
Abstract
Purpose
To compare the efficacy of propofol in a subhypnotic dose (10 mg iv), droperidol (1.25 mg iv), or metoclopramide (10 mg iv) in the treatment of PONV in the post anaesthesia care unit (PACU).
Methods
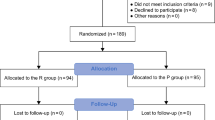
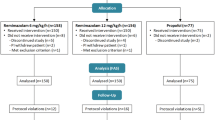
In a prospective, randomized, double-blind protocol, over four months, all eligible inpatients and outpatients were asked to give their consent to be included in the study should they suffer PONV in the PACU. They received a standardized general anaesthetic without any prophylactic antiemetic drug. In the recovery room, patients complaining of persistent nausea (lasting more than ten minutes) and/or experiencing at least two episodes of retching or vomiting were given one of the three study drugs. Recurrence of retching or vomiting was recorded for 60 min after administration of the study drug and nausea severity was assessed on a visual analog scale. Patients still complaining of PONV 30 min after administration of the study drug received a rescue medication (dimenhydrinate).
Results
Seventy-eight patients received one of the study drugs. The recurrence of retching or vomiting was higher with propofol (58%) than with droperidol (4%) or metoclopramide (24%) (P <0.00l). More patients who received propofol needed the rescue medication (54%) than those who received droperidol (15%) or metoclopramide (28%) (P <0.02). No difference was observed in nausea severity.
Conclusion
A subhypnotic dose of propofol (10 mg iv) is less effective than the conventional antiemetic drugs droperidol and metoclopramide for the treatment of PONV in the PACU.
Résumé
Objectif
Comparer le propofol à dose subhypnotique (10 mg iv), le dropéridol (1,25 mg iv) et le métoclopramide (10 mg iv) pour le traitement des nausées et vomissements postopératoires (NVP) à la salle de réveil.
Méthode
Pendant quatre mois, tous les patients éligibles ont été solicités et ont consenti à participer à une étude prospective, randomisée et en double aveugle dans l’éventualité de NVP à ta salle de réveil. L’anesthésie était standardisée et ne comportait pas d’antiémétiques. A la salle de réveil, les patients qui se plaignaient de nausées persistantes (dix min et plus) et/ou qui éprouvaient au moins deux épisodes d’efforts de vomissements ou des vomissements ont reçu un des trois médicaments. La récidive des efforts de vomissements ou des vomissements a été notée pendant 60 min après l’administration du médicament à l’étude et l’importance de la nausée a été évaluée sur une échelle visuelle analogue. Les patients qui continuaient de se plaindre de NVP 30 min après l’administration d’un des médicaments étudiés ont reçu un médicament de sauvetage (dimenhydrinate).
Résultats
Soixante-dix-huit patients ont reçu un des médicaments étudiés. La récidive d’efforts de vomissements et de vomissements a été plus élevée avec le propofol (58%) qu’avec le dropéridol (4%) et le métoclopramide (24%) (P < 0.001). Les patients ayant reçu le propofol ont été plus nombreux (54%) à recevoir le médicament de sauvetage que ceux qui avaient reçu le dropéridol (15%) ou le métoclopramide (28%) (P < 0,02). La gravité de la nausée pas été différente entre les groupes.
Conclusion
La dose subhypnotique de propofol (10 mg iv) est moins efficace que les antiémétiques habituels dropéridol et métoclopramide pour traiter les NVP à la salle de réveil.
Article PDF
Similar content being viewed by others

References
Hines R, Barash PG, Watrous G, O’Connor T. Complications occurring in the postanesthesia care unit: a survey. Anesth Analg 1992; 74: 503–9.
Gold BS, Kitz DS, Lecky JH, Neuhaus JM. Unanticipated admission to the hospital following ambulatory surgery. JAMA 1989;262: 3008–10.
Trépanier CA, Isabel L. Perioperative gastric aspiration increases postoperative nausea and vomiting in outpatients. Can J Anaesth 1993; 40: 325–8.
Watcha MF, White PF. Postoperative nausea and vomiting. Its etiology, treatment and prevention. Anesthesiology 1992; 77: 162–84.
Palazzo MGA, Strunin L. Anaesthesia and emesis. I: etiology. Can Anaesth Soc J 1984; 31: 178–87.
Cohen MM, Duncan PG, DeBoer DP, Tweed WA. The postoperative interview: assessing risk factors for nausea and vomiting. Anesth Analg 1994; 78: 7–16.
Kapur PA. The big “little problem” (Editorial). Anesth Analg 1991; 73: 243–5.
Borgeat A, Wilder-Smith OHG, Saiah M, Rifat K. Subhypnotic doses of propofol possess direct antiemetic properties. Anesth Analg 1992; 74: 539–41.
Bodner M, White PF. Antiemetic efficacy of ondansetron after outpatient laparoscopy. Anesth Analg 1991; 73: 250–4.
Korttila K. The study of postoperative nausea and vomiting. Br J Anaesth 1992; 69 (suppl): 20S-23S.
Doze VA, Shafer A, White PF. Propofol-nitrous oxide versus thiopental-isoflurane-nitrous oxide for general anesthesia. Anesthesiology 1988; 69: 63–71.
Watcha MF, Simeon RM, White PF, Stevens JL. Effect of propofol on the incidence of postoperative vomiting after stabismus surgery in pediatric outpatients. Anesthesiology 1991;75: 204–9.
McCollum JSC, Milligan KR, Dundee JW. Forum. The antiemetic action of propofol. Anaesthesia 1988; 43: 239–40.
Reimer EJ, Montgomery CJ, Bevan JC, Merrick PM, Blackstock D, Popovic V. Propofol anaesthesia reduces early postoperative emesis after paediatric strabismus surgery. Can J Anaesth 1993; 40: 927–33.
Andrews PLR. Physiology of nausea and vomiting. Br J Anaesth 1992; 69 (suppl): 2S-19S.
Borgeat A, Wilder-Smith OHG, Suter PM. The nonhypnotic therapeutic applications of propofol. Anesthesiology 1994; 80: 642–56.
DiFlorio T. Is propofol a dopamine antagonist? (Letter). Anesth Analg 1993; 77: 200–1.
Borgeat A, Bonnefoi H, Tramer M, Bischoff P, Wilder-Smith OHG, Rifat K. Does propofol possess antidopaminergic properties? Anesth Analg 1994; 78: S43.
Khalil SN, Berry JM, Howard G, et al. The antiemetic effect of lorazepam after outpatient strabismus surgery in children. Anesthesiology 1992; 77: 915–9.
Östman PL, Faure E, Glosten B, Kernen M, Robert MK, Bedwell S. Is the antiemetic effect of the emulsion formulation of propofol due to the lipid emulsion? Anesth Analg 1990;71: 536–40.
Sebel PS, Lowdon JD. Propofol: a new intravenous anesthetic. Anesthesiology 1989; 71: 260–77.
Borgeat A, Wilder-Smith O, Forni M, Suter PM. Adjuvant propofol enables better control of nausea and emesis secondary to chemotherapy for breast cancer. Can J Anaesth 1994; 41: 1117–9.
Melnick B, Sawyer R, Karambelkar D, Phitayakorn P, Uy NTL, Patel R. Delayed side effects of droperidol after ambulatory general anesthesia. Anesth Analg 1989; 69: 748–51.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Lacroix, G., Lessard, M.R. & Trépanier, C.A. Treatment of post-operative nausea and vomiting: comparison of propofol, droperidol and metoclopramide. Can J Anaesth 43, 115–120 (1996). https://doi.org/10.1007/BF03011251
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011251