
Abstract
Background
With the advent of sestamibi scans, high-resolution ultrasonography (US), and intraoperative intact parathyroid hormone (PTH) measurements, minimally invasive parathyroidectomy (MIP) is considered the standard of care for patients with primary hyperparathyroidism (PHPT). Preoperative imaging, however, can be negative more than 20% of the time.
Methods
We chose to examine one surgeon’s experience with patients who presented with PHPT and negative or indeterminate preoperative imaging from July 1993 to September 2009. A retrospective review of a parathyroid surgery database and patient records was conducted to collect the following information: patient age and sex; calcium and PTH levels; sestamibi and US results; and operative reports. Each sestamibi scan had been re-reviewed preoperatively by the surgeon with a nuclear medicine physician. The study cohort included patients with negative or indeterminate sestamibi results and a negative or no US report in which the surgeon was able to identify a “shadow” or subtlety on sestamibi and plan an MIP.
Results
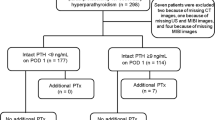
A total of 126 patients had a negative or indeterminate sestamibi scan and a negative or no US report. “Shadows” or subtleties were found in 18 of 44 (41%) of the cases with a negative sestamibi and in 62 of 82 (76%) of cases with an indeterminate sestamibi scan. For these 80 cases a MIP was planned. In all, 7 of 80 (9%) were converted to a bilateral exploration. The remaining 46 patients underwent a planned bilateral exploration. Cure rates were comparable: 99% in the study group compared to 97% in the group who underwent a planned or converted bilateral exploration.
Conclusions
With careful preoperative re-review of a negative or indeterminate sestamibi scan and the identification of subtleties in patients with a negative preoperative US scan, a successful MIP can be performed 91% of the time with a 98% cure rate.





Similar content being viewed by others

References
Greene AB, Butler RS, McIntyre S et al (2009) National trends in parathyroid surgery from 1998 to 2008: a decade of change. J Am Coll Surg 209:332–343
Civelek AC, Ozalp E, Donovan P et al (2002) Prospective evaluation of delayed technetium-99m sestamibi SPECT scintigraphy for preoperative localization of primary hyperparathyroidism. Surgery 131:149–157
Mihai R, Gleeson F, Buley ID et al (2006) Negative imaging studies for primary hyperparathyroidism are unavoidable: correlation of sestamibi and high-resolution ultrasound scanning with histological analysis in 150 patients. World J Surg 30:697–704
Melton GB, Somervell H, Friedman KP et al (2005) Interpretation of 99mTc sestamibi parathyroid SPECT scan is improved when read by the surgeon and nuclear medicine physician together. Nucl Med Commun 26:633–638
Bilezikian JP, Potts JT Jr, Fuleihan Gel H et al (2002) Summary statement from a workshop on asymptomatic primary hyperparathyroidism: a perspective for the 21st century. J Clin Endocrinol Metab 87:5353–5361
Arkles LB, Jones T, Hicks RJ et al (1996) Impact of complementary parathyroid scintigraphy and ultrasonography on the surgical management of hyperparathyroidism. Surgery 120:845–851
Purcell GP, Dirbas FM, Jeffrey RB et al (1999) Parathyroid localization with high-resolution ultrasound and technetium Tc 99m sestamibi. Arch Surg 134:824–828 (discussion 828–830)
Arici C, Cheah WK, Ituarte PH et al (2001) Can localization studies be used to direct focused parathyroid operations? Surgery 129:720–729
Nguyen BD (1999) Parathyroid imaging with Tc-99m sestamibi planar and SPECT scintigraphy. Radiographics 19:601–614 (discussion 615–616)
Solorzano CC, Lee TM, Ramirez MC et al (2005) Surgeon-performed ultrasound improves localization of abnormal parathyroid glands. Am Surg 71:557–562 (discussion 562–563)
Moalem J, Guerrero M, Kebebew E (2009) Bilateral neck exploration in primary hyperparathyroidism: when is it selected and how is it performed? World J Surg 33:2282–2291
Bilezikian JP, Khan AA, Potts JT Jr (2009) Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the third international workshop. J Clin Endocrinol Metab 94:335–339
Ogilvie JB, Clark OH (2005) Parathyroid surgery: we still need traditional and selective approaches. J Endocrinol Invest 28:566–569
Yip L, Pryma DA, Yim JH et al (2009) Sestamibi SPECT intensity scoring system in sporadic primary hyperparathyroidism. World J Surg 33:426–433
Anonymous (1990) Diagnosis and management of asymptomatic primary hyperparathyroidism. National Institutes of Health Consensus Development Conference, October 29–31, 1990. Consensus Statement 8:1–18
Irvin GL 3rd, Dembrow VD, Prudhomme DL (1993) Clinical usefulness of an intraoperative “quick parathyroid hormone” assay. Surgery 114:1019–1022 (discussion 1022–1023)
Westerdahl J, Bergenfelz A (2007) Unilateral versus bilateral neck exploration for primary hyperparathyroidism: five-year follow-up of a randomized controlled trial. Ann Surg 246:976–980 (discussion 980–981)
Slepavicius A, Beisa V, Janusonis V et al (2008) Focused versus conventional parathyroidectomy for primary hyperparathyroidism: a prospective, randomized, blinded trial. Langenbecks Arch Surg 393:659–666
Miccoli P, Bendinelli C, Berti P et al (1999) Video-assisted versus conventional parathyroidectomy in primary hyperparathyroidism: a prospective randomized study. Surgery 126:1117–1121 (discussion 1121–1122)
Carty SE, Worsey J, Virji MA et al (1997) Concise parathyroidectomy: the impact of preoperative SPECT 99mTc sestamibi scanning and intraoperative quick parathormone assay. Surgery 122:1107–1114 (discussion 1114–1116)
Udelsman R (2002) Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg 235:665–670 (discussion 670–672)
Lavely WC, Goetze S, Friedman KP et al (2007) Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase (99m)Tc-sestamibi parathyroid scintigraphy. J Nucl Med 48:1084–1089
Harari A, Allendorf J, Shifrin A et al (2009) Negative preoperative localization leads to greater resource use in the era of minimally invasive parathyroidectomy. Am J Surg 197:769–773
Bergenfelz A, Lindblom P, Tibblin S et al (2002) Unilateral versus bilateral neck exploration for primary hyperparathyroidism: a prospective randomized controlled trial. Ann Surg 236:543–551
Acknowledgments
We thank Ms. Catherine Y. Jones for her administrative assistance. Dr. Kouniavsky received grants from the Israel Cancer Association and American Physicians Fellowship for Medicine in Israel.
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper article is from the Scientific Papers Session in Endocrine Surgery at the 2009 ACS Clinical Congress.
Rights and permissions
About this article
Cite this article
Neychev, V.K., Kouniavsky, G., Shiue, Z. et al. Chasing “Shadows”: Discovering the Subtleties of Sestamibi Scans to Facilitate Minimally Invasive Parathyroidectomy. World J Surg 35, 140–146 (2011). https://doi.org/10.1007/s00268-010-0800-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-010-0800-1