
Abstract.
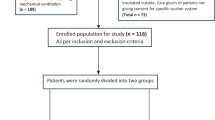
Objective: To determine whether selective decontamination locally in the subglottic area (SDSA) reduces tracheal colonization and prevents ventilator-associated pneumonia (VAP) in patients with multiple trauma. Design and setting: A prospective randomized, controlled, clinical study in a 14-bed general intensive care unit of a university hospital. Patients: 79 consecutive multiple trauma patients admitted to the ICU who were expected to be mechanically ventilated for more than 5 days; 61 patients completed the protocol. Intervention: Patients were randomly assigned to receive SDSA using a continuous infusion of a suspension containing three nonabsorbable antibiotics (polymyxin, tombramycin, and amphotericin B; n=30) or placebo (n=31). Measurements: The incidence of bronchial and gastric colonization and the number of cases of VAP were recorded. Gastric fluid and tracheal secretion cultures were obtained soon after intubation and thereafter every 4 days. Etiological diagnosis of VAP was based on samples taken by a specific protected double catheter set. Results: VAP developed in 5 of 30 (16.6%) patients receiving SDSA and 16 of 31 (51.6%) patients receiving placebo. Negative bronchial secretion cultures were found in 14 of 30 (46.6%) patients in the SDSA group and in only 3 of 31 (9.6%) patients in the control group. No patient with negative bronchial secretion culture developed VAP. No significant differences in outcome were found. Conclusions: The SDSA is an effective and safe type of chemoprophylaxis against tracheal colonization and can significantly reduce the incidence of VAP in mechanically ventilated patients with multiple trauma.
Article PDF
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Electronic Publication
Rights and permissions
About this article
Cite this article
Pneumatikos, I., Koulouras, V., Nathanail, C. et al. Selective decontamination of subglottic area in mechanically ventilated patients with multiple trauma. Intensive Care Med 28, 432–437 (2002). https://doi.org/10.1007/s00134-002-1238-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-002-1238-1