
Abstract
Objective
To explore the relationship between hospital mortality and time spent by patients on hospital wards before admission to the intensive care unit (ICU).
Design
Observational study of prospectively collected data.
Setting
Participating intensive care units within the North East Thames Regional Database.
Patients and participants
Patients, 7,190, admitted to ICU from the hospital wards of 24 hospitals.
Interventions
None.
Measurements and results
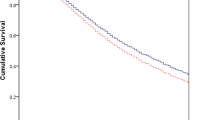
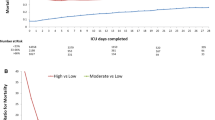
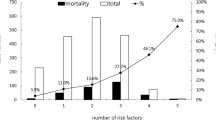
Of ICU admissions from the wards, 40.1% were in hospital for more than 3 days and 11.7% for more than 15 days. ICU patients who died in hospital were in-patients longer (p=0.001) before admission (median 3 days; interquartile range 1–9) than those discharged alive (median 2 days; interquartile range 1–5). Hospital mortality increased significantly (p<0.0001) in relation to time on hospital wards before ICU: 47.1% (standardised mortality ratio 1.09) for patients in hospital 0–3 days before ICU admission up to 67.2% (standardised mortality ratio 1.39) for patients on the wards for more than 15 days before ICU. Length of stay before ICU admission was an independent predictor of hospital mortality (odds ratio per day 1.019; 95% confidence interval 1.014–1.024). There were significant differences (p<0.001) in patient age, APACHE II score and predicted mortality in relation to time on wards before ICU admission.
Conclusions
Mortality was high among patients admitted from the wards to ICU; many were inpatients for days or weeks before admission. The longer these patients were in hospital before ICU admission, the higher their mortality. Patients with delayed admission differed in some respects compared to those admitted earlier.

Similar content being viewed by others
References
Goldhill DR, Sumner A (1998) Outcome of intensive care patients in a group of British intensive care units. Crit Care Med 26:1337–1345
Goldfrad C, Rowan K (2000) Consequences of discharges from intensive care at night. Lancet 355:1138–1142
Daly K, Beale R, Chang RW (2001) Reduction in mortality after inappropriate early discharge from intensive care unit: logistic regression triage model. BMJ 322:1274–1276
Goldhill DR, McNarry A (2002) Intensive Care Outreach Services. Curr Anaesth Crit Care 13:356–361
Goldhill DR, McNarry AF (2004) Physiological abnormalities in early warning scores are related to mortality in adult inpatients. Br J Anaesth 92:882–884
Goldhill DR, Sumner A (1998) APACHE II, data accuracy and outcome prediction. Anaesthesia 53:937–943
Knaus WA, Draper EA, Wagner DP, Zimmerman JE (1985) APACHE II: a severity of disease classification system. Crit Care Med 13:818–829
Gardner MJ, Altman DG (1989) Statistics with confidence. BMJ, London pp 59–60
Buist MD, Jarmolowski E, Burton PR, Bernard SA, Waxman BP, Anderson J (1995) Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary-care hospital. Med J Aust 171:22–25
Franklin C, Mathew J (1994) Developing strategies to prevent inhospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med 22(2):244–247
Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL (1990) Clinical antecedents to in-hospital cardiopulmonary arrest. Chest 98:1388–1392
George ALJ, Folk BP, Crecelius PL, Campbell WB (1989) Pre-arrest morbidity and other correlates of survival after in-hospital cardiopulmonary arrest. Am J Med 87:28–34
Goldhill DR, White SA, Sumner A (1999) Physiological values and procedures in the 24 hours before ICU admission from the ward. Anaesthesia 54:529–534
Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV (2002) Effects of a medical emergency team on reduction of incidence and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ 324:387–390
Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart GK, Opdam H, Silvester W, Doolan L, Gutteridge G (2003) A prospective before-and-after trial of a medical emergency team. Med J Aust 179:283–287
Ball C, Kirkby M, Williams S (2003) Effect of the critical care outreach team on patient survival to discharge from hospital and readmission to critical care: non-randomised population based study. BMJ 327:1014–1017
Bennett-Guerrero E, Hyam JA, Shaefi S, Pyrtherch DR, Sutton GL, Weaver PC, Mythen MG, Grocott MP, Parides MK (2003) Comparison of P-POSSUM risk-adjusted mortality rates after surgery between patients in the USA and the UK. Br J Surg 90:1593–1598
McNarry AF, Goldhill DR (2004) Intensive care admission decisions for a patient with limited survival prospects: a questionnaire and database analysis. Intensive Care Med 30:325–330
Author information
Authors and Affiliations
Corresponding author
Additional information
Preliminary analysis of this data was presented in abstract at the Intensive Care Society (UK) State of the Art Scientific Meeting in London, December 2001.
Electronic Supplementary Material
Rights and permissions
About this article
Cite this article
Goldhill, D.R., McNarry, A.F., Hadjianastassiou, V.G. et al. The longer patients are in hospital before Intensive Care admission the higher their mortality. Intensive Care Med 30, 1908–1913 (2004). https://doi.org/10.1007/s00134-004-2386-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2386-2