
Abstract
Summary
Evaluation of hospitalizations in a 70+ population showed that hip fractures (HF) were associated with a significant increase in the utilization of inpatient care for a lengthy period. Hospital days attributable to several diagnostic classes still exceeded both prefracture and population levels in the second year after HF.
Introduction
The goal was to assess effects of HF on the inpatient care utilization.
Methods
The study covered HF patients and the 70+general population (26,000) living in Central Finland. Hospitalization data categorized by the ICD-10 main classes were obtained from the nationwide discharge register.
Results
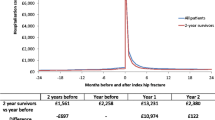
In 2002–2003, 498 residents (mean age 82 SD 7, 74.9% women) of the study area sustained HF. Among them, the number of hospital days was 23, 107, and 52 per person-year in the prefracture, first and second postfracture year, respectively. In the 70+ general population, the number was constantly 11 per year. The age- and gender-adjusted rate ratio of hospital days between the two groups was 1.30 (95% CI 1.27 to 1.32), 6.91 (95% CI 6.85 to 7.00), and 3.61 (95% CI 3.55 to 3.67) for the prefracture, first and second postfracture year, respectively. Hospital days due to injuries were more prevalent in the HF group throughout the period. Moreover, excess of days was seen in six other diagnostic classes in the first and in four classes in the second postfracture year.
Conclusions
Hospital days in HF patients still exceeded both the prefracture and population levels in the second year after HF. Days attributable to several other causes than HF itself became also more prevalent indicating that HF can steeply decrease patients’ coping capacity and launch a cascade of impairments in the function of different organ systems.


Similar content being viewed by others

References
Johnell O, Kanis J (2005) Epidemiology of osteoporotic fractures. Osteoporos Int 16:S3–S7
Marks R, Allegrante JP, MacKenzie CR et al (2003) Hip fractures among the elderly: causes, consequences and control. Ageing Res Rev 2:57–93
Kanis J, Oden A, Johnell O et al (2003) The components of excess mortality after hip fracture. Bone 32:468–473
Wiktorowics ME, Goeree R, Papaioannou A et al (2001) Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteoporos Int 12:271–278
Braithwaite RS, Col NF, Wong JB (2003) Estimating hip fracture morbidity, mortality and costs. J Am Ger Soc 51:364–370
Wolinsky FD, Fitzgerald JF, Stump TE (1997) The effect of hip fracture on mortality, hospitalization, and functional status: a prospective study. Am J Public Health 87:389–403
American Geriatrics Society, British Geriatrics Society, American Academy of Orthopaedic Surgeons Panel on Falls Prevention (2001) Guideline for the prevention of falls in older persons. J Am Ger Soc 49:664–672
Close J, Ellis M, Hooper R et al (1999) Prevention of falls in the elderly trial (PROFET): a randomised controlled trial. Lancet 353:93–97
Sund R, Nurmi-Lüthje I, Lüthje P et al (2007) Comparing properties of audit data and routinely collected register data in case of performance assessment of hip fracture treatment in Finland. Methods Inf Med 46:558–566
Gissler M, Haukka J (2004) Finnish health and social welfare registers in epidemiological research. Norsk Epidemiologi 14:113–120
Keskimäki I, Aro A (1991) Accuracy of data on diagnoses, procedures and accidents in the Finnish Hospital Discharge Register. Int J Health Sci 2:15–21
Tolonen H, Salomaa V, Torppa J, Sivenius J, Immonen-Räihä P, Lehtonen A (2007) The validation of the Finnish Hospital Discharge Register and Causes of Death Register data on stroke diagnoses. Eur J Cardiovasc Prev Rehabil 14:380–385
Lönnroos E, Kautiainen H, Karppi P et al (2006) Increased incidence of hip fractures. A population-based study in Finland. Bone 39:623–627
ICD 10, International statistical classification of diseases and related health problems, tenth revision. World Health Organization, Geneva
Lönnroos E, Kautiainen H, Karppi P et al (2007) Incidence of second hip fractures. A population-based study. Osteoporos Int 18:1279–1285
Hardin J, Hilbe J (2007) Generalized linear models and extensions, 2nd ed. Stata
Pande I, Scott DL, O’Neill TW et al (2006) Quality of life, morbidity and mortality after low trauma hip fracture in men. Ann Rheum Dis 65:87–92
Magaziner J, Lydick E, Hawkes W et al (1997) Excess mortality attributable to hip fracture in white women aged 70 years and older. Am J Public Health 87:1630–1636
Fransen M, Woodward M, Norton R et al (2002) Excess mortality or institutionalization after hip fracture: men are at greater risk than women. J Am Ger Soc 50:685–690
Klotzbuecher CM, Ross PD, Landsman PB et al (2000) Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15:721–739
Kanis JA, Johnell O, De Laet C et al (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–382
Lundström M, Edlund A, Bucht G et al (2003) Dementia after delirium in patients with femoral neck fractures. J Am Geriatr Soc 51:1002–1006
Edlund A, Lundström M, Brännström B et al (2001) Delirium before and after operation for femoral neck fracture. J Am Geriatr Soc 49:1335–1340
Rahkonen T, Luukkainen-Markkula R, Paanila S et al (2000) Delirium episode as a sign of undetected dementia among community dwelling elderly subjects: a 2 year follow up study. J Neurol Neurosurg Psychiatry 69:519–521
Gruber-Baldini AL, Zimmerman S, Morrison RS et al (2003) Cognitive impairment in hip fracture patients: timing of detection and longitudinal follow-up. J Am Geriatr Soc 51:1227–1236
Lenze EJ, Munin MC, Skidmore ER et al (2007) Onset of depression in elderly persons after hip fracture: implications for prevention and early intervention of late-life depression. J Am Geriatr Soc 55:81–86
Dolan MM, Hawkes WG, Zimmerman SI et al (2000) Delirium on hospital admission in aged hip fracture patients: prediction of mortality and 2-year functional outcomes. J Gerontol A Biol Sci Med Sci 55:M527–M534
The SOTKAnet Indicator Bank maintained by National Research and Development Centre for Welfare and Health (STAKES). Population health status, individuals entitled to special refunds for cardiovascular drugs. http://uusi.sotkanet.fi/portal/page/portal/etusivu/hakusivu. Accessed March 17th, 2008
Vestergaard P, Rejnmark L, Mosekilde L (2007) Increased mortality in patients with a hip fracture-effect of pre-morbid conditions and post-fracture complications. Osteoporos Int 18:1583–1593
Tosteson AN, Gottlieb DJ, Radley DC et al (2007) Excess mortality following hip fracture: the role of underlying health status. Osteoporos Int 18:1463–1472
Salter AE, Khan KM, Donaldson MG et al (2006) Community-dwelling seniors who present to the emergency department with a fall do not receive Guideline care and their fall risk profile worsens significantly: a 6-month prospective study. Osteoporos Int 17:672–683
Peng EWK, Elnikety S, Hatrick NC (2006) Preventing fragility hip fracture in high risk groups: an opportunity missed. Postgrad Med J 82:528–531
Giangregorio L, Papaioannou A, Cranney A et al (2006) Fragility fractures and the osteoporosis care gap: an international phenomenon. Semin Arthritis Rheum 35:293–305
Ganz D, Bao Y, Schekelle P, Rubenstein L (2007) Will my patient fall? JAMA 297:77–86
Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH (2003) Interventions for preventing falls in elderly people. Cochrane Database Syst Rev 4:CD000340
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lönnroos, E., Kautiainen, H., Sund, R. et al. Utilization of inpatient care before and after hip fracture: a population-based study. Osteoporos Int 20, 879–886 (2009). https://doi.org/10.1007/s00198-008-0752-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0752-6