 1,800 km from the South Pole. At this location, the sun is continuously seen above the horizon from November to February, or austral summer, and remains below the horizon from May to August, or austral winter. In Antarctica, the 12 months of the year fall into three seasons: initial summer (January–March), winter (April–September) and second summer (October–December). On arrival at the base, the expedition members were initially accommodated in unheated summer huts located around Maitri, in which the temperature ranged from 5 to 15°C, for about 7–10 days before they moved into the main station. The main station was centrally heated, with the temperature maintained between 22 and 25°C irrespective of the outside temperature. Thus, the room temperature during sleep recording remained the same as in control experiments in Delhi. In Delhi, subjects consumed a diet of 3,000–3,500 kcal day−1 (12.6–14.7 MJ; protein 14.6%, fat 24.9%, carbohydrate 60.5%), whereas in Antarctica the daily intake of dietary energy was 3,500–4,000 kcal day−1 (14.7–16.8 MJ; protein 11.9%, fat 26.3% and carbohydrate 61.8%). The mean weight of the subjects, which was 71.0 ± 1.88 kg in Delhi, increased during the initial summer months (January–March) in Antarctica to 78.6 ± 0.74 kg. However, during the winter months (April–September) this weight gain was reversed, reducing towards basal values and becoming almost normal at the end of the second summer months (October–November). Subjects were provided with a regular supply of warm running water and other amenities. The highest maximum and minimum ambient temperatures recorded around Maitri were 6°C in January and −37°C in July, respectively. Table 1 shows climatic data from Maitri from January to December 2005. In the summer months, the subjects in this study spent most of their time engaged in specialised jobs inside and outside the station. During routine as well as urgent outdoor work, they were protected with proper polar clothing and footgear. During winter months, as outdoor activities were limited (apart from essential activities to maintain the station), expedition members were involved mostly in leisure activities such as watching movies, reading books, playing computer games and cards to escape the monotony and boredom of the polar night. From April to September, when environmental conditions became extreme (e.g. severe temperature drops, high winds, blizzards) they remained confined to the station for periods of up to a few days at a stretch. However, subjects were allowed to move outside the station if they wished for short periods during this time. They did not practice yoga, meditation or any other physical exercise during the period of their stay.
Sleep recordings
Polysomnographic sleep recordings were carried out in Delhi and in Antarctica using a 40 channel polysomnograph (Bravo, Nicolet Biomedical, Madison, WI), using Ultrasom software for sleep staging. The sleep pattern in each subject was recorded for three consecutive nights at a time. The total recordings for the six subjects spanned about 18 days in each month. During baseline recordings in Delhi in November 2004, two dummy recordings were obtained for each subject during two consecutive nights to get them accustomed to the instrumentation and to sleeping under laboratory conditions. Actual recordings of baseline sleep profiles were made only in the third, fourth and fifth night (i.e. three consecutive nights). A similar protocol was followed during the first recording at Maitri, Antarctica, during the month of January 2005. Thereafter, sleep recordings were carried out for three consecutive nights for each subject. Total sleep recordings of 234 nights (six subjects × three nights each × 13 months) were carried out throughout the experiment. Electroencephalogram (EEG), electromyogram (EMG), electrocculogram (EOG), electrocardiogram (ECG), peripheral oxygen saturation (SpO2) and heart rate (HR) measurements during sleep were also recorded. EEG recordings were obtained from four regions, C3-A2, C4-A1, O1-A2 and O2-A1 using Ag-AgCl disc electrodes. Bipolar EOGs were recorded from the outer canthi of the left and right eyes (LOC and ROC), respectively. EMG recordings were obtained from the submandibular region. The ECG was recorded using standard limb leads. SpO2 and HR were recorded using a Capnograph (BCI Capnocheck Sleep, BCI International, Waukesha, WI). Sleep recording was started at 2100 hours and continued until the subjects woke up the next morning. After each subject was instrumented appropriately, data recording began and subjects were encouraged to sleep with the lights of the experimental room turned off. When the lights were turned on in the morning, the recording was terminated and the sleep recording system removed.
Electroencephalographic scoring
Sleep data were analysed using the Ultrasom software package (Nicolet Biomedical). Polysomnograms were visualised on a computer screen using the standard sleep montage (C3-A2, C4-A1, O1-A2 and O2-A1) for scoring sleep data. Two investigators used standard criteria (Rechtschaffen and Kales 1968) to score sleep stages manually, using blind polysomnography recordings taken every 30 s. Each recording was scored independently by both observers, and epochs in which the scorers disagreed were reviewed jointly. Sleep onset was defined as the first three consecutive epochs of sleep stage 1 or the first epoch of other stages of sleep. To study changes in sleep patterns, the data were processed under two categories, namely, general sleep characteristics and internal sleep architecture. The general sleep characteristics were time in bed (TIB; from lights out until the subject’s preferred time of arising), sleep period time (SPT; from falling asleep to morning awakening), wake after sleep onset (WASO), movement time (MT), total sleep time (TST; SPT − WASO + MT), sleep latency, sleep efficiency (% of TST vs TIB) and the mean sleep cycle time. The internal sleep architecture was examined by calculating the percentage of stages 1 and 2, stages 3 and 4 and REM sleep versus TST. Finally REM latency (which was considered to be the time elapsed from the first stage 2 to the first minute of REM) was also calculated.
Statistical analyses
Statistical analyses of sleep data were carried out using one-way ANOVA with repeated measures to compare values recorded during individual months spent in Antarctica and baseline values recorded in Delhi. Results are presented as the mean ± standard error of mean (SEM) of 18 nights’ recordings for each parameter in every month. Student’s Newman Keul post hoc test was carried out for comparing values obtained for different parameters in Antarctica in different months with baseline values observed in Delhi. The values in different months of stay in Antarctica were also inter-compared. A similar analysis was carried out to see whether there was a significant night effect on all sleep parameters. Differences were considered significant at P < 0.05. All statistical calculations were performed using SPSS software, version 15.
Results
Table 2 presents the monthly mean (± SEM) of sleep characteristics in Delhi and during the stay in Antarctica for all six subjects. Data obtained for a total of 234 nights were processed.
Significant variations between subjects (subject effect) were found for all sleep parameters recorded. Due to the subject effect, the sleep parameters of each subject were also examined separately.
The average time course of general sleep characteristics of individual subjects for each recording session (three nights) in each subject (DR, VK, KR, BP, AB and BI) in Delhi and also in Antarctica between January and December are shown in Figs. 1 and 2. There was no significant variation in TIB or SPT throughout the stay in Antarctica but the duration of TIB (481.0 ± 3.21 min) and SPT (478.5 ± 3.0 min) increased greatly compared to baseline values (456.3 ± 5.33 min and 453.9 ± 5.34 min, respectively) in the midwinter months. Statistical analysis revealed significant variation in TST (P < 0.001) with time (month effect). Results of the post hoc test between paired months showed that TST decreased significantly (P < 0.01) from baseline values (445.6 ± 5.47 min) in Delhi in all months during the stay in Antarctica. The decrease was not uniform in all months, with the maximum decrease (408.7 ± 7.96 min) being observed during the midwinter month of June. No significant difference in TST values were observed between different months of the subjects’ stay in Antarctica. In terms of individual subject variation, TST decreased in five out of six subjects. Subject DR showed an increase in TST from his basal value in almost all the months during the stay. Subjects AB and BP exhibited increased TST in January and November, respectively.

Time course of general sleep characteristics (expressed in minutes) averaged for each recording session in each subject (DR, VK, KR, BP, AB and BI) in Delhi and from January to December in Antarctica. Solid line, ■ Time in bed (TIB); broken line, ▲ sleep period time (SPT); solid line ● total sleep time (TST)

Time course of sleep latency (SL, solid line ■), movement time (MT, solid line ●) and wake after sleep onset (WASO, broken line ▲) averaged for each recording session in each subject (DR, VK, KR, BP, AB and BI) in Delhi and from January to December in Antarctica. Values are expressed in minutes
Sleep latency showed a significant variation with time (month effect) and was found to increase from that of baseline (2.4 ± 0.36 min) in Delhi only in the months of January (7.6 ± 1.16 min, P < 0.01) and April (3.9 ± 0.70 min, P < 0.01), being maintained almost at basal value for the rest of the period spent in the Antarctic. Comparison of sleep latency between different months showed that the changes in January were significant compared to all other months spent in Antarctica. Three subjects (VK, AB and BI) revealed a considerable increase in sleep latency in the initial summer month of January compared to basal values compared to other subjects. There was also a small increase in sleep latency in subjects BP and AB in April, accounting for the increase in the mean value for the group in this month.
Mean duration of WASO and MT increased significantly (P < 0.01 and 0.05) compared to baseline values in all six subjects in almost all the months during the stay in Antarctica except February and March. During the winter months of April, May, June and July, WASO and MT were found to be significantly higher (P < 0.01) than the values measured in the summer months of January, February, March, November and December. When individual subjects were considered, this change in WASO was found to be consistent in all six subjects (Fig. 2). The mean sleep efficiency of all six subjects started decreasing significantly (P < 0.01) immediately after their induction in Antarctica, with a maximum decrease of about 10% (87.3 ± 0.15%) compared to the basal value (97.7 ± 0.14%). This decreasing trend was maintained for the remaining months of the stay in Antarctica.
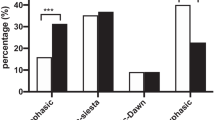
The time course of sleep stages throughout the period of stay of individual subjects is shown in Fig. 3. Significant variation in stages 1 and 2 (P < 0.001) with time (month effect) was observed. Stages 1 and 2 increased significantly (P < 0.01) from Delhi baseline values in all months during the stay at Antarctica, except for November when it decreased from the baseline value (Table 2). An average 9% increase from the basal value in stages 1 and 2 was observed mainly in midwinter. The duration of stages 1 and 2 in the winter months of April, May, June, July, August and September was significantly (P < 0.01) higher than in the initial summer months of January, February and March, as well as the second summer months of October, November and December. The increase in stages 1 and 2 was similar in all subjects as shown in Fig. 3. A return of stages 1 and 2 sleep towards basal values was evident in all subjects towards the end of the expedition.

Time course of stages 1 and 2 (Stg 1&2, solid line ■), stages 3 and 4 (Stg 3&4, broken line ▲) and rapid eye movement (REM, solid line ●) sleep averaged for each recording session in each subject (DR, VK, KR, BP, AB and BI) in Delhi and from January to December in Antarctica. Values are expressed as percentage of total sleep time
Stages 3 and 4 showed significant (P < 0.001) variation with time (month effect). Post hoc testing revealed that stages 3 and 4 decreased significantly (P < 0.01 and 0.05) from baseline values in Delhi in all months of the stay in Antarctica, except for November when it increased above the baseline value. This decreasing trend was most pronounced between April and September. There was an average 13% decrease in stages 3 and 4 from the basal value in midwinter. Similar to stages 1 and 2, the changes in stages 3 and 4 varied significantly between the winter and initial summer as well as the second summer months. The behaviour of the individual subjects followed almost the same trend as the group value.
REM sleep also exhibited a significant (P < 0.01) increase with time (month effect) during winter (April to September) only, and accounted for an increase during midwinter months of about 4% compared to baseline levels. Individual subjects responded almost in the same way as that of the group average, maintaining baseline values in the initial and second summers (Fig. 3). REM sleep increased in all the winter months and the changes from the January–March to the October–December values were significant. Individual subjects’ variation revealed that subject VK showed a small decrease in REM sleep in the month of April compared to the baseline value (Fig. 3). A significant increase in REM latency was found only in April.
There was no significant night effect when the first, second and third nights’ sleep recordings were compared.
Discussion
The results of the present study revealed a decrease in TST, an increase in sleep latency (mainly in the initial summer month), an increase in WASO, decreased sleep efficiency, a significant reduction in slow wave sleep (stages 3 and 4) and a significant increase in stage 1 and 2 and REM sleep during the dark winter months during a stay in an Antarctic research station.
The pattern of slow wave sleep in this study showed a seasonal variation, with a significant (P < 0.01) decrease in winter when compared to the summer months. The amount of slow wave sleep started decreasing immediately upon arrival in Antarctica, followed by a steep drop from the end of the summer months, which continued throughout the winter. However, levels recovered towards baseline values in the subsequent second summer months. The reduction in slow wave sleep during winter in all six subjects in our study is consistent with the findings of Palinkas et al. (2000), who also observed a complete absence of stage 4 sleep as well as sizable reduction in the amount of stage 3 sleep of overwintering members in Antarctica. Our findings also corroborate the work of Shurley (1974), who reported a similar reduction in stage 4 of slow wave sleep in four subjects overwintering in Antarctica. The results of the latter study showed that stage 4 was reduced immediately upon arrival in Antarctica, decreasing gradually thereafter to reach a maximum reduction of 0.6% of total sleep time towards the end of the dark winter period. Similar observations were reported in the Arctic by Buguet et al. (1976). Electroencephalographic sleep studies carried out by Buguet in the Arctic revealed a marked reduction in slow wave sleep during the winter months (Buguet et al. 1976). In contrast, studies conducted by Buguet et al. (1987) at the French coastal station of Dumont d’Urville contradict the findings of many other studies including the present study. In the study of Buguet et al. (1987), slow wave sleep showed a tendency to increase throughout the winter in all subjects studied, whereas stages 1 and 2 of sleep decreased. The authors concluded that the improved physical fitness of their subjects might have caused an increase in deep sleep, as these subjects exercised more during winter. The subjects in the present study were restricted mostly to indoor activities during the dark winter months, and experienced very little physical exertion. Since it is known that physical activity during daytime increases the duration of slow wave sleep activity (Buguet et al. 1980), lack of physical activity during the dark winter months might be one factor responsible for the reduced slow wave sleep found in our subjects. Alternatively, Sassin et al. (1969) observed that the absence of sunlight during winter might somehow depress hypothalamic function; this in turn would diminish the pituitary secretion of the human growth hormone, whose release is known to be associated with the onset of stage 4 sleep. Malhotra et al. (1998) observed a decrease in growth hormone from basal values in members of an overwintering Indian expedition during winter months, but the changes were not significant. Research on selective deprivation of deep sleep in healthy volunteers has revealed association with vague physical complaints, changes in bodily sensations, increased passivity, social withdrawal and mild depression (Agnew et al. 1964). Although a detail account of the symptoms of our subjects has not been assembled, symptoms similar to those just described were also observed in our subjects towards the end of winter.
Stages 1 and 2 followed a similar seasonal variation but with the opposite pattern of change compared to that of slow wave sleep in our subjects. A similar observation of increased stage 1 and 2 sleep was also reported by Paterson (1975) in ten subjects at the British Antarctic Survey base at Halley Bay. Significant increases in the amount of stage 1 and 2 sleep in their subjects matched the reduction in slow wave sleep. In our subjects, however, the increased stage 1 and 2 sleep throughout the period of stay in Antarctica did not match the decrease in slow wave sleep over the same period; this may be due to a concomitant increase in REM sleep, which accounts for about one-third of the sleep cycle.
The increase in REM sleep in our subjects during winter differed from findings in previous reports. For example, Buguet et al. (1987) failed to observe any change in REM sleep in eight subjects during their overwinter stay at the French coastal station. On the other hand, Shurley (1974) found a decrease in REM sleep from basal values in expedition members at the South Pole station. According to the hypotheses of Newman and Evans (1965) and Dewan (1968), the quantity of REM sleep varies directly with the information input load since the last period of sleep. Some reports have indicated that intensive cognitive activity or visual stimulation before sleep onset increases REM sleep (De Gennaro et al. 1995; Smith and Lapp 1991). In Antarctica, the information input load since the last period of sleep was related mostly to events within the station, as communication with the outside world was limited. It is worthwhile mentioning that, during winter, there was a manifold increase in the visual information loading of our subjects due to continuous watching of movies, playing computer games, reading books, etc. These activities kept the subjects and other expedition members busy and helped them to avoid the intensity of confinement, isolation and boredom. The contribution of this greater magnitude of sensory information loading of our subjects prior to sleep onset resulted in the occurrence of noticeably increased REM sleep during winter months. In addition, our subjects were also exposed to a much warmer environment (22–25°C) inside the station continuously during most of the winter months with minimum physical exertion compared to their exposure in the cold environment with frequent outdoor activities during the summer months. The amount of REM sleep during summer remained almost at the basal level. The effect of acute exposure to warm ambient temperature on sleep has been studied extensively on human volunteers in controlled laboratory conditions (Karacan et al. 1978; Muzet et al. 1983; Libert et al. 1988; Okamoto-Mizuno et al. 1999; Okamoto-Mizuno et al. 2004). These studies indicated that TST, stages 1 and 2, stages 3 and 4 and REM sleep decreased, with frequent and longer awakenings, greater shifting among sleep stages, and delayed onset of deep sleep (stages 3 and 4). However, animal experiments with chronic exposure of rats to warmer ambient temperature were found to produce a persistent increase in the amount of sleep, slow wave sleep and REM sleep (Rosenthal and Vogel 1993; Mahapatra et al. 2005). The observation in the present study of increased REM sleep in our subjects, who were exposed continuously to a warmer ambient temperature for a period of 6 months contradicts the previous observations on human volunteers mentioned above in which subjects experienced short-term exposure to warmer ambient temperature, but is in agreement with the observations of Rosenthal and Vogel (1993) and Mahapatra et al. (2005), who observed a greater amount of REM sleep in rats exposed for a longer duration to warmer ambient temperature. It may be emphasized that both factors, i.e. increased sensory information loading prior to sleep onset and prolonged confinement in the warmer environment of the Antarctic station, led to a greater amount of REM sleep in our subjects in winter months only.
Although there were no significant changes in TIB and SPT, TST and sleep efficiency were found to decrease in our subjects. There was a marked increase in sleep latency from the baseline value in the first month (January). However, in absolute terms, this resulted in an increase of only 5.2 min from the baseline value. WASO increased significantly from the baseline duration of 5.9 (± 0.39) min to a maximum of 40.6 (± 1.24) min in the winter month of May. This increase was maintained throughout the rest of the stay in all subjects. TST decreased significantly from the baseline in all the months of this study, with a maximum reduction of 37 min from baseline values during the midwinter month of June. One of the subjects (DR), however, showed a different response. This observation was contrary to the previous observation of Buguet et al. (1987), Shurley (1974) and Bogolovskii (1974), who reported no significant change in TST in their subjects. In our study, TST started recovering towards basal values during the second summer months when a new team arrives in the station. Sleep efficiency decreased significantly (P < 0.01) in parallel to TST, and maximally from 97.7% (± 0.14%) in Delhi to 87.3% (± 0.15%) in the dark midwinter month of June in Antarctica. The observed decreased TST and sleep efficiency with increased WASO strongly support the conclusion that the subjects had undergone sleep disturbance, mostly in the winter months, during their stay.
Owen and Arendt (1992) justified internal desynchronisation between sleep and circadian rhythm as one of the major causes of sleep disturbances in polar regions. Whether a similar internal desynchronisation between sleep and circadian rhythm occurred in our subjects remains a matter of speculation. Although there were individual subject variations in the sleep parameters studied, the individual trends of changes were almost the same in most of the subjects. One limitation of the present study is that we could not collect similar data from the same or a similar group of men in Delhi or elsewhere in India over the same period. Baseline data was collected in Delhi only in the month of November 2004 before leaving for Antarctica. Hence, the results of the present study cannot confirm that these sleep pattern changes are specific to Antarctica, as our subjects could not be studied for the same duration in Delhi.
In conclusion, this study contradicts the ideas of Bogolovskii (1974) and Buguet et al. (1987) that insomnia and major sleep disturbances are no longer a common feature of polar expedition members living in modern and comfortable Antarctic stations, but supports the observation of other researchers (Taylor 1960; Gunderson 1963; Joern et al. 1970; Natani et al. 1970; Paterson 1975; Palinkas et al. 2000) who found a general trend of sleep disturbances amongst overwintering expedition members in Antarctica. The hypodynamic Antarctic station microculture, with very little physical exertion during the cold and dark winter months, might provide one explanation for the reduced deep sleep observed in our subjects. The increased sensory information input load due to continuous watching of movies, playing computer games, reading books, etc., and the prolonged exposure to warmer ambient temperature within the station might be responsible for the increased REM sleep in our subjects, as observed during the same winter months. However, these sleep pattern changes might not be specific to Antarctica. The sedentary lifestyle adopted by expedition members during winter could be considered as the primary factor underlying sleep disturbances. The data provided in this study will give us an insight into the sleep-related problems encountered by volunteers temporarily residing in, and interacting with, the extreme environment of Antarctica. It will help us in designing novel intervention strategies such as yoga, meditation and appropriately designed physical exercise programmes, particularly during the dark winter months, to improve the quality and quantity of sleep during this period.
References
Agnew HW, Webb WB, Williams RL (1964) The effects of stage four sleep deprivation. Electroencephalogr Clin Neurophysiol 17:68–70. doi:10.1016/0013-4694(64)90011-2
Bhargava R, Mukerji S, Sachdeva U (2000) Psychological impact of the Antarctic winter on Indian expeditioners. Environ Behav 32:111–127. doi:10.1177/00139160021972450
Bogolovskii MM (1974) Polar insomnia on the Antarctic continent. Lancet 1(7856):503–504. doi:10.1016/S0140-6736(74)92803-7
Broadway JW, Arendt J (1988) Seasonal and bright light changes of the phase position of the human melatonin rhythm in Antarctica. Arctic Med Res 7:201–203
Broadway JW, Arendt J, Folkard S (1987) Bright light phase shifts the human melatonin rhythm during the Antarctic winter. Neurosci Lett 79:185–189. doi:10.1016/0304-3940(87)90694-X
Buguet A, Livingstone SD, Reed LD, Limmer RE (1976) EEG patterns and body temperatures in man during sleep in Arctic winter nights. Int J Biometeorol 20(1):61–69. doi:10.1007/BF01553173
Buguet A, Roussel B, Angus R, Sabiston B, Radomski M (1980) Human sleep and adrenal individual reactions to exercise. Electroencephalogr Clin Neurophysiol 49:515–523. doi:10.1016/0013-4694(80)90394-6
Buguet A, Rivolier J, Jouvet M (1987) Human sleep patterns in Antarctica. Sleep 10:374–382
De Gennaro L, Violani C, Ferrara M, Casagrande M, Bertini M (1995) Increase of REM duration and decrease of REM latency after a prolonged test of visual attention. Int J Neurosci 82:162–168
Dewan DM (1968) The P-hypothesis for dreaming sleep. Psychophysiology 5:203–208
Gunderson EKE (1963) Emotional symptoms in extremely isolated groups. Arch Gen Psychiatry 9:362–368
Joern AT, Shurley JT, Brooks RE, Guenter CA, Pierce CM (1970) Short term changes in sleep pattern on arrival at the south polar plateau. Arch Intern Med 125:649–654. doi:10.1001/archinte.125.4.649
Karacan I, Thornby JI, Anch AM, Williams RL, Perkins HM (1978) Effects of high ambient temperature on sleep in young men. Aviat Space Environ Med 49:855–860
Kennaway DJ, Van Dorp CF (1991) Free running rhythm of melatonin, cortisol, electrolytes, and sleep in humans in Antarctica. Am J Physiol Regul Integr Comp Physiol 29:R1137–R1144
Libert JP, Di Nisi J, Fukuda H, Muzet A, Ehrhart J, Amoros C (1988) Effect of continuous heat exposure on sleep stages in humans. Sleep 11:195–209
Mahapatra APK, Mallick HN, Kumar VM (2005) Changes in sleep on chronic exposure to warm and cold ambient temperatures. Physiol Behav 84:287–294. doi:10.1016/j.physbeh.2004.12.003
Malhotra AS, Pal K, Prasad R, Bajaj AC, Kumar R, Sawhney RC (1998) Plasma insulin and growth hormone during Antarctic residence. Jpn J Physiol 48:167–169. doi:10.2170/jjphysiol.48.167
Muzet A, Ehrhart J, Candas V, Libert JP, Vogt JJ (1983) REM sleep and ambient temperature in man. Int J Neurosci 18:117–126. doi:10.3109/00207458308985885
Natani K, Shurley JT, Pierce CM, Brooks RE (1970) Long term changes in sleep pattern in men on the south polar plateau. Arch Intern Med 125:655–659. doi:10.1001/archinte.125.4.655
Newman EA, Evans GR (1965) Human dream processes as analogous to computer program clearance. Nature 206:534–536. doi:10.1038/206534a0
Okamoto-Mizuno K, Mizuno K, Michie S, Maeda A, Iizuka S (1999) Effects of humid heat exposure on human sleep stages and body temperature. Sleep 22:767–773
Okamoto-Mizuno K, Tsuzuki K, Mizuno K (2004) Effects of mild heat exposure on sleep stages and body temperature in older men. Int J Biometeorol 9:32–36
Owen J, Arendt J (1992) Melatonin suppression in human subjects by bright and dim light in Antarctica: time and season dependent effects. Neurosci Lett 137:181–184. doi:10.1016/0304-3940(92)90399-R
Palinkas LA, Houseal M, Miller C (2000) Sleep and mood during winter in Antarctica. Int J Circumpolar Health 59:63–73
Paterson RAH (1975) Seasonal reduction of slow-wave sleep at an Antarctic coastal station. Lancet 1(7904):468–469. doi:10.1016/S0140-6736(75)91552-4
Polosatov MV (1973) Effects of the extreme factors of Antarctica on sleep of polar expedition members (English translation). Sov Ant Exped Infor Bull 86:69–74
Rechtschaffen A, Kales A (1968) A manual of standardised terminology, techniques and scoring system for sleep stages of human subjects. US Government Printing Office, Washinton DC
Rosenthal MS, Vogel GW (1993) The effect of a three day increase of ambient temperature toward the thermoneutral zone on rapid eye movement sleep in the rat. Sleep 16:702–705
Sassin JF, Parker DC, Mace JW, Gotlin RW, Johnson LC, Rossman LG (1969) Human growth hormone release—relation to slow-wave sleep and sleep-waking cycles. Science 165:513–515. doi:10.1126/science.165.3892.513
Sawhney RC, Malhotra AS, Nair CS, Bajaj AC, Rajan KC, Pal K et al (1995) Thyroid function during a prolonged stay in Antarctica. Eur J Appl Physiol 72:127–133. doi:10.1007/BF00964127
Sawhney RC, Malhotra AS, Prasad R, Pal K, Kumar R, Bajaj AC (1998) Pituitary gonadal hormones during prolonged residency in Antarctica. Int J Biometeorol 42:51–54. doi:10.1007/s004840050083
Shurley JT (1974) Physiological research at U.S. stations in Antarctica. In: Gunderson EKE (ed) Human adaptability to Antarctic conditions. American Geophysical Union, Washington, pp 71–87
Shurley JT, Pierce CM, Natani K, Brooks RE (1970) Sleep and activity patterns at South Pole station. A preliminary report. Arch Gen Psychiatry 22:385–389
Smith C, Lapp L (1991) Increases in number of REMs and REM density in humans following an intensive learning period. Sleep 14:325–330
Taylor IM (1960) Medical experiences at Mc Murdo Sound. In: Horvath S (ed) Cold injury. Macy, New York, pp 117–140
Yoneyama S, Hashimoto S, Honma K (1999) Seasonal changes of human circadian rhythm in Antarctica. Am J Physiol Regul Integr Comp Physiol 46:R1091–R1097
Acknowledgements
The authors would like to express their gratitude to all the volunteers for their participation in the study. We are thankful to the Defence Research and Development Organisation, Ministry of Defence, Government of India, Department of Science & Technology, Government of India for funding the project, and the National Centre for Antarctic and Ocean Research, Department of Ocean Development, Government of India for providing logistic support in Antarctica.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bhattacharyya, M., Pal, M.S., Sharma, Y.K. et al. Changes in sleep patterns during prolonged stays in Antarctica. Int J Biometeorol 52, 869–879 (2008). https://doi.org/10.1007/s00484-008-0183-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-008-0183-2