
Abstract
Background
Pressure injuries (PIs), especially in the sacral region are frequent, costly, and increase morbidity and mortality of patients in an intensive care unit (ICU). These injuries can occur as a result of prolonged pressure and/or shear forces. Neuromuscular electrical stimulation (NMES) can increase muscle mass and improve local circulation, potentially reducing the incidence of PI.
Methods
We performed a randomized controlled trial to assess the efficacy and safety of NMES in preventing PI in critically ill patients. We included patients with a period of less than 48 h in the ICU, aged ≥ 18 years. Participants were randomly selected (1:1 ratio) to receive NMES and usual care (NMES group) or only usual care (control group—CG) until discharge, death, or onset of a PI. To assess the effectiveness of NMES, we calculated the relative risk (RR) and number needed to treat (NNT). We assessed the muscle thickness of the gluteus maximus by ultrasonography. To assess safety, we analyzed the effects of NMES on vital signs and checked for the presence of skin burns in the stimulated areas. Clinical outcomes were assessed by time on mechanical ventilation, ICU mortality rate, and length of stay in the ICU.
Results
We enrolled 149 participants, 76 in the NMES group. PIs were present in 26 (35.6%) patients in the CG and 4 (5.3%) in the NMES group (p ˂ 0.001). The NMES group had an RR = 0.15 (95% CI 0.05–0.40) to develop a PI, NNT = 3.3 (95% CI 2.3–5.9). Moreover, the NMES group presented a shorter length of stay in the ICU: Δ = − 1.8 ± 1.2 days, p = 0.04. There was no significant difference in gluteus maximus thickness between groups (CG: Δ = − 0.37 ± 1.2 cm vs. NMES group: Δ = 0 ± 0.98 cm, p = 0.33). NMES did not promote deleterious changes in vital signs and we did not detect skin burns.
Conclusions
NMES is an effective and safe therapy for the prevention of PI in critically ill patients and may reduce length of stay in the ICU.
Trial registration RBR-8nt9m4. Registered prospectively on July 20th, 2018, https://ensaiosclinicos.gov.br/rg/RBR-8nt9m4
Similar content being viewed by others


Background
Critically ill patients are at a high risk of developing a pressure injury (PI) [1, 2]. PIs can occur as a result of intense and/or prolonged pressure combined with shear forces [3]. Critically ill patients often require mechanical ventilation (MV), during which the head should be kept elevated at 30°, in addition to sedation to ensure patient–ventilator synchrony [4, 5]. Many patients present multiple comorbidities, and may require vasopressor drugs to maintain hemodynamic stability, as well as remaining immobile for long periods. All these factors contribute to the increased incidence of PIs in the sacral region [6].
The incidence of PIs in the ICU ranges from 17.2% to 41.0% depending on the type of patient and their risk factors [7,8,9]. The onset of a PI usually occurs between the first and second week of hospitalization in the ICU and the sacral region is the most affected [2]. The development of PIs is associated with episodes of infection, increased length of hospital stay, and morbidity and mortality [6]. The presence of a PI delays rehabilitation, increases treatment costs, and negatively impacts the quality of life of patients [6, 10].
Due to the high costs associated with the treatment of PIs, some public health systems no longer reimburse the excess costs of stage 3 and 4 PIs acquired during hospitalization [11]. The United Kingdom reports spending of up to £2.1 billion annually on hospital-acquired pressure injury [12]. The high incidence of PIs has proven to be a challenge in ICUs, and this has led to a relentless search for new technologies for their prevention and treatment [10, 13, 14]. Systematic reviews have concluded that the use of support surfaces and the repositioning care frequently employed in clinical practice are not effective in preventing PIs [15, 16].
In this sense, neuromuscular electrical stimulation (NMES) appears to be a potential tool to decrease the incidence of PIs [14]. Through NMES, it is possible to evoke muscle contractions, which can increase local circulation, reduce edema, and maintain muscle mass, without requiring the collaboration of patients [17, 18]. There is evidence that NMES can reduce the incidence of PIs in patients with spinal cord injury [19, 20]. NMES can provide an increase in muscle mass and regional blood flow, as well as an improvement in oxygenation of stimulated tissues in this population [19, 20]. In critically ill patients, the application of NMES is increasingly employed to maintain muscle mass and improve systemic and peripheral circulation [21,22,23].
Thus, it is plausible to advocate that the use of NMES can reduce the incidence of PIs in critically ill patients, but this hypothesis needs to be tested. Therefore, the primary objective of the present study was to assess the effectiveness of NMES in preventing sacral PI in patients admitted to the ICU. Secondarily, we evaluated the effects of NMES on gluteal muscle thickness and clinical outcomes, as well as the feasibility and safety of this therapy.
Methods
Study design
This is a single-center, blinded, two-arm, parallel-group, randomized-controlled trial conducted in two ICUs of a 428-bed public tertiary hospital located in Porto Alegre, Rio Grande do Sul, Brazil. The trial was registered in the Brazilian Registry of Clinical Trials (protocol number RBR-8nt9m4). The study was carried out after approval from the PUCRS Research Ethics Committee No CAEE 91988318.6.0000.5336 and in accordance with CONSORT guidelines [24].
Settings and participants
The study was performed between July 1, 2019 and March 16, 2020, in two general ICUs composed of 29 beds, serving clinical and surgical patients. Patients were randomly assigned in a 1:1 ratio to receive NMES and usual care (NMES group), or usual care only (control group—CG).
Eligibility criteria
Patients aged 18 years or over, admitted to the ICU for less than 48 h, without the presence of a PI in the sacral region, and who agreed to participate, were included in the study. Awake and lucid patients were informed about the study and then received the Informed Consent Form to sign. Consent to participate for sedated and intubated patients was given by the guardians after receiving information and signing the consent form.
Patients were ineligible in case of pregnancy, pacemaker or defibrillator implant, preexisting neuromuscular disease (Duchenne disease, Myasthenia Gravis, Guillain-Barré syndrome), brain death, spinal cord injury, BMI greater than or equal to 35 km/m2, rhabdomyolysis, skin lesion at the site of electrode application, or a medical contraindication.
Randomization and allocation
This was a randomized 2 group parallel clinical trial with an intervention allocation of 1:1. The randomization sequence was generated by a researcher (MBW) who had no participation in patient recruitment. The computer-generated randomization list was prepared using the website www.randomizer.org, which sequentially assigned patients to the CG or NMES group. One researcher (MVB) prepared sealed, opaque, and numbered envelopes containing the group allocation. When each patient was enrolled in the study, the investigator opened the envelope with the smallest number to define the group.
Blinding
Image assessments (ultrasound and photographs of the sacral region) were performed by independent evaluators who were blinded to group allocation. Codes were assigned to the images and patient identification information was removed. It was not possible to blind the patients and the ICU care team.
Control group—CG
The CG received the usual PI prevention care adopted in the routine of the ICUs [25]. These precautions include regular manual repositioning (change of position every 2 h), and the use of pressure relief support surfaces, such as pillows, mattress covers, replacement mattresses, or entire bed replacements. The skin in the sacral region of the pelvis was evaluated daily.
Intervention group—(NMES group)
In addition to the conventional PI prevention care, patients in the NMES group underwent an NMES protocol. NMES was applied in the gluteus maximus region using the Dualpex 071 device (Quark Medical, Piracicaba, Brazil). The area was cleaned with soap and water to remove residues that could hinder electrode adhesion. NMES was used bilaterally with a channel in each muscle. Self-adhesive electrodes measuring 9 × 5 cm were used. The first electrode was attached just below the lateral iliac border and the second at the medial and superior insertion of the gluteus in the iliotibial tract bilaterally, as previously described by Silva et al. [26]. Further details can be seen in Fig. 1. The protocol lasted 25 min, once a day, six times a week, totaling 50 stimuli per session. A symmetric biphasic rectangular pulse was employed, with a frequency of 100 Hz, pulse width of 500 µs, Ton 5 s, Toff 25 s, ramp up of 1 s and ramp down of 1 s. The current amplitude was applied at the greatest possible intensity to evoke maximum contractions (type 5/5) in each gluteus, according to the classification by Segers et al. [27]. During the execution of the protocol, awake patients were able to guide the intensity of stimulation. In less sedated patients, facial expression was important to judge the increase in current intensity. At the end of each session, the electrodes were removed and the underlying skin assessed. The electrode fixation site was marked with a semi-permanent dermographic pen to avoid electrode placement changes in the following days.

Positioning of electrodes in the application of NMES. The figure shows the placement of the 9 × 5 cm self-adhesive electrodes, applied bilaterally with a channel in each gluteus maximus muscle. The first electrode was attached just below the lateral iliac border and the second at the medial and superior insertion of the gluteus in the iliotibial tract, bilaterally, as described by Silva et al. [26]
Outcomes
Primary outcome
Incidence of PI
The primary outcome was the assessment of the incidence of PIs. The groups were evaluated daily for the appearance of PIs in the sacral region, and at any sign of appearance, skin images were captured using a high-resolution smartphone camera (Xiaomi® Mi 9T, 1080 × 2340 px Dual camera, Langfang, Hebei, China). The images were evaluated by three experts who were blinded to the study. The Kappa coefficient of the three evaluators was calculated. Image classification was performed according to the staging system of the latest guidelines published by the European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP), and Pan Pacific Pressure Injury Alliance (PPPIA) [3]. Further details can be seen in Fig. 2.

Diagnosis according to stages of PI. The figure shows the diagnosis of the stages of PI, adapted according to the staging system of the European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP), and Pan Pacific Pressure Injury Alliance (PPPIA) [3]. The stages of PIs are as follows: stage 1 pressure injury, stage 2 pressure injury, stage 3 pressure injury, stage 4 pressure injury, deep tissue pressure injury and unstageable pressure injury
Secondary outcomes
Thickness of the gluteus maximus muscle
The thickness of the right gluteus maximus muscle was assessed by means of ultrasonography (US) images taken in the first 48 h of hospitalization, and every 7 days successively until discharge, death, or the appearance of a PI. For this, the patients were positioned with a 90° hip flexion, and the gluteus maximus thickness was measured at 50% of the distance between the sacral vertebra and the greater trochanter [28]. Further details are shown in Fig. 3. The image acquisition region was defined with a measuring tape and marked with a semi-permanent dermographic pen for further image capture at the same point. The US was performed with the SonoSite EDGE II device (FUJIFILM SonoSite, Bothell, Washington, USA). A linear transducer (7 to 13 MHz), mode B, with a depth of 4.9 cm was used and three images were captured at each recording.

Ultrasound image acquisition of the gluteus maximus muscle. The figure shows the capture site of the ultrasound images of the gluteus maximus muscle thickness. The patient was positioned with a 90° hip flexion. The region was measured at 50% of the distance between the sacral vertebra and the greater trochanter, as described by Barbalho et al. [28]
Safety criteria
Vital signs (mean arterial pressure (MAP), heart and respiratory rates (HR; RR), as well as peripheral oxygen saturation (SPO2)) were assessed before and after each session in the NMES group. In the CG, vital signs were measured before and after a similar time interval (30 min). The skin was evaluated for the presence of burns after NMES.
Feasibility
To assess the feasibility of this protocol, we recorded the time taken to perform the entire procedure (electrode placement, NMES session, and electrode removal). In addition, we counted the total number of prescribed NMES sessions, the total number of sessions performed, and the quality of evoked contractions, according to the classifications of Segers et al. [27]: types 1 to 5 (1: no palpable or visible contraction; 2: just palpable but no visible contraction; 3: just palpable and just visible contraction; 4: palpable and visible contraction (partial muscle bulk); 5: palpable and visible contraction (full muscle bulk).
Clinical outcomes
To analyze clinical outcomes, we assessed time on mechanical ventilation, ICU mortality rate, and length of stay in the ICU.
Sample size calculation
The sample size calculation was performed based on institutional incidence data in the ICU in the previous year. The Power and Sample Size Calculation 3.1 program was used. To detect a 20% difference in the incidence of PI in the NMES group and 40% in the CG, with a significance level of α = 5%, 1-β test power = 80%, and relative risk = 0.5 between groups, 81 patients were calculated as necessary in each group. Taking into account the 15% loss to the follow-up rate, the final number of participants needed in our study was estimated as 100 participants in each group.
Statistical analysis
The numbers of patients per group were provided based on the intention-to-treat principle and the reasons for loss to follow-up were highlighted. To verify the symmetry of data distribution, the Kolmogorov Smirnov test was used. Continuous variables are described using means, standard deviation, median and interquartile range. Categorical variables are presented as absolute values and percentages. To verify the effectiveness of the intervention, the relative risk (RR), relative risk reduction (RRR), absolute risk reduction (ARR), and number needed to treat (NNT) and prevent the event were used. Confidence intervals for these measures of association were obtained and statistical significance was assessed using the Fisher's exact test. Due to the occurrence of the SARS-CoV-2 pandemic, an interim analysis was performed. To evaluate the results of this analysis, the Haybittle–Peto approach was used (p < 0.001), regarding the establishment of the stopping boundary for the interruption of the study [28]. Fisher 1-β post hoc power was also calculated to demonstrate the power of the study for the primary outcome. To verify the agreement of examiners in the assessment of photographic images, the Kappa coefficient was calculated. To verify the agreement in the assessment of muscle thickness in the US images, the intraclass correlation coefficient (ICC) was used. The comparisons of muscle thickness between groups and intragroups were calculated using the Student's t test and Wilcoxon test. In the follow-up characteristics, the comparisons between groups were calculated using the Pearson's Chi-square test, Fisher's exact test, Student's t test for independent groups (assuming homogeneity of variances), and Mann–Whitney test, according to each distribution of data and characteristics. Intergroup analysis of vital signs before and immediately after the session was performed using the Student's t test. A significance level of α < 0.05 was adopted in the statistical tests, with lower results being considered statistically significant. Study data were collected and managed using research electronic data capture (REDCap) tools hosted at PUCRS. Subsequently, the data were exported to Excel and the Statistical Package for Social Science (SPSS), version 25.0 for Windows for analysis.
Results
Study population
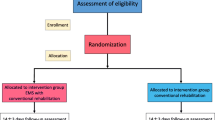
During the study period, 510 patients were evaluated for selection, and of these, 149 were randomized. We were obliged to stop recruitment in March 2020, due to the global spread of SARS-CoV-2, before reaching 81 participants in each group. Thus, the study ended with 73 patients included in the CG and 76 in the NMES group. Therefore, we performed the calculation of Power (1-β) post hoc for the primary outcome. Further details can be seen in the flow diagram in Fig. 4. Tables 1 and 2 present the baseline characteristics and the tracking characteristics of the groups, respectively.

Flow diagram. Other reasons: death before randomization, inter-hospital transfers, not being able to sign the consent form within 48 h, and discharge before screening
Primary outcome
Pressure injury incidence
The development of a PI was present in 26 (35.6%) patients from the CG and 4 (5.3%) from the NMES (p ˂ 0.001) (Fig. 5). Fisher's post hoc power (1-β) was also calculated from the effect size, and a value of 94% was detected for the effect of NMES on the incidence of a PI. The weighted Kappa coefficient of examiner A vs. B was 0.81; A vs. C = 1.00; and B vs. C = 0.81, all these estimates were statistically significant (p < 0.001).

Effect of NMES on pressure injury incidence. NMES: neuromuscular electrical stimulation; RR: relative risk; CI: confidence interval; RRR: relative risk reduction; ARR: absolute risk reduction; NNT: number needed to treat. This effect was analyzed by the Fisher's exact test. An intention-to-treat analysis was performed for all randomized participants
Secondary outcomes
Gluteus maximus thickness
The assessment of gluteus maximus muscle thickness (test–retest) over a period of 7 days was performed in only 34 patients (CG = 17 and NMES Group = 17). This was due to discharges, deaths, and PI incidence during this period. The two-point US images, in the first 48 h of hospitalization and on the seventh day, were analyzed by an expert. The ICC was 0.98 (p < 0.001). There was no significant difference in muscle thickness between groups (CG: Δ = − 0.37 ± 1.2 cm vs. NMES Group: Δ = 0 ± 0.98, p = 0.33). Further details are shown in Fig. 6.

Comparison of intragroups and intergroups gluteus maximum muscle thickness. Only 17 patients remained in the ICU for at least 7 days. NMES: neuromuscular electrical stimulation. p values were calculated by the Student's t test
Safety
No clinically important intergroup variations were observed (Fig. 7). In addition, no skin burns were evidenced.

Effect of NMES on vital signs. The figure shows the variation in vital signs before and immediately after NMES in the intervention and control groups. The variation in the control group was recorded before and after an interval of 30 min (time similar to NMES group). There were no clinically significant intergroup differences in the vital signs. However, a significant numeric intergroup difference was observed in SPO2 on day 2, p < 0.001. All analyses were performed using the Student's t test for independent groups. NMES: neuromuscular electrical stimulation; MAP: mean arterial pressure; SPO2: peripheral oxygen saturation
Feasibility
Two hundred and eighty-two (96%) from the total of 295 prescribed NMES sessions were completed. Thirteen sessions were not carried out in five patients in the NMES group (four patients due to severe hemodynamic instability and one due to surgical intervention), which made it impossible for these patients to be mobilized at some moments. Muscle contraction and viability data are shown in Table 3. At the end of each NMES session, all patients presented fatigue, with decreased quality of contraction.
Clinical outcomes
Patients in the NMES group presented a shorter length of stay in the ICU (Δ = − 1.8 ± 1.2 days, p = 0.04). No significant statistical differences were detected for time on MV and ICU mortality rate. Further details are presented in Table 2.
Discussion
In the present study, we demonstrated that NMES applied in the gluteal region was effective in preventing sacral PI in critically ill patients. This may reduce the length of stay in the ICU. Furthermore, our results reinforce the safety and feasibility of this treatment in the ICU. Despite the aforementioned results, we did not evidence effects of NMES on muscle trophism.
Pressure injury
The incidence of PIs found in the CG of the present study is similar to the values presented by other authors [1, 2]. This high incidence indicates the lack of effectiveness of the current PI prevention strategies recommended in the guidelines, demonstrating the need to study new tools, such as NMES [3, 25].
We did not find an RCT on the use of NMES to prevent PIs in critically ill patients, only one prospective observational study published by Kane et al. [14]. The authors used a continuous NMES protocol with application times ranging from 7 to 24 h, with stimuli of 10 s every 10 min [14]. Twenty patients at moderate to severe risk of developing PI were evaluated and in a follow-up period ranging from 4 to 25 days, none of the patients developed PI.
In the present study, it was not possible to utilize a continuous use protocol, since we performed NMES with a conventional device that does not allow this type of adjustment. It is possible that our favorable results may be related to the characteristics of the current used that could evoke type 4 and 5 contractions. It is a fact that, even when NMES is applied for shorter periods, as in the present study, the anti-inflammatory and local circulatory effects can be perpetuated for hours [22, 23, 29,30,31]. Future studies should establish the optimal dosage of NMES.
Despite the lack of RCTs in critically ill patients, dozens of studies have been published in recent years on the use of NMES to prevent PI in patients with spinal cord injury. This was previously presented in a systematic review [18].
Liu et al. [17] reported that studies used wide variations in current parameters (i.e., frequencies of 10–50 Hz; pulse width of 64–600 µs; and current amplitude of 20–150 mA), which makes analysis difficult. However, four of the five studies that evaluated the long-term effects of NMES (> 8 weeks) demonstrated a reduction in the incidence of PI, corroborating our study.
This reduction appears to be basically associated with three mechanisms, (i) decrease in tissue pressure caused by the change in contact produced by evoked contractions [19, 20]; (ii) local increase in microcirculation [32, 33]; and (iii) muscle hypertrophy [18]. Furthermore, similarly to resistance exercise, NMES can promote anti-inflammatory and angiogenic effects, which may reduce the incidence of PI [29,30,31]. Since we did not demonstrate an increase in the muscle thickness of the gluteus maximus, we attributed the lower incidence of PI in the NMES group to a reduction in pressure areas and to an increase in tissue oxygenation in the adjacent areas.
Gluteus maximus thickness
The fact that there was no increase in muscle mass in the NMES group can be explained by some factors intrinsic to the dose–effect [34]. The treatment time required for NMES to produce muscle hypertrophy in critically ill patients could be longer than 7 days [34,35,36]. Furthermore, the effect on strength gain and trophism is directly proportional to the strength of the evoked contraction [37]. Therefore, an adequate combination of adjustments in frequency, pulse width, and current intensity is necessary [38], as well as in the number of stimuli applied in the area [39]. The choice to use this protocol was based on previous studies in critically ill patients [26, 27] and we agree that higher stimulus intensities could evoke better responses in trophism. Although the majority of our evoked contractions were classified as type 5, we cannot attest that this was the maximal evoked contraction. We used an NMES device developed for outpatient use which could have limited capacity for critically ill patients [40]. In these patients, the use of higher current amplitude and longer pulse width may be essential to achieve better results [26, 27].
Safety and feasibility
The use of NMES in critically ill patients is safe and feasible and is in agreement with previous publications [26, 32, 33, 41]. NMES applied to the glutes of our patients did not cause deleterious changes in the physiological parameters evaluated. In addition, we did not observe any burn cases. When NMES is applied by a trained team and the protocols use adequate electrodes, respecting the current density, the risks are significantly reduced.
The present protocol proved to be feasible, mainly because of its short duration and the fact that it did not impede the ICU care routine, corroborating the findings of Kane et al. [14]. Those authors demonstrated that NMES was simple to use, quick to install and remove (average of 8 min), and could easily be incorporated into routine care. In addition, the costs of acquiring the electrostimulator are considered low, and can be managed by the ICU physiotherapy team. We demonstrated that only 5% of the sessions were canceled for clinical or operational reasons, similar to values presented by other authors [26, 34]. However, this did not make it impossible to apply the NMES on the other days of follow-up.
Clinical outcomes
In the current study, patients in the NMES group presented a shorter length of stay in the ICU compared to the CG. This result may have occurred due to the preventive effect of NMES on PIs. Patients who develop a PI tend to stay in the ICU for longer, which impacts morbidity and costs [6]. Actual costs were not within the scope of this study. However, shortening the ICU length of stay can benefit patients and reduce costs, as longer hospital stays are associated with nosocomial infection, death, delirium, and long-term cognitive impairment [42, 43].
The effect of NMES on the clinical outcomes need be interpreted with caution, since it was not our primary outcome. This was a secondary analysis and does not reflect the main research question for which the sample size was calculated. However, these results could lead to the formulation of new hypotheses that give rise to further data collection and experiments.
Limitations
The present study had some limitations that should be considered. It is a single center study, thus the results may not be generalizable to different patients and care settings. Furthermore, we did not follow up on patients after discharge from the ICU. Moreover, although the examiner was blinded to the groups, we did not have a sham group and the ICU healthcare professionals could not be completely blinded to patient allocation, which are limitations. In this sense, in future procedural improvement studies, a cluster RCT design can be used, where the randomization unit is the center, service, or hospital, and not the individual. Furthermore, it was necessary to interrupt our study before reaching the calculated number of patients for each group. However, the interim analysis with the Haybittle–Peto adjustment showed that the results for the primary outcome were significant and the power post hoc analysis demonstrated a type II error < 20%.
Future perspectives
Future RCTs should focus on the use of stimulators that can deliver wider pulse widths and current intensities in a larger number of muscle groups. This may be key to evoking systemic effects and better outcomes in preventing PIs. In addition, other areas with a high incidence of PIs also need to be evaluated.
Conclusions
The present study demonstrated the safety, feasibility, and efficacy of NMES to reduce the incidence of sacral PIs in critically ill patients. This may reduce the length of stay in the ICU. However, NMES was not able to significantly reduce the loss of muscle mass. The current results may support the incorporation of NMES into the routine of PI prevention in the ICU.
Availability of data and materials
The study data will be available from the corresponding author upon reasonable request.
Abbreviations
- PI:
-
Pressure injury
- ICU:
-
Intensive care unit
- NMES:
-
Neuromuscular electrical stimulation
- CG:
-
Control group
- RR:
-
Relative risk
- RRR:
-
Relative risk reduction
- ARR:
-
Absolute risk reduction
- NNT:
-
Number needed to treat
- SpO2 :
-
Peripheral oxygen saturation
- RBR:
-
Brazilian registry of clinical trials
- MV:
-
Mechanical ventilation
- PUCRS:
-
Pontifical Catholic University of Rio Grande do Sul
- CAEE:
-
Certificate of presentation of ethical appreciation
- CONSORT:
-
Consolidated standards of reporting trials
- BMI:
-
Body mass index
- EPUAP:
-
European pressure ulcer advisory panel
- NPIAP:
-
National pressure injury advisory panel
- PPPIA:
-
Pan pacific pressure injury alliance
- US:
-
Ultrasound
- MAP:
-
Mean arterial pressure
- HR:
-
Heart rate
- RR:
-
Respiratory rate
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- ICC:
-
Intraclass correlation coefficient
- SPSS:
-
Statistical package for social science
- SAPS 3:
-
Simplified acute physiology score 3
- SOFA:
-
Sequential organ failure assessment
- RASS:
-
Richmond agitation sedation scale
- IMS:
-
Intensive care unit mobility scale
- CI:
-
Confidence interval
- NA:
-
Not applicable
- RCT:
-
Randomized controlled trial
References
Pittman J, Beeson T, Dillon J, Yang Z, Mravec M, Malloy C, et al. Hospital-acquired pressure injuries and acute skin failure in critical care: a case-control study. J Wound Ostomy Cont Nurs. 2021;48(1):20–30.
Cox J, Cwocn A. Predictors of pressure ulcers in adult critical care patients. Am J Crit Care. 2011;20(5):364–75.
European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel PPPIA. Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide. Clinical Practice Guideline. 2019. 1–48 p.
Pearson SD, Patel BK. Evolving targets for sedation during mechanical ventilation. Curr Opin Crit Care. 2020;26(1):47–52.
Olkoski E, Assis GM. Application of measures for preventing pressure ulcers by the nursing team before and after an education campaign. Esc Anna Nery - Rev Enferm. 2016;20(2):363–9.
Koerner S, Adams D, Harper SL, Black JM, Langemo DK. Use of thermal imaging to identify deep-tissue pressure injury on admission reduces clinical and financial burdens of hospital-acquired pressure injuries. Adv Ski Wound Care. 2019;32(7):312–20.
Baron MV, Reuter CP, Burgos MS, Cavalli V, Brandenburg C, Krug SBF. Experimental study with nursing staff related to the knowledge about pressure ulcers. Rev Lat Am Enfermagem. 2016;24: e2831.
Jomar RT, de Jesus RP, de Jesus MP, Gouveia BR, Pinto EN, da Pires AS. Incidence of pressure injury in an oncological intensive care unit. Rev Bras Enferm. 2019;72(6):1490–5.
Rogenski NMB, Santos VLC. Incidence of pressure ulcers at a university hospital. Rev Lat Am Enfermagem. 2005;13(4):474–80.
Baron MV, dos Santos AC, Martins PRH, Dominguez LML, Ott JN, Brandenburg C, et al. The combined use of thermography and ultrasound to evaluate the development of pressure injury in a critically ill patient. Med Case Reports Study Protoc. 2021;2(10): e0157.
Fleck CA. Implications of the new centers for medicare & medicaid services pressure ulcer policy in acute care. J Am Col Certif Wound Spec. 2009;1(2):58–64.
Bennett G, Dealey C, Posnett J. The cost of pressure ulcers in the UK. Age Ageing. 2004;33(3):230–5.
Koepp J, Baron MV, Martins PRH, Brandenburg C, Kira ATF, Trindade VD, et al. The quality of mobile apps used for the identification of pressure ulcers in adults: systematic survey and review of apps in app stores. JMIR mHealth uHealth. 2020;8(6):1–15.
Kane A, Warwaruk-Rogers R, Ho C, Chan M, Stein R, Mushahwar VK, et al. A feasibility study of intermittent electrical stimulation to prevent deep tissue injury in the intensive care unit. Adv Wound Care. 2017;6(4):115–24.
Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. J Am Med Assoc. 2006;296(8):974–84.
Gaspar S, Peralta M, Marques A, Budri A, Gaspar de Matos M. Effectiveness on hospital-acquired pressure ulcers prevention: a systematic review. Int Wound J. 2019;16(5):1087–102.
Kaplan HM, Baker LL, Davoodi R, Wong NT, Loeb GE. Preventing ischial pressure ulcers: II. Biomech Appl Bionics Biomech. 2011;8(3–4):333–43.
Liu LQ, Moody J, Traynor M, Dyson S, Gall A. A systematic review of electrical stimulation for pressure ulcer prevention and treatment in people with spinal cord injuries. J Spinal Cord Med. 2014;37(6):703–18.
Kim J, Ho CH, Wang X, Bogie K. The use of sensory electrical stimulation for pressure ulcer prevention. Physiother Theory Pr. 2010;26(8):528–36.
Gyawali S, Solis L, Chong SL, Curtis C, Seres P, Kornelsen I, et al. Intermittent electrical stimulation redistributes pressure and promotes tissue oxygenation in loaded muscles of individuals with spinal cord injury. J Appl Physiol. 2011;110(1):246–55.
Liu M, Luo J, Zhou J, Zhu X. Intervention effect of neuromuscular electrical stimulation on ICU acquired weakness: a meta-analysis. Int J Nurs Sci. 2020;7(2):228–37.
Ojima M, Takegawa R, Hirose T, Ohnishi M, Shiozaki T, Shimazu T. Hemodynamic effects of electrical muscle stimulation in the prophylaxis of deep vein thrombosis for intensive care unit patients: a randomized trial. J Intensive Care. 2017;5(1):9.
Gerovasili V, Tripodaki E, Karatzanos E, Pitsolis T, Markaki V, Zervakis D, et al. Short-term systemic effect of electrical muscle stimulation in critically ill patients. Chest. 2009;136(5):1249–56.
Boutron I, Altman DG, Moher D, Schulz KF, Ravaud P, CONSORT NPT Group. CONSORT statement for randomized trials of nonpharmacologic treatments: a 2017 update and a CONSORT extension for nonpharmacologic trial abstracts. Ann Intern Med. 2017;167(1):40–7.
European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel PPPIA. Prevention and Treatment of Pressure Ulcers : Quick Reference Guide. Clinical Practice Guideline. 2014. 1–75 p.
Silva PE, Babault N, Mazullo JB, Oliveira TP, Lemos BL, Carvalho VO, et al. Safety and feasibility of a neuromuscular electrical stimulation chronaxie-based protocol in critical ill patients: a prospective observational study. J Crit Care. 2017;37:141–8.
Segers J, Hermans G, Bruyninckx F, Meyfroidt G, Langer D, Gosselink R. Feasibility of neuromuscular electrical stimulation in critically ill patients. J Crit Care. 2014;29(6):1082–8.
Barbalho M, Coswig VS, Steele J, Fisher JP, Paoli A, Gentil P. Evidence for an upper threshold for resistance training volume in trained women. Med Sci Sports Exerc. 2019;51(3):515–22.
Sanchis-Gomar F, Lopez-Lopez S, Romero-Morales C, Maffulli N, Lippi G, Pareja-Galeano H. Neuromuscular electrical stimulation: a new therapeutic option for chronic diseases based on contraction-induced myokine secretion. Front Physiol. 2019;10:1463.
Bahadori S, Immins T, Wainwright TW. The effect of calf neuromuscular electrical stimulation and intermittent pneumatic compression on thigh microcirculation. Microvasc Res. 2017;111:37–41.
Filipovic A, Kleinöder H, Plück D, Hollmann W, Bloch W, Grau M. Influence of whole-body electrostimulation on human red blood cell deformability. J Strength Cond Res. 2015;29(9):2570–8.
Stefanou C, Karatzanos E, Mitsiou G, Psarra K, Angelopoulos E, Dimopoulos S, et al. Neuromuscular electrical stimulation acutely mobilizes endothelial progenitor cells in critically ill patients with sepsis. Ann Intensive Care. 2016;6(1):21.
Angelopoulos E, Karatzanos E, Dimopoulos S, Mitsiou G, Stefanou C, Patsaki I, et al. Acute microcirculatory effects of medium frequency versus high frequency neuromuscular electrical stimulation in critically ill patients—a pilot study. Ann Intensive Care. 2013;3(1):39.
Silva PE, De CássiaMarqueti R, Livino-De-Carvalho K, De Araujo AET, Castro J, Da Silva VM, et al. Neuromuscular electrical stimulation in critically ill traumatic brain injury patients attenuates muscle atrophy, neurophysiological disorders, and weakness: a randomized controlled trial. J Intensive Care. 2019;7(1):59.
Gerovasili V, Stefanidis K, Vitzilaios K, Karatzanos E, Politis P, Koroneos A, et al. Electrical muscle stimulation preserves the muscle mass of critically ill patients: a randomized study. Crit Care. 2009;13(5):R161.
Nakano H, Naraba H, Hashimoto H, Mochizuki M, Takahashi Y, Sonoo T, et al. Novel protocol combining physical and nutrition therapies, Intensive Goal-directed REhabilitation with Electrical muscle stimulation and Nutrition (IGREEN) care bundle. Crit Care. 2021;25(1):415.
Maffiuletti NA, Gondin J, Place N, Stevens-Lapsley J, Vivodtzev I, Minetto MA. Clinical use of neuromuscular electrical stimulation for neuromuscular rehabilitation: what are we overlooking? Arch Phys Med Rehabil. 2018;99(4):806–12.
Gregory CM, Dixon W, Bickel CS. Impact of varying pulse frequency and duration on muscle torque production and fatigue. Muscle Nerve. 2007;35(4):504–9.
Dow DE, Cederna PS, Hassett CA, Kostrominova TY, Faulkner JA, Dennis RG. Number of contractions to maintain mass and force of a denervated rat muscle. Muscle Nerve. 2004;30(1):77–86.
Grunow JJ, Goll M, Carbon NM, Liebl ME, Weber-Carstens S, Wollersheim T. Differential contractile response of critically ill patients to neuromuscular electrical stimulation. Crit Care. 2019;23:308.
Sachetti A, Carpes MF, Dias AS, Sbruzzi G. Safety of neuromuscular electrical stimulation among critically ill patients: systematic review. Rev Bras Ter Intensiva. 2018;30(2):219–25.
Cai Y, Lo JJM, Venkatachalam I, Kwa AL, Tambyah PA, Hsu LY, et al. The impact of healthcare associated infections on mortality and length of stay in Singapore—a time-varying analysis. Infect Control Hosp Epidemiol. 2020;41(11):1315–20.
Stollings JL, Kotfis K, Chanques G, Pun BT, Pandharipande PP, Ely EW. Delirium in critical illness: clinical manifestations, outcomes, and management. Intensive Care Med. 2021;47(10):1089–103.
Acknowledgements
CAPES, as well as the FAPERGS.
Funding
This study was funded in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brazil (CAPES)—Finance Code 001, as well as by the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS) (contest FAPERGS 05/2019—Programa Pesquisador Gaúcho—PQG). CAPES and FAPERGS had no role in the design or conduct of the study, collection, analysis, or interpretation of data, in the writing of the manuscript or in the decision to submit it for publication. The corresponding authors had full access to all data and the ultimate responsibility for submitting them for publication.
Author information
Authors and Affiliations
Contributions
MVB and BEPC had full access to all the study data and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: MVB, BEPC, and PES. Acquisition of data: MVB, AFMS, and MPS. Analysis and interpretation of data: MVB, BEPC, MVMP, SC, and PES. Drafting of the manuscript: MVB, BEPC, CEPF, JSU, JK, and PES. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: MBW. Obtained funding: BEPC. Administrative, technical, or material support: CB, TM, ICR BEPC. Study supervision: MVB. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Research Ethics Committee of PUCRS under CAEE No. 91988318.6.0000.5336. All legally acceptable participants or representatives provided informed consent.
Consent for publication
Not applicable.
Competing interests
Dr. Paulo Eugênio Silva has patents in neuromuscular electrical stimulation as an inventor. He also has equity in Visuri SA and serves as a scientific advisor. The remaining authors have no relevant conflicts to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Baron, M.V., Silva, P.E., Koepp, J. et al. Efficacy and safety of neuromuscular electrical stimulation in the prevention of pressure injuries in critically ill patients: a randomized controlled trial. Ann. Intensive Care 12, 53 (2022). https://doi.org/10.1186/s13613-022-01029-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-022-01029-1