
Abstract
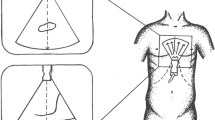
Aim of our study was to assess if the 2D-Echo transverse diameter of the left hepatic vein (LHV) obtained from the subcostal approach is correlated with invasive mean right atrial pressure (RAP). Thirty-two consecutive patients with acute myocardial infarction were studied by simultaneous 2D-Echo and right heart catheterization. LHV could be adequately imaged in 90% of patients. Mean RAP values at catheterization ranged from 0 to 15mmHg (mean 6±3.5 mmHg). A correlation was found between mean RAP and LHV diameter calculated after inspiration (r=0.81, SEE=1.54 mm, slope=0.71,p< 0.001) as well as after expiration (r=0.82, SEE=1.32mm, slope=0.62,p< 0.001) or during post-expiratory apnoea (r=0.85, SEE=1.3 mm, slope=0.71,p< 0.001). Moreover, percent increments of LHV diameter correlated well with percent changes of mean RAP during rapid infusion of 250–500 cc of saline in 4 patients (r=0.98,p< 0.001).
Thus, the 2D-Echo LHV diameter is a feasible measurement that seems to correlate well with invasive mean RAP over a wide range of mean RAP values in patients with myocardial infarction; the changes in LHV diameter correlate well with the percent increase in central venous pressure obtained with saline infusion. Underestimation of invasive RAP occurs when mean RAP value exceeds 12 mmHg and can be explained by limited venous compliance. However these preliminary results suggest that this method may represent a valid alternative to obtain a non invasive estimate of mean RAP with 2D-Echocardiography.
Similar content being viewed by others


References
Yock PG, Popp RL. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation 1984; 70: 657–62.
Feigenbaum H. Echocardiography. Philadelphia: Lea and Febiger, 1981: 218.
Moreno FLL, Hagan AD, Holmen JR, Pryor TA, Strickland RD, Castle CH. Evaluation of size and dynamics of the inferior vena cava as an index of right-sided cardiac function. Am J Cardiol 1984; 53: 579–85.
Mintz GS, Kotler MN, Parry WR, Iskandrian AS, Kane SA. Real-time vena caval ultrasonography: normal and abnormal findings and its use in assessing right-heart function. Circulation 1981; 64: 1018–25.
Gullace G, Savoia MT. Echocardiographic assessment of the inferior vena cava wall motion for studies of right heart dynamics and function. Clin Cardiol 1984; 7: 393–404.
Nakao S, Come PC, McKay RG, Ransil BJ. Effects of positional changes on inferior vena caval size and dynamics and correlations with right-sided cardiac pressure. Am J Cardiol 1987; 59: 125–32.
Kircher BJ, Himelman RB, Schiller NB. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol 1990; 66: 493–6.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Luca, L., Mario, P., Giansiro, B. et al. Non invasive estimation of mean right atrial pressure utilizing the 2D-Echo transverse diameter of the left hepatic vein. Int J Cardiac Imag 8, 191–195 (1992). https://doi.org/10.1007/BF01146837
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01146837