
Abstract
Purpose
Minimum effective anaesthetic concentration (MEAC) of lidocaine for spinal anaesthesia, defined as the concentration at which a spinal anaesthetic agent produces surgical anaesthesia within 20 min of administration in 50% of patients, was determined in a randomised, double-blind study in young patients undergoing knee and ankle surgery.
Methods
Using the combined spinal-epidural technique, 48 or 72 mg hyperbaric lidocaine containing dextrose 7.5% was administered intrathecally to 43 patients at concentrations ranging from 0.2–0.9%. The choice of lidocaine concentration was determined by Dixon’s up-and-down method, Complete anaesthesia was defined as: ( I ) pinprick anaesthesia at or higher than T12, (2) anaesthesia to transcutaneous tetanic electric stimulation (50 Hz at 60 mA for five seconds) in the knees and (3) complete leg paralysis; all occurring in both lower extremities within 20 min. Epidural anaesthesia was initiated if anaesthesia was incomplete.
Results
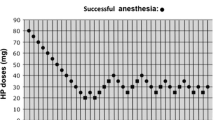
In the 48 mg group, MEAC was 0.54% (95% Cl-0.21–0.87). Anaesthetic effect was variable with mean duration of anaesthesia of 29 min (range: 20–50 min) and maximum pinprick sensory level ranging from T2-T10. In the 72 mg group, successful anaesthesia was achieved consistently at a concentration of 0,3%, i.e., MEAC was < 0.3%. Mean duration of complete anaesthesia was 46 min (range: 30–60 min) with maximum sensory level from T3–T8.
Discussion
Spinal anaesthesia can be accomplished with very dilute lidocaine solutions (< 0.9%). The value of MEAC is dose-dependent, i.e., complete anaesthesia can be accomplished with lower concentrations by increasing the dose of spinal anaesthetic administered.
Résumé
Objectif
Déterminer la concentration anesthésique minimale efficace (CAME) de lidocaïne pour anesthésie rachidienne. Cette CAME est définie comme la concentration à laquelle l’agent anesthésique produit une anesthésie chirurgicale chez 50% des patients dans un délai de 20 minutes après l’injection. L’étude a été réalisée à double insu et selon une distribution aléatoire chez de jeunes patients soumis à une chirurgie de la cheville ou du genou.
Méthodes
Utilisant une technique combinée de rachi-épidurale, de la lidocaïne rendue hyperbare avec du dextrose 7.5% a été administrée en sous arachnoïdien à raison de 48 ou 72 mg chez 43 patients en concentrations variant de 0,2 à 0,9%. Le choix des concentrations de lidocaïne était déterminé par la méthode des hauts et bas de Dixon, Une anesthésie complète était définie par : I-une anesthésie à la piqûre à Tl2 ou plus haut; 2-une anesthésie à une stimulation électrique tétanique percutanée au niveau des genoux (50 Hz, 60 mA et 5 sec); 3-une paralysie complète des jambes; toutes ces manifestations devaient être présentes aux deux jambes en moins de 20 minutes. Si l’anesthésie étart: incomplète, la relève était assurée par l’épidurale.
Résultats
Dans le groupe 48 mg, la CAME était de 0,54% (intervalle de confiance 95%–0,2l à 0,87%). L’effet anesthésique était variable avec une durée moyenne de 29 min. (écart 20–50 min.) et un niveau senstif à l’aiguille variant de T2 à Tl0. Dans le groupe 72 mg, une anesthésie adéquate était atteinte de façon fiable à une concentration de 0,3%, c’est-à-dire que la CAME était < 0,3%. La durée moyenne de l’anesthésie complète était de 46 minutes (écart 30–60 min.) avec un niveau sensitif maximal variant de T3 à T8.
Discussion
L’anesthésie rachidienne peut être réussie avec des solutions de lidocaïne très diluées (< 0,9%), La valeur de la CAME dépend de la dose, i.e., une anesthésie complète peut être réalisée avec des concentrations plus faibles à condition d’augmenter la dose d’anesthésique local administré.
Article PDF
Similar content being viewed by others


References
Fink BR. History of neural blockade.In: Cousins MJ, Bridenbaugh PO (Eds.). Neural Blockade in Clinical Anesthesia and Management of Pain, 2nd ed. Philadelphia: Lippincott, 1988: P3–24.
Phillips OC, Ebner Nelson AT, Black MH. Neurologic complications following spinal anesthesia with lidocaine: a propcctivc review of 10,440 cases. Anesthesiology 1968; 30: 284–9.
Rigler ML, Drasner K, Krejcie TC, et al. Cauda equina syndrome after continuous spinal anesthesia. Anesth Analg 1991; 72: 275–81.
Schell RM, Brauer FS, Cote DJ, Applegate RL II. Persistent sacral nerve root deficits after continuous spinal anaesthesia. Can J Anaesth 1991; 38: 908–11.
Schneider M, Ettlin T, Kaufinann M, et al. Transient neurologic toxicity after hyperbaric subarachnoid anesthesia with 5% lidocaine. Anesth Analg 1993; 76: 1154–7.
Lambert LA, Lambert DH, Strichartz GR. Irreversible conduction block in isolated nerve by high concentrations of local anesthetics. Anesthesiology 1994; 80: 1082–93.
Bainton CR, Strichartz GR. Concentration dependence of Edocaine-induced irreversible conduction loss in frog nerve. Anesthesiology 1994; 81: 657–67.
Kalichman MW, Powell HC, Myers RR. Quantitative histologie analysis of local anesthetic-induced injury to rat sciatic nerve. J Pharmacol Exp Ther 1989; 250: 406–13.
Drasner K, Rigler ML, Sessler DI, Stoller ML. Caude equina syndrome following intended epidural anesthesia. Anesthesiology 1992; 77: 582–5.
Toft P, Bruun-Mogensen Chr, Kristensen J, Hole P. A comparison of glucose-free 2% lidocaine and hyperbaric 5% lidocaine for spinal anaesthesia. Acta Anaesthesiol Scand 1990; 34: 109–13.
Kristensen J, Helbo-Hansen HS, Toft P, Hole P. Spinal anaesthesia with glucose-free 2% lignocaine. Effect of different volumes. Acta Anaesthesiol Scand 1989; 33: 53–7.
Manica VS, Bader AM, Fragneto R, Gilbertson L, Datta S. Anesthesia for in vitro fertilization: a comparison of 1.5% and 5% lidocaine for ultrasonically guided oocyte retrieval. Anesth Analg 1993; 77: 453–6.
Kumar A, Bala I, Bhukal I, Singh H. Spinal anaesthesia with lidocaine 2% for Caesarean section. Can J Anaesth 1992; 39: 915–9.
Bodily MN, Carpenter RL, Owens BD. Lidocaine 0.5% spinal anaesthesia: a hypobaric solution for short-stay perirectal surgery. Can J Anaesth 1992; 39: 770–3.
Chan VWS, Garcia J, Drasner K. A comparative study of hyperbaric spinal lidocaine 0.5% versus 5% for urologie surgery. Anesthesiology 1995; 83: A777.
Dixon WJ, Masscy FJ Jr. Introduction to Statistical Analysis, 4th ed. New York: McGraw Hill, 1983; 428–49.
Petersen-Felix S, Zbinden AM, Fischer M, Thomson DA. Isoflurane minimum alveolar concentration decreases during anesthesia and surgery. Anesthesiology 1993; 79: 959–65.
Hampl KF, Schneider MC, Pargger H, Gut J, Drewe J, Drasner K. A similar incidence of transient neurologic symptoms after spinal anesthesia with 2% and 5% lidocaine. Anesth Analg 1996; 83: 1051–4.
Columb MO, Lyons G, Naughton NN, et al. Estimation of the minimum local analgesic concentration (MLAC) of epidural chloroprocaine hydrochloride in labor. Reg Anesth 1995; 20: S96.
de Jong RH. Local Anesthetics, 1st ed. St. Louis: Mosby-Year Book, 1994.
Liu S, Pollock JE, Mulroy MF, Alien HW, Neal JM, Carpenter RL Comparison of 5% with Dextrose, 1.5% with Dextrose, and 1.5% Dextrose-free lidocaine solutions for spinal anesthesia in human volunteers. Anesth Analg 1995; 81: 697–702.
Katzman R, Hussey F. A simple constant-infusion manomctric test for measurement of CSF absorption. I. Rationale and method. Neurology 1970; 20: 534–44.
Greene NM. Distribution of local anesthetic solutions within the subarachnoid space. Anesth Analg 1985; 64: 715–30.
Wildsmith JAW, McClure JH, Brown DT, Scott DB. Effects of posture on the spread of isobaric and hyperbaric amethocaine. Br J Anaesth 1981; 53: 273–8.
Axelsson KH, Edström HH, Sundberg AEA, Widman GB. Spinal anaesthesia with hyperbaric 0.5% bupivacaine: effects of volume. Acta Anaesthesiol Scand 1982; 26: 439–45.
Sundnes KO, Vaagenes P, Skretting P, Lind B, Edström HH. Spinal analgesia with hyperbaric bupivacaine: effects of volume of solution. Br J Anaesth 1982; 54: 69–73.
Van Zundert AAJ, Grouls RJE, Karsten HHM, Lambert DH. Spinal anesthesia. Volume or concentrationwhat matters? Reg Anesth 1996; 21: 112–8.
Bengtsson M, Edström HH, Löfström JB. Spinal analgesia with bupivacaine, mepivacaine and tetracaine. Acta Anaesthesiol Scand 1983; 27: 278–83.
Sheskey MC, Rocco AG, Bizzarri-Schmid M, Francis DM, Edstrom H, Covino BG. A dose-response study of bupivacaine for spinal anesthesia. Anesth Analg 1983; 62: 931–5.
de Jong RH. Last round for a “heavyweight?” Anesth Analg 1994; 78: 3–4.
Carpenter RL. Hypcrbaric lidocainc spinal anesthesia: do we need an alternative? Anesth Analg 1995; 81: 1125–8.
Sjösröm S, Bläss J. Severe pain in both legs after spinal anaesthesia with hyperbaric 5% lignocaine solution. Anaesthesia 1994; 49: 700–2.
Pinczower GR, Chadwick HS, Woodland R, Lowmiller M. Bilateral kg pain following lidocaine spinal anaesthesia. Can J Anaesth 1995; 42: 217–20.
Rodriguez-Chinchilla R, Rodgríguez-Pont A, Pintanel T, Vidal-Lôpez F. Bilateral severe pain at L3-4 after spinal anaesthesia with hyperbaric 5% lignocaine. Br J Anaesth 1996; 76: 328–9.
Fenerty J, Sonner J, Sakura S, Drasner K. Transient radicular pain following spinal anesthesia: review of the literature and report of a case involving 2% lidocaine. Int J Obstet Anesth 1996; 5: 32–5.
Brasnsr K, Sakura S, Chan VWS, Bollen AW, Ciriales R. Persistent sacral sensory deficit induced by intrathecal local anesthetic infusion in the rat. Anesthesiology 1994; 80: 847–52.
Pollock JE, Liu SS, Neal JM, Stephenson CA. The importance of lidocaine concentration in the development of transient radiocular irritation. Reg Anesth 1997;22. S85.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Peng, P.W.H., Chan, V.W.S. & Perlas, A. Minimum effective anaesthetic concentration of hyperbaric lidocaine for spinal anaesthesia. Can J Anaesth 45, 122–129 (1998). https://doi.org/10.1007/BF03013249
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013249