
Abstract
Objectives
The objective of this study was to evaluate by cross-sectional imaging the prevalence and degree of cortical scalloping by small eccentric chondromas correlated with histologic diagnosis and patient history.
Materials and methods
From 122 patients with histologically proven enchondromas and two patients without histology but with radiologic and clinical follow-up, 11 patients with small, eccentrically located chondromas in the long bones had cross-sectional imaging available. The lesions were evaluated for location, size, presence, and degree of cortical scalloping. The patient’s medical charts and microscope slides were reviewed for relevant clinical history, clinical management, and histology.
Results
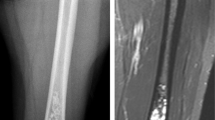
The chondromas ranged in size from 1.6 to 3.8 cm (mean 2.3 cm). Two lesions were located in the proximal femoral diaphysis, two in the distal femoral diaphysis, six in the distal femoral metaphysis, and one in the proximal tibial epimetaphysis. The lesions were curetted due to diagnostic uncertainty, continued pain, marked radiologic cortical penetration, or due to patient insistence on biopsy. All 11 lesions were benign, nine histologically, and two by stability over 4 and 7 years. The prevalence of cortical scalloping among eccentric chondromas was 100%. Cortical scalloping or occupancy ranged from 50 to 100% (mean 75%).
Conclusions
All small eccentric chondromas in this study were associated with an appearance of cortical scalloping of varying degree. All curetted lesions were histologically bland without nuclear atypia. Based on the benign histology of nine lesions and lack of growth of two lesions over several years, the degree of cortical scalloping is felt to be a result of lesion location within the endosteum rather than biological activity or malignancy.






Similar content being viewed by others


References
Bauer TW, Dorfman HD, Latham JT. Periosteal chondroma: a clinicopathologic study of 21 cases. Am J Surg Pathol. 1982; 6: 631–638.
Flemming DJ, Murphey MD. Enchondroma and chondrosarcoma. Semin Musculoskelet Radiol. 2000; 4: 59–71.
Walden MJ, Murphey MD, Vidal JA. Incidental enchondromas of the knee. AJR Am J Roentgenol. 2008; 190: 1611–1615.
Brien EW, Mirra JM, Kerr R. Benign and malignant cartilage tumors of bone and joint: their anatomic and theoretical basis with an emphasis on radiology, pathology and clinical biology. I. The intramedullary cartilage tumors. Skelet Radiol. 1997; 26: 325–353.
Skeletal Lesions Interobserver Correlation among Expert Diagnosticians (SLICED) Study Group. Reliability of histopathologic and radiologic grading of cartilaginous neoplasms in long bones. J Bone Joint Surg Am. 2007; 89: 2113–2123.
Murphey MD, Flemming DJ, Boyea SR, Bojescul JA, Sweet DE, Temple HT. Enchondroma versus chondrosarcoma in the appendicular skeleton: differentiating features. Radiographics. 1998; 18: 1213–1237.
Kendell SD, Collins MS, Adkins MC, Sundaram M, Unni KK. Radiographic differentiation of enchondroma from low-grade chondrosarcoma in the fibula. Skeletal Radiol. 2004; 33: 458–466.
Weiner SD. Enchondroma and chondrosarcoma of bone: clinical, radiologic, and histologic differentiation. Instr Course Lect. 2004; 53: 645–649.
Lucas DR, Bridge JA. Chondromas: enchondroma, periosteal chondroma and enchondromatosis. In: Fletcher CDM, Unni KK, Mertens F, editors. WHO classification of tumours: pathology and genetics. Tumours of soft tissue and bone. Lyon: IARC; 2002: 237–240.
Dorfman HD, Czerniak B. Benign cartilage lesions. In: Dorfman HD, Czerniak B, editors. Bone tumors. St. Louis: Mosby; 1998: 253–275.
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper was presented by the first author at the 35th annual members meeting of the International Skeletal Society, New Delhi, India, October 2008.
Rights and permissions
About this article
Cite this article
Bui, K.L., Ilaslan, H., Bauer, T.W. et al. Cortical scalloping and cortical penetration by small eccentric chondroid lesions in the long tubular bones: not a sign of malignancy?. Skeletal Radiol 38, 791–796 (2009). https://doi.org/10.1007/s00256-009-0675-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-009-0675-0