
Abstract
Background
To evaluate the antibacterial efficacy of photo-activated riboflavin using Ultraviolet A (UVA) on three bacterial strains commonly detected in keratitis.
Methods
Three bacterial strains (Staphylococcus epidermidis, Staphylococcus aureus and Pseudomonas aeruginosa) were cultured on blood/hematin–agar plates and dispersed in PBS. Dispersion was done of 10 μl of bacterial stock-solutions in 90 μl of RPMI, where different riboflavin molarities had been added, to achieve a bacterial concentration of 1-4 × 10 4/ml. Riboflavin end molarities before illumination were 0, 100, 200, 300 and 400 μM. Each solution had a negative control. The solutions were illuminated with UVA (365 nm) for 30 minutes (5.4 J/cm2) and then continued for a total time of 60 minutes (10.8 J/cm2). A count of CFU was conducted after incubation and results compared.
Results
In all tested strains, a slight decrease of bacteria was seen when exposed to UV for 30 minutes. A doubling of the UV dose showed a marked decrease of bacterial count in all bacteria tested. The combination of UV and riboflavin showed a more extensive reduction of CFU, confirming an interaction effect between UV and riboflavin.
Conclusion
Riboflavin photo-activation using UVA (365 nm) can achieve an extensive eradication of bacteria, and the combination is more potent in reducing bacterial number than UV alone.
Similar content being viewed by others


Introduction
Pathogen inactivation by way of riboflavin photosensitization, using ultraviolet or visible light, was first recognised in the 1960s [1]. Extensive investigation of this phenomenon indicates that microbes are damaged by non-specific oxidative stress, mediated by reactive oxygen species as well as by intercalation of the riboflavin molecule into the RNA and DNA of micro-organisms [2–4]. A wide range of micro-organisms including viruses, bacteria, and parasites have been effectively inactivated by the photosensitization of riboflavin using UV light. Mirasol™, a commercially available device for the purpose of pathogen inactivation in transfusions, is based on the UV/riboflavin combination [5–12]. Corneal cross-linking is also a procedure that is mediated by ultraviolet light photo-activation of riboflavin, and promising clinical results have been reported in the treatment of keratoconus, pellucid marginal degeneration and corneal ectasia [13–21]. It has been proposed that photosensitization of riboflavin, using ultraviolet light A (UVA) at 365 nm (Collagen Cross-linking), perhaps could be applied as a treatment against infectious keratitis. This is supported by published case reports [22–24] and in vitro experiments [25]. At a time when antibiotic-resistant micro-organisms are becoming an increasing problem [26–36], introduction of a new method to treat corneal infections would be of great benefit. It is crucial to elucidate whether the photo-activation of riboflavin using UVA at 365 nm is a method which is possible to incorporate in the treatment of microbial keratitis. There is to date no published data either on the efficiency of standard treatment protocol for keratoconus (Collagen Cross-linking) on bacterial growth inhibition, or whether the antibacterial effect is dependent on riboflavin concentration. We present a model to increase the understanding of the antibacterial efficacy of photo-activated riboflavin using UVA.
Materials and methods
Bacterial isolates were received from the microbiological department of Örebro University Hospital, and all bacterial strains were known reference bacteria. Isolates of Staphylococcus epidermidis RS 30 (s1) (ATCC 12228), Staphylococcus aureus RS 12 (s1) (CCUG 15915, ATCC 29213) and Pseudomonas aeruginosa RS 11 (s1) (CCUG 17619, ATCC 27853) were chosen for these experiments.
The bacteria were cultured on blood/hematin–agar plates, and the strains dispersed in PBS (GIBCO no: 14190, Invitrogen) to a concentration of approximately 108/ml. Counting of microbes was performed in a Burker chamber. Dilution of the above in PBS was made to reach concentrations of bacteria in stock solutions 2.0 × 105/ml (S. epidermidis), 3.5 × 105/ml (S. aureus) and 5.0 × 105/ml (P. aeruginosa). During the test period, the solutions were kept at room temperature (approximately 6 hours). Uncolored fluids were chosen in order to avoid disturbance or bias of pigment from broth in the photo-activation procedure. Dispersion was done of 10 μl of bacterial stock-solutions in 90 μl of riboflavin (No: R7649-25G, Sigma-Aldrich) in RPMI (GIBCO no: 11835, Invitrogen). This was done to achieve a bacterial concentration of 1-4 × 10 4/ml and riboflavin end molarities before illumination of 100, 200, 300 and 400 μM, in order to obtain a trend where eradication was most efficient. The addition of riboflavin was performed just before illumination with UV-light.
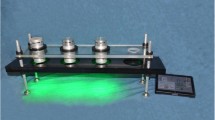
The total volume of fluid in the vessel was 100 μl, sufficient to maintain a thin layer of bacteria during 60 minutes incubation. The vessel chosen for the experiments were the inside of sterile corks from Sarstedt laboratory test tubes (No: 60.540.012, Sarstedt, Newton, NC, USA). These are white in color, and were selected to minimize light absorption during illumination. The inside diameter of the vessels was 8.5 mm and did not exceed the 9 mm spot, enabling illumination of the whole surface of solution.
For every preparation of riboflavin/bacteria solution, a non-illuminated control vessel was prepared. Each test series also had an illuminated control vessel with preparation of solution containing a similar bacterial end concentration without riboflavin. This solution without addition of riboflavin also had a negative control.
Prior to each illumination period, preparation for calculation of bacteria in solution and colony-forming units (CFU, 50 μl of diluted sample on each plate) determination was carried out.
The UV source used was UV-X (Peschke Meditrade™, Switzerland) with a wavelength of 365 nm. Calibration of the diode lamp was carried out before each experiment to determine that the value was between 2.7 and 3.3 mW/cm2. The distance of light source to surface of solution was 5 cm and illumination was conducted in a dark room, to prevent photosensitization of riboflavin from background visible light. After UV illumination for 30 minutes, resulting in a total dose of 5.4 J/cm2, 10 μl of the solution was extracted and determination of CFU/ml was performed. The remaining 90 μl of solution was illuminated directly after for another 30 minutes, resulting in a total UV dose of 10.8 J/cm2.
Subsequently all the solutions were diluted in PBS for count of CFU and incubated on agar plates for 18-20 hours at 37 centigrades. The number of CFU (mostly around 50-150 colonies/plate) was counted for each solution as well as the corresponding control solution, and the concentration of bacteria was calculated.
Each experiment was performed completely three times, thus resulting in three measurements at each point. A total of three numbers of CFU were estimated, since values received were either improbable or neglected and this was done to balance statistical analysis. During analysis these values were varied without any major changes in statistical results.
Statistical analysis was executed using a two-way ANOVA with factors UV and riboflavin and their interaction term was calculated. The results from bacterial count at 30 and 60 minutes were analyzed separately. Differences in bacterial number between start and end point (30 and 60 minutes respectively) were calculated at each measurement and used as outcome variable in the ANOVA. Comparison between solutions with and without riboflavin was carried out and statistical significance calculated. An unpaired t-test was done at each measured molarity comparing the differences between UV-exposed/unexposed solutions at end-point. Significance level was set to 5%. Software used for analysis was SPSS® 15.0 (SPSS Inc. Chicago, IL, USA).
Results
In the first experiment (Figs. 1 and 2) preparations were made with solutions of Staphylococcus epidermidis RS 30 (s1) (ATCC 12228) into start concentrations ranging between 1.6 and 2.5 × 104/ml. After 30 minutes non-illuminated solutions showed no clear tendency towards reduction in bacterial number. When exposed to UV, a slightly larger reduction was observed in all solutions. No significant differences were seen between vessels containing riboflavin and the simply UV-exposed vessels.

Staphylococcus epidermidis

Staphylococcus epidermidis
The decrease in bacterial count after 60 minutes of storage in RPMI was at all riboflavin concentrations similar to the one found after 30 minutes. UVA illumination without riboflavin was comparable to loss of bacteria from storage in RPMI (negative control), i.e. 27 and 23 percent respectively. The vessels containing riboflavin showed a clear reduction in bacterial count (mean reduction from start point ranging between 86 and 90%). No clear variation was seen at the diverse riboflavin levels. At all measured molarities, the differences between the riboflavin-absent solutions (simply UV-exposed) were statistically significant (p < 0.001). T-tests at each riboflavin level between UV-irradiated and negative controls were also statistically significant (p < 0.05). The p value for the interaction term of UV and riboflavin was 0.008.
In the next experiment, preparations with Staphyloccus aureus (Figs. 3 and 4) were dispersed to concentrations in final solutions varying between 2.5 and 4.0 × 104/ml. UV exposure for 30 minutes resulted in a decrease of bacteria in all vessels. Mean reduction varied between 11 and 39 percent. T-tests with negative controls revealed a statistical significance (p < 0.05), with the exception of the measurements at the 300 μM riboflavin level (p = 0.056). There was a tendency towards a higher reduction in the containers with riboflavin; however, this was in no case statistically significant. Again, no obvious pattern was observed regarding whether the extent of riboflavin in dispensers had significance in the eradication of micro-organisms.

Staphylococcus aureus

Staphylococcus aureus
As illumination time was doubled, the number of bacteria in solutions containing riboflavin was further reduced, with a tendency towards a slightly higher reduction as molarity of riboflavin increased. The mean eradication of bacteria in the containers without riboflavin compared to the number at the starting point equalled 28%, whereas the decrease in presence of riboflavin ranged between 61 and 71 percent. The reduction compared to negative controls was at all riboflavin levels statistically significant (p < 0.05). When comparisons were made with riboflavin-absent solutions, illuminated with UV, statistical significance was seen at 300 and 400 μM (p values 0.018 and 0.021 respectively) and the p value for the interaction term between UV and riboflavin was 0.038.
For the final experiment (Figs. 5 and 6), solutions were prepared with start concentrations of Pseudomonas aeruginosa between 9.4 × 103/ml and 3.1 × 104/ml. At evaluation after both 30 and 60 minutes, UV exposure alone showed no further reduction than control solutions. The mean CFU count even somewhat exceeded the one found in negative controls, yet the differences were not statistically significant at either of these points. When subjected to UV for 30 minutes, in presence of riboflavin, a decrease of bacteria was seen at all molarities, ranging between 39 and 53 percent; however, t-tests showed a statistical significance only at the 300 μM level (p < 0.05).

Pseudomonas aeruginosa

Pseudomonas aeruginosa
All the solutions containing riboflavin showed after 60 minutes illumination a nearly complete eradication of micro-organisms, averaging between 98 and 100 percent. Storage of bacteria in presence of riboflavin presented a slightly variable pattern, but no additional reduction in bacterial number was observed when compared to the 30-minutes reading. The differences compared to non-illuminated controls were statistically significant at the 100 and 400 μM readings (p < 0.05) and bordering statistical significance at the 200 and 300 levels (p = 0.051 and p = 0.054 respectively). The ANOVA showed statistical significance at all levels containing riboflavin when comparied to the riboflavin-absent solutions (p < 0.05). The interaction term was also statistically significant (p = 0.034).
Discussion
The results of our in vitro experiments clearly show that photo-activation of riboflavin using UVA at 365 nm achieves eradication of all three tested bacteria. An augmentation of UV exposure time increased this effect in all tested strains. It is also evident that the combination of riboflavin and UV was considerably more efficient in reducing micro-organisms than UV single-handedly. A dose of 10.8 J/cm2 (or UV exposure for 60 minutes) resulted in a high degree of eradication of each bacterium. Doubling the length of UV irradiation led to a response of greater magnitude than variations in riboflavin molarity. This might be explained by the fact that an increase in the UV dose should also amplify the amount of oxidative stress generated; however, an augmentation in riboflavin concentration does not necessarily do the same. Perhaps only a small amount of riboflavin is required to achieve the effect studied, and excess riboflavin may even block UV penetration into deeper layers of the fluid solution.
Interestingly, the bacteria tested showed a rather heterogeneous response to the procedure, indicating a variation in sensibility between different micro-organisms. Perhaps diversities in metabolism and sensitivity to oxidative stress could explain the differences in sensitivity between the tested bacteria. Several factors could be of importance for these differences. The length of cell cycle could be of significance, since a shorter cell cycle would increase the possibility for exposure during cell division, leading to a higher risk of errors in genetic material of micro-organisms, followed by mutations and cell death. Cell wall structure, intracellular transport systems and metabolic pathways are other factors that may well influence sensitivity to oxidative stress.
These results support the observations of Martins et al. [25] that the photo-sensitization of riboflavin seems to have an efficient antimicrobial effect, especially if the dose of UV is increased.
It is therefore a future possibility that this procedure could be developed into a treatment option in handling infectious keratitis. This could conceivably be an alternative, but more likely a complement to the topical antibiotic therapy. A new mechanism of action against pathogens would be of great benefit and maybe a considerable improvement in the treatment of microbial keratitis. Antibiotic-resistant bacterial strains could also be of less significance when using photo-activation procedures.
Incubation time for 30 minutes resulted in only a limited bacterial eradication in this model, signifying that the settings used in treatment of keratoconus might not be sufficient for complete sterilization of an infectious ulcer during a keratitis. The layer of fluid in our model may also in part explain a retardation of the UV penetration in the solution, resulting in a reduced effect of the treatment. A decrease of the fluid layer thickness would increase the UV penetration in the whole fluid layer, possibly increasing the eradicating effect. Interfacial tension and fluid evaporation are two factors making it very difficult to use a small enough volume of bacterial solution in order to enable UV penetration in the whole fluid thickness.
The model described presents an opportunity to study the effect of the UV–riboflavin combination in multiple micro-organisms, as well as determining the importance of riboflavin concentration for each tested strain. The outcome observed in these experiments at different levels of riboflavin did not show clear differences in efficacy. However, it is important to realize that the different molarities translate only to minute variations in riboflavin concentration. It would naturally be of interest to investigate exactly at which riboflavin level the peak eradication is located; however, this is beyond the scope of this particular work.
The antimicrobial effect of riboflavin photosensitization using UVA should be further explored, as it might have the potential to be incorporated into the therapy of infectious conditions, such as keratitis.
References
Tsugita A, Okada Y, Uehara K (1965) Photosensitized inactivation of ribonucleic acids in the presence of riboflavin. Biochim Biophys Acta 103:360–363
Kumar V, Lockerbie O, Keil SD, Ruane PH, Platz MS, Martin CB, Ravanat JL, Cadet J, Goodrich RP (2004) Riboflavin and UV-light based pathogen reduction: extent and consequence of DNA damage at the molecular level. Photochem Photobiol 80:15–21
Corbin F 3rd (2002) Pathogen inactivation of blood components: current status and introduction of an approach using riboflavin as a photosensitizer. Int J Hematol 76(Suppl 2):253–257, Review
AuBuchon JP, Herschel L, Roger J, Taylor H, Whitley P, Li J, Edrich R, Goodrich RP (2005) Efficacy of apheresis platelets treated with riboflavin and ultraviolet light for pathogen reduction. Transfusion 45:1335–1341
Ruane PH, Edrich R, Gampp D, Keil SD, Leonard RL, Goodrich RP (2004) Photochemical inactivation of selected viruses and bacteria in platelet concentrates using riboflavin and light. Transfusion 44:877–885
Cardo LJ, Rentas FJ, Ketchum L, Salata J, Harman R, Melvin W, Weina PJ, Mendez J, Reddy H, Goodrich R (2006) Pathogen inactivation of Leishmania donovani infantum in plasma and platelet concentrates using riboflavin and ultraviolet light. Vox Sang 90:85–91
Cardo LJ, Salata J, Mendez J, Reddy H, Goodrich R (2007) Pathogen inactivation of Trypanosoma cruzi in plasma and platelet concentrates using riboflavin and ultraviolet light. Transfus Apher Sci 37:131–137
Goodrich RP, Edrich RA, Li J, Seghatchian J (2006) The Mirasol PRT system for pathogen reduction of platelets and plasma: an overview of current status and future trends. Transfus Apher Sci 35:5–17, Review
AuBuchon JP, Herschel L, Roger J, Taylor H, Whitley P, Li J, Edrich R, Goodrich RP (2005) Efficacy of apheresis platelets treated with riboflavin and ultraviolet light for pathogen reduction. Transfusion 45:1335–1341
Picker SM, Steisel A, Gathof BS (2008) Effects of Mirasol PRT treatment on storage lesion development in plasma-stored apheresis-derived platelets compared to untreated and irradiated units. Transfusion 48:1685–1692
Reddy HL, Dayan AD, Cavagnaro J, Gad S, Li J, Goodrich RP (2008) Toxicity testing of a novel riboflavin-based technology for pathogen reduction and white blood cell inactivation. Transfus Med Rev 22:133–153, Review
Perez-Pujol S, Tonda R, Lozano M, Fuste B, Lopez-Vilchez I, Galan AM, Li J, Goodrich R, Escolar G (2005) Effects of a new pathogen-reduction technology (Mirasol PRT) on functional aspects of platelet concentrates. Transfusion 45:911–919
Wollensak G (2006) Crosslinking treatment of progressive keratoconus: new hope. Curr Opin Ophthalmol 17:356–360, Review
Wollensak G, Spoerl E, Seiler T (2003) Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol 135:620–627
Kanellopoulos AJ, Binder PS (2007) Collagen cross-linking (CCL) with sequential topography-guided PRK: a temporizing alternative for keratoconus to penetrating keratoplasty. Cornea 26:891–895
Hafezi F, Kanellopoulos J, Wiltfang R, Seiler T (2007) Corneal collagen crosslinking with riboflavin and ultraviolet A to treat induced keratectasia after laser in situ keratomileusis. J Cataract Refract Surg 33:2035–2040
Caporossi A, Baiocchi S, Mazzotta C, Traversi C, Caporossi T (2006) Parasurgical therapy for keratoconus by riboflavin-ultraviolet type A rays induced cross-linking of corneal collagen: preliminary refractive results in an Italian study. J Cataract Refract Surg 32:837–845
Raiskup-Wolf F, Hoyer A, Spoerl E, Pillunat LE (2008) Collagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term results. J Cataract Refract Surg 34:796–801
Coskunseven E, Jankov MR 2nd, Hafezi F (2009) Contralateral eye study of corneal collagen cross-linking with riboflavin and UVA irradiation in patients with keratoconus. J Refract Surg 25:371–376
Wittig-Silva C, Whiting M, Lamoureux E, Lindsay RG, Sullivan LJ, Snibson GR (2008) A randomized controlled trial of corneal collagen cross-linking in progressive keratoconus: preliminary results. J Refract Surg 24:S720–S725
Vinciguerra P, Albè E, Trazza S, Rosetta P, Vinciguerra R, Seiler T, Epstein D (2009) Refractive, topographic, tomographic, and aberrometric analysis of keratoconic eyes undergoing corneal cross-linking. Ophthalmology 116:369–378
Schnitzler E, Spörl E, Seiler T (2000) Irradiation of cornea with ultraviolet light and riboflavin administration as a new treatment for erosive corneal processes, preliminary results in four patients. Klin Monatsbl Augenheilkd 217:190–193
Iseli HP, Thiel MA, Hafezi F, Kampmeier J, Seiler T (2008) Ultraviolet A/riboflavin corneal cross-linking for infectious keratitis associated with corneal melts. Cornea 27:590–594
Micelli Ferrari T, Leozappa M, Lorusso M, Epifani E, Micelli Ferrari L (2009) Escherichia coli keratitis treated with ultraviolet A/riboflavin corneal cross-linking: a case report. Eur J Ophthalmol 19:295–297
Martins SA, Combs JC, Noguera G, Camacho W, Wittmann P, Walther R, Cano M, Dick J, Behrens A (2008) Antimicrobial efficacy of riboflavin/UVA combination (365 nm) in vitro for bacterial and fungal isolates: a potential new treatment for infectious keratitis. Invest Ophthalmol Vis Sci 49:3402–3408
Moshirfar M, Meyer JJ, Espandar L (2007) Fourth-generation fluoroquinolone-resistant mycobacterial keratitis after laser in situ keratomileusis. J Cataract Refract Surg 33:1978–1981
Mamalis N (2007) The increasing problem of antibiotic resistance. J Cataract Refract Surg 33:1831–1832
de la Cruz J, Behlau I, Pineda R (2007) Atypical mycobacteria keratitis after laser in situ keratomileusis unresponsive to fourth-generation fluoroquinolone therapy. J Cataract Refract Surg 33:1318–1321
Moshirfar M, Mirzaian G, Feiz V, Kang PC (2006) Fourth-generation fluoroquinolone-resistant bacterial keratitis after refractive surgery. J Cataract Refract Surg 32:515–518
Jhanji V, Sharma N, Satpathy G, Titiyal J (2007) Fourth-generation fluoroquinolone-resistant bacterial keratitis. J Cataract Refract Surg 33:1488–1489
McGhee CN, Niederer R (2006) Resisting susceptibility: bacterial keratitis and generations of antibiotics. Clin Experiment Ophthalmol 34:3–5
Betanzos-Cabrera G, Juárez-Verdayes MA, González-González G, Cancino-Díaz ME, Cancino-Díaz JC (2009) Gatifloxacin, moxifloxacin, and balofloxacin resistance due to mutations in the gyrA and parC genes of Staphylococcus epidermidis strains isolated from patients with endophthalmitis, corneal ulcers and conjunctivitis. Ophthalmic Res 42:43–48
O'Neill AJ (2008) New antibacterial agents for treating infections caused by multi-drug resistant Gram-negative bacteria. Expert Opin Investig Drugs 17:297–302, Review
Talbot GH (2008) What is in the pipeline for Gram-negative pathogens? Expert Rev Anti Infect Ther 6:39–49, Review
Nicasio AM, Kuti JL, Nicolau DP (2008) The current state of multidrug-resistant gram-negative bacilli in North America. Pharmacotherapy 28:235–249, Review
McGowan JE Jr (2006) Resistance in nonfermenting gram-negative bacteria: multidrug resistance to the maximum. Am J Med 119(Suppl 1):S29–S36, discussion S62-70. Review
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Makdoumi, K., Bäckman, A., Mortensen, J. et al. Evaluation of antibacterial efficacy of photo-activated riboflavin using ultraviolet light (UVA). Graefes Arch Clin Exp Ophthalmol 248, 207–212 (2010). https://doi.org/10.1007/s00417-009-1231-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-009-1231-2