
Abstract
Objective
This study examines the effect of ADHD (attention deficit hyperactivity disorder) diagnosis and stimulant medication for ADHD treatment on child heart rate (HR) and blood pressure (BP) in a community sample compared to children without ADHD.
Methods
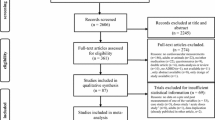
Data came from the HBEAT Study. From 49 schools, 2013 participants from southern Ontario in grades 5–8 were included. Linear regression analyses examined the effects of ADHD medications on systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate adjusting for age, sex and body mass index (BMI).
Results
Compared to non-ADHD children and adjusting for age, sex and BMI, children with ADHD on stimulant medication had a 12.3-bpm higher HR, and 3.0-mmHg higher SBP and DBP (all statistically significant). Children with ADHD on no stimulant medication had no differences in HR and BP compared to those children without a diagnosis of ADHD.
Conclusion
Stimulant medications used to treat ADHD are associated with elevated HR and higher BP. While it is unknown whether children on ADHD medications may be at risk for longer-term cardiovascular issues, this study supports the need to examine the long-term consequences of ADHD medication.
Résumé
Objectif
Examiner l’effet du diagnostic de TDAH (trouble déficitaire de l’attention avec hyperactivité) et des médicaments stimulants pour le traitement du TDAH sur la fréquence cardiaque et la pression artérielle des enfants d’un échantillon communautaire comparés aux enfants sans TDAH.
Méthode
Les données proviennent de l’étude HBEAT. Y ont participé 2013 élèves de la 5e à la 8e année fréquentant 49 écoles du Sud de l’Ontario. Par analyse de régression linéaire, nous avons examiné les effets des médicaments pour le traitement du TDAH sur la pression systolique, la pression diastolique et la fréquence cardiaque en apportant des ajustements selon l’âge, le sexe et l’indice de masse corporelle (IMC).
Résultats
Comparativement aux enfants sans TDAH et compte tenu de l’âge, du sexe et de l’IMC, les enfants avec TDAH qui prennent des médicaments stimulants ont une fréquence cardiaque plus élevée de 12,3 PPM et une pression systolique et diastolique plus élevée de 3 mmHg (tous ces résultats sont significatifs). La fréquence cardiaque et la pression artérielle des enfants avec TDAH qui ne prennent pas de médicaments stimulants ne sont pas différentes de celles des enfants sans diagnostic de TDAH.
Conclusion
Les médicaments stimulants pour le traitement du TDAH sont associés à une fréquence cardiaque élevée et à une pression artérielle supérieure. On ne sait pas si les enfants qui prennent des médicaments pour le traitement du TDAH courent des risques de maladies cardiovasculaires à long terme, mais notre étude confirme qu’il faut examiner les conséquences à long terme de la prise de médicaments pour le traitement du TDAH.
Similar content being viewed by others


References
Banach, A. M., Peralta-Huertas, J., Livingstone, K., Petrella, N., Klentrou, P., Faught, B., Wade, T. J., & O’Leary, D. (2010). Arterial distensibility is reduced in overweight pre- and early pubescent children. European Journal of Pediatrics, 169, 695–670.
Centers for Disease Control and Prevention. (2017). Attention deficit/hyperactivity disorder: data & statistics. Available at: https://www.cdc.gov/ncbddd/adhd/data.html. Accessed 21 Feb 2018.
Fitzgibbon, L. K., Coverdale, N. S., Philips, A. A., Shoemaker, J. K., Klentrou, P., Wade, T. J., Cairney, J., & O’Leary, D. D. (2012). The association between baroreflex sensitivity and blood pressure in children. Applied Physiology, Nutrition and Metabolism, 37, 301–301.
Hartiala, O., Magnussen, C. G., Kajander, S., Knuuti, J., Ukkonen, H., Saraste, A., et al. (2012). Adolescence risk factors are predictive of coronary artery calcification at middle age: cardiovascular risk in the Young Finns study. Journal of the American College of Cardiology, 60(15), 1362–1370.
Hausner, E., Fiszman, M. L., Haning, J., Harlow, P., Zornberg, G., & Sobel, S. (2008). Long-term consequences of drugs on the paediatric cardiovascular system. Food and Drug Administration, 12, 1083–1096.
Kavey, R. W., Daniels, S. R., Lauer, R. M., Atkins, D. L., Hayman, L. L., & Taubert, K. (2003). American Heart Association guidelines for primary prevention of atherosclerotic cardiovascular disease beginning in childhood. Circulation, 102, 1562–1566.
Kratochvil, C. J., Heiligenstein, J. H., Dittmann, R., Spencer, T. J., Biederman, J., Wernicke, J., et al. (2002). Atomoxetine and methyphenidate treatment in children with ADHD: a prospective, randomized, open-label trial. Journal of the American Academy of Child and Adolescent Psychiatry, 41(7), 776–784.
Magnussen, C. G., Smith, K. J., & Juonala, M. (2013). When to prevent cardiovascular disease? As early as possible: lessons from prospective cohorts beginning in childhood. Current Opinion in Cardiology, 28, 561–568.
Mattu, G. S., Heran, B. S., & Wright, J. M. (2004). Comparison of the automated non-invasive oscillometric blood pressure monitor (BpTRU) with the auscultatory mercury sphygmomanometer in a paediatric population. Blood Pressure Monitoring, 9(1), 39–45.
National Institutes of Health. (2000). National Institutes of Health Consensus Development Conference statement: diagnosis and treatment of attention-deficit/hyperactivity disorder (ADHD). J Am Acad Child Adolesc Psychiatry, 39, 182–193.
Phillips, A. A., Chirico, D., Coverdale, N. S., Fitzgibbon, L. K., Shoemaker, J. K., Wade, T. J., Cairney, J., & O’Leary, D. D. (2014). The association between arterial properties and blood pressure in children. Applied Physiology, Nutrition and Metabolism, 40, 72–78.
Samuels, J. A., Franco, K., Wan, F., & Sorog, J. M. (2006). Effects of stimulants on 24-hour ambulatory blood pressure in children with ADHD: A double-blind, randomized, cross-over trial. Paediatric Nephrology and Hypertension, 21, 92–95.
Szatmari, P., Offord, D. R., & Boyle, M. H. (1989). Ontario Child Healthy Study: prevalence of attention deficit disorder with hyperactivity. Journal of Child Psychology and Psychiatry, 30(2), 219–230.
Vlachopoulos, C., Aznaouridis, K., & Stefanadis, C. (2010). Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. Journal of the American College of Cardiology, 55(13), 1318–1327.
Winterstein, A. G., Gerhard, T., Shuster, J., Johnson, M., Zito, J. M., & Saidi, A. (2007). Cardiac safety of central nervous system stimulants in children and adolescents with attention-deficit/hyperactivity disorder. Paediatrics, 120, 1494–1500.
Woodgate, R. L., & Sigurdson, C. M. (2015). Building school-based cardiovascular health promotion capacity in youth: a mixed methods study. BMC Public Health, 15, 1–11.
Zuvekas, S., & Vitiello, B. (2008). Stimulant medication use in children: a 12-year perspective. American Journal of Psychiatry, 1, 1–2.
Funding
This study was funded by the Heart and Stroke Foundation of Ontario (SDA2367).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by both the university and the school district research ethics board. Informed written consent was obtained from the parents and verbal assent was obtained from the children to participate in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
St. Amour, M.D., O’Leary, D.D., Cairney, J. et al. What is the effect of ADHD stimulant medication on heart rate and blood pressure in a community sample of children?. Can J Public Health 109, 395–400 (2018). https://doi.org/10.17269/s41997-018-0067-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/s41997-018-0067-0