
Abstract
Background
The objectives of this study were to determine: (1) the incidence permanent hypothyroidism after thyroid lobectomy (TL), (2) whether asymptomatic patients with mildly elevated thyrotropin (TSH) levels can be managed without thyroid hormone replacement, and (3) if the degree of lymphocytic infiltration (LI) and germinal center (GC) formation in the resected thyroid lobe correlates with the development of post-TL hypothyroidism.
Methods
Subjects undergoing TL between January 2006 and January 2008 at 2 centers were enrolled in the study and thyroid function was followed prospectively based on a previously published algorithm. The histology of each resected thyroid lobe was examined, and the degree of LI and GC was quantified.
Results
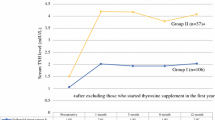
The study cohort consisted of 117 patients. Early postoperative TSH levels were significantly increased over preoperative levels (P < .001). TSH measured at 6 months to 1 year postoperatively, while still significantly increased over preoperative levels (P < .001), was also significantly reduced (P = .006) compared with early postoperative levels. Of the patients who presented with early postoperative hypothyroidism, 69.2% recovered to normal levels without intervention. The overall incidence of early postoperative hypothyroidism was 21.6%, and permanent hypothyroidism was 7.8%. A high degree of LI and GC correlated with a significantly higher mean TSH level (P = .003).
Conclusions
The incidence of hypothyroidism following TL is low, and a significant proportion of individuals who become biochemically hypothyroid will demonstrate only a transient elevation in their TSH levels. As well, individuals with LI, or GC formation, within their resected thyroid lobe may be at increased risk for post-TL hypothyroidism.



Similar content being viewed by others


References
Frates MC, Benson CB, Charboneau JW, Cibas ES, Clark OH, Coleman BG, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;235:794–800.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Lee YH, Lee NJ, Kim JH, Suh SI, Kim TK, Song JJ. Sonographically guided fine needle aspiration of thyroid nodule: discrepancies between cytologic and histopathologic findings. J Clin Ultrasound. 2008;36:6–11.
Mendez W, Rodgers SE, Lew JI, Montano R, Solorzano CC. Role of surgeon-performed ultrasound in predicting malignancy in patients with indeterminate thyroid nodules. Ann Surg Oncol. 2008;15:2487–92.
Wiseman SM, Baliski C, Irvine R, Anderson D, Wilkins G, Filipenko D, et al. Hemithyroidectomy: the optimal surgical approach for individuals undergoing surgery for a cytological diagnosis of follicular neoplasm. Ann Surg Oncol. 2006;13:425–32.
Melck A, Bugis S, Baliski C, Irvine R, Anderson DW, Wilkins G, et al. Hemithyroidectomy: the preferred initial surgical approach for management of Hurthle cell neoplasm. Am J Surg. 2006;191:593–7.
Gharib H, Mazzaferri EL. Thyroxine suppressive therapy in patients with nodular thyroid disease. Ann Intern Med. 1998;128:386–94.
Biondi B, Filletti S, Schlumberger M. Thyroid-hormone therapy and thyroid cancer: a reassessment. Nat Clin Pract Endocrinol Metab. 2005;1:32–40.
Moon HG, Jung EJ, Park ST, Jung TS, Jeong CY, Ju YT, et al. Thyrotropin level and thyroid volume for prediction of hypothyroidism following hemithyroidectomy in an Asian patient cohort. World J Surg. 2008;32:2503–8.
Su SY, Grodski S, Serpell JW. Hypothyroidism following hemithyroidectomy. Ann Surg. 2009;250:991–4.
Wormald R, Sheahan P, Rowley S, Rizkalla H, Toner M, Timon C. Hemithyroidectomy for benign thyroid disease: who needs follow up for hypothyroidism? Clin Otolaryngol. 2008;33:587–91.
Koh YW, Lee SW, Choi EC, Lee JD, Mok JO, Kim HK, et al. Prediction of hypothyroidism after hemithyroidectomy: a biochemical and pathological analysis. Eur Arch Otorhinolaryngol. 2008;265:453–7.
Miller FR, Paulson D, Prihoda TJ, Otto RA. Risk factors for the development of hypothyroidism after hemithyroidectomy. Arch Otolaryngol Head Neck Surg. 2006;132:36–8.
Seiberling KA, Dutra JC, Bajaramovic S. Hypothyroidism following hemithyroidectomy for benign nontoxic thyroid disease. Ear Nose Throat J. 2007;86:295–9.
Piper HG, Bugis SP, Wilkins GE, Walker BA, Wiseman S, Baliski CR. Detecting and defining hypothyroidism after hemithyroidectomy. Am J Surg. 2005;189:587–91.
Berglund J, Bondeson L, Christensen SB, Tibblin S. The influence of different degrees of chronic lymphocytic thyroiditis on thyroid function after surgery for benign, non-toxic goitre. Eur J Surg. 1991;157:257–60.
Cheung P, Boey J, Wong J. Thyroid function after hemithyroidectomy for benign nodules. World J Surg. 1986;10:718–23.
Faber J, Galloe AM. Changes in bone mass during prolonged subclinical hyperthyroidism due to L-thyroxine treatment: a meta-analysis. Eur J Endocrinol. 1994;130:350–6.
Schlote B, Nowotny B, Schaaf L. Subclinical hyperthyroidism: physical and mental state of patients. Eur Arch Psychiatry Clin Neurosci. 1992;241:357–64.
Al-Abadi AC. Subclinical thyrotoxicosis. Postgrad Med J. 2001;77:29–32.
Burmeister LA, Flores A. Subclinical thyrotoxicosis and the heart. Thyroid. 2002;12:495–9.
Sinard RJ, Tobin EJ, Mazzaferri EL, Hodgson SE, Young DC, Kunz AL, et al. Hypothyroidism after treatment nonthyroid head and neck cancer. Arch Otolaryngol Head Neck Surg. 2000;126:652–7.
McHenry CR, Slusarczyk SJ. Hypothyroidism following hemi-thyroidectomy: Incidence, risk factors and management. Surgery. 2000;128:994–8.
Buchanan MA, Lee D. Thyroid auto-antibodies, lymphocytic infiltration and the development of postoperative hypothyroidism following hemithyroidectomy for non-toxic nodular goiter. J R Coll Surg Edinb. 2001;46:86–90.
Stoll SJ, Pitt SC, Liu J, Schaefer S, Sippel RS, Chen H. Thyroid hormone replacement after thyroid lobectomy. Surgery. 2009;146:554–8.
Lombardi G, Panze N, Lupoli, Leonello D, Carlino M, Minozzi M. Study of the pituitary-thyroid axis in euthyroid goiter after partial thyroidectomy. J Endrocrinol Investig. 1983;6:485–7.
Campion L, Gallour G, Ruelland, Cloarec L, Allannic H. Lipid and thyroid changes after partial thyroidectomy: Guidelines for L-thyroxine therapy? Clin Chem. 1995;41:473–4.
Clark OH, Lambert WR, Cavalieri RR, Rapoport B, Hammond ME, Ingbar SH. Compensatory thyroid hypertrophy after hemithyroidectomy in rats. Endrocrinology. 1976;99:988.
Marine D. Control of compensatory hyperplasia of the thyroid of guinea-pigs by administration of iodine. Arch Pathol. 1926;2:829.
Acknowledgment
Dr. Wiseman is a Michael Smith Foundation for Health Research (MSFHR) Scholar, and his work was supported by the MSFHR. Dr. Griffith was supported by the MSFHR and the Canadian Institutes of Health Research (CIHR).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Johner, A., Griffith, O.L., Walker, B. et al. Detection and Management of Hypothyroidism Following Thyroid Lobectomy: Evaluation of a Clinical Algorithm. Ann Surg Oncol 18, 2548–2554 (2011). https://doi.org/10.1245/s10434-011-1627-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-011-1627-1