
Abstract
Background
Interventions aimed at reducing risky sexual behavior are considered an important strategy for averting Human Immunodeficiency Virus (HIV) infection among youth (15–24 years) who continue to be at risk of the disease. Enhancing intervention success requires a comprehensive understanding of the barriers and facilitators to interventions targeting youth. However, there is lack of a systematic review of both quantitative and qualitative studies to comprehensively identify and synthesize barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth worldwide. This review aimed to identify and synthesize barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth globally based on original peer-reviewed studies published in the last decade.
Methods
The Joanna Briggs Institute approach for mixed methods systematic reviews and Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines were used to guide this review. Nine electronic databases, Joint United Nations Programme on HIV/AIDS and World Health Organization websites, and reference lists of included studies and systematic reviews on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth were searched for eligible articles. Studies that met the inclusion criteria underwent quality appraisal and data extraction. Findings were analyzed using thematic synthesis and underpinned by Nilsen, 2015’s Determinant Framework.
Results
Overall 13 studies comprising of eight qualitative studies, four quantitative studies and one mixed methods study were included in the review. Several barriers and facilitators across the five Determinant Framework domains were identified. Most of the barriers fell under the characteristics of the context domain (e.g., gender-biased norms). The next important group of barriers emerged within the characteristics of the end users domain (e.g., fear of relationship breakdown). In terms of facilitators, the majority fell under the characteristics of the strategy of facilitating implementation domain (e.g., implementation of intervention with fidelity) and characteristics of the end users domain (e.g., fear of pregnancy or sexually transmitted infections). The next common set of facilitators appeared within the characteristics of the context domain (e.g., family support).
Conclusion
This review identified several multi-level barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth. Multi-level and combination approaches are needed to address these factors and enhance intervention success.
Similar content being viewed by others


Background
Young people continue to be at considerable risk for Human Immunodeficiency Virus (HIV) despite intervention efforts to control the disease [1]. Specifically, youth aged between 15 and 24 years account for nearly 30% of all new HIV infections and 9% of all people living with HIV worldwide [2]. Moreover, there are indications that HIV infection rates among youth will increase annually by 13% leading to approximately 3.5 million new infections by 2030 [2, 3]. The socio-ecological model [4, 5] suggests that young people are vulnerable to HIV due to numerous factors at different socio-ecological levels that affect risky sexual behaviors including low self-esteem, lack of parent–child communication, peer pressure, poverty [6, 7], alcohol or drug abuse [8], limited HIV-related knowledge, gender-based violence [9], gender disparities and cultural factors [10, 11].
To date HIV has no cure, therefore HIV prevention programs aimed at reducing risky sexual behavior are regarded as an important strategy of controlling the disease. As a result, various HIV prevention interventions for reducing risky sexual behavior among youth have been developed [12, 13]. Reviews that have evaluated the efficacy of these interventions suggest that such strategies are more effective at changing non-behavioral outcomes (e.g., attitudes, beliefs, intentions and HIV-related knowledge), and less effective at changing behavioral outcomes (e.g., condom use) [14,15,16].
Developing effective strategies to enhance intervention efficacy requires a comprehensive understanding of the barriers and facilitators to HIV prevention interventions targeting youth. Theoretical framework is valuable for identifying barriers and facilitators to intervention and for developing policies and strategies to promote intervention success [17, 18]. One such theoretical framework is the Determinant Framework proposed by Nilsen, 2015 [17]. This framework is composed of five major domains or levels, which can capture a myriad of factors that affect the success of an intervention. These domains include: (i) characteristics of the implementation object, which involves features of an intervention that might influence intervention success (e.g., duration of the intervention); (ii) characteristics of the users or adopters, which includes features of implementers of an intervention that might influence intervention success (e.g., training, skills and experience of the implementers of an intervention); (iii) characteristics of the end users, which includes attributes of clients or recipients of an intervention that might affect intervention success (e.g., age, knowledge and self-efficacy of the recipients of an intervention); (iv) characteristics of the context, which involves attributes of conditions or surroundings of an intervention that might affect intervention success (e.g., availability of funding or resources within the organization implementing the intervention); and (v) characteristics of the strategy of facilitating implementation, which includes tactics of delivering a program that might influence intervention success (e.g., implementation of intervention with fidelity or according to plan) [17].
In the last decade, a number of systematic reviews have been conducted on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior in youth [19,20,21,22,23,24,25]. However, these reviews have synthesized research findings from studies that were conducted using quantitative approaches [19,20,21,22,23,24,25]. Furthemore, these reviews have focused on studies conducted in a specific geographical region; for instance, Sub-Saharan Africa [22,23,24], developing countries [20], Europe [21], and South Africa [19, 25]. Other reviews have focused on barriers [22] or facilitators [20] only. Moreover, in the last decade, no systematic review has included both quantitative and qualitative studies to identity and synthesize barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth worldwide. Therefore, the purpose of this review was to synthesize current global evidence on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth based on peer-reviewed quantitative, qualitative or mixed methods studies published in the last decade. Conducting this review was essential to provide holistic evidence to support youth-focused HIV prevention programs across the globe. Consistent with other reviews, barriers were defined as factors that impede intervention success (e.g., lack of funding) [23]. Facilitators were defined as factors that promote intervention success (e.g., availability of funding) [23].
Methods
Study design
This systematic review was conducted using the Joanna Briggs Institute (JBI) approach for mixed methods systematic reviews [26] and Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [27]. The mixed methods approach was employed to obtain a comprehensive synthesis of evidence than that provided by a single method approach [28]. The protocol for this review was registered in PROSPERO (registration number CRD42020187272) [29].
Inclusion criteria
Studies were considered in this review if they:
-
(a)
were original peer-reviewed studies written in English language;
-
(b)
included youth (15–24 years) as intervention recipients;
-
(c)
presented barriers and/or facilitators to HIV prevention intervention for reducing risky sexual behavior;
-
(d)
were conducted in any geographical location;
-
(e)
were conducted using quantitative, qualitative or mixed methods study designs;
-
(f)
were published between January 2010 and April 2022. This period was chosen to obtain current evidence.
Search strategy
The Cambridge Core, CINAHL, Cochrane Library, Google Scholar, MEDLINE, ProQuest Central, PsycINFO, Oxford Journals and Web of Science datababes, Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organization (WHO) websites were searched for eligible studies using relevant keywords. Moreover, reference lists of included studies and systematic reviews on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth were screened to identify additional eligible studies. Keywords used to search included “Youth”, “Barriers”, “Facilitators”, “HIV Prevention Intervention”, “Risky Sexual Behavior”, “Efficacy” and “Implementation” (Additional file 1: Table S1). Booleans (e.g., “OR” and “AND”) were used to combine similar and different search terms, respectively. For example, (youth OR young people OR teen OR young adults OR students OR adolescents) AND (barriers OR challenges OR constrains OR difficulties OR obstacles OR issues OR problems). A detailed search strategy is shown in Additional file 1: Table S1 using MEDLINE as a example. The search strategy was adapted to other databases/websites.
Study selection
Following the search, all identified references were collated and uploaded into EndNote X9 Reference Management System and duplicates removed. FM, EA and ATB assessed the title, abstract and full-text articles against the inclusion criteria. Any disagreements were resolved through consensus.
Assessment of methodological quality
The methodological quality of the studies were assessed independently by FM, EA and ATB, and differences were resolved through discussion. Authors of papers were contacted to request missing information. Quantitative studies were assessed using the JBI Critical Appraisal Checklist for Randomized Controlled Trials (13 items) [26] and JBI Critical Appraisal Checklist for Quasi-Experimental Studies (nine items) [26]. The JBI Critical Appraisal Checklist for Qualitative Research (10 items) [26] was used to assess qualitative studies. Mixed methods studies were appraised using both methods. A study was considered ‘good’ if it scored more than 70%, ‘fair’ if it scored between 50 and 70% and ‘poor’ (excluded) if it scored less than 50% on the quality appraisal tool.
Data extraction
FM extracted data from the included studies using a standardized JBI data extraction form [26]. Data extraction was discussed with EA, MTB and AB, and any discrepancies were resolved though consensus. Details extracted include: author, year of publication, title of the study, purpose or objective of the study, study location, setting, study design, population and sample size, methods, data analysis and findings (barriers and facilitators). Findings regarding barriers and facilitators were identified through repeated reading of the studies. Additional file 2: Table S2–S14 presents extracted findings relating to barriers and facilitators with each finding supported by an illustration from the same text that informed the finding. As recommended by JBI, quantitative data were converted into ‘qualitized data’ (textual descriptions or narrative interpretation of the quantitative findings) to enhance integration with qualitative data.
Data synthesis
Synthesis involved two phases. In the first phase, a thematic synthesis approach was used [30, 31]. This involved reading of the findings several times for familiarization, systematic coding of data and identification of prominent themes. In the second phase, barriers and facilitators obtained from thematic synthesis were mapped to the Determinant Framework suggested by Nilsen, 2015 [17] to highlight the key barriers and facilitators, and strategies needed within the different Determinant Framework levels to improve intervention success [17, 18]. Synthesis was undertaken by FM, and discussed with EA, MTB and AB. Any disagreements were resolved through consensus.
Results
Search outcome
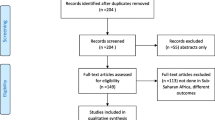
Of the 7826 records identified, 6691 titles and abstracts were screened. Of these, 144 full-texts were further screened and 13 studies met the inclusion criteria. No studies were excluded following assessment of methodological quality (Fig. 1).
Characteristics of the included studies
The characteristics of the included studies are summarized in Table 1. Studies included in the review consisted of eight qualititative studies [32, 36,37,38,39, 42,43,44], four quantitative studies [34, 35, 40, 41] and one mixed methods study [33]. Of the quantitative studies, two studies were quasi-experimental studies without a comparison group [34, 35], one study was a quasi-experimental study with a comparison group [40], and one study was a randomised controlled trial [41].
Of the included studies, six were published in 2012 [34, 38, 41,42,43,44]. Seven studies were published each in 2010 [36], 2011 [32], 2013 [37], 2016 [35], 2017 [33], 2019 [40] and 2020 [39].
Seven countries were represented across the included studies including the United States of America [34, 35, 37, 40,41,42], Tanzania [43, 44], Yemen [32], Myanmar [33], South Africa [36], Uganda [38] and Mozambique [39]. As per the World Bank definition [45], majority of these countries (n = 6) were low/middle-income countries, except the United States of America (a high-income country). Four of the low/middle-income countries were from Sub-Saharan Africa, a region with the highest number of people living with HIV than any other region in the world [2].
In terms of setting, seven studies were conducted in a community setting [32, 34,35,36,37, 39, 43], two studies were undertaken in an educational setting [38, 40], two studies were conducted in a healthcare setting [41, 42], one study was undertaken in community and healthcare setting [33], and one study was conducted in the community, educational and healthcare setting [44].
Participants were youth or intervention recipients in eight studies [34,35,36,37,38, 41,42,43]. One study included youth and implementers [33], one study involved youth, implementers and community members [32], one study included youth, family members and community members [39], one study incorporated youth and community members [44]. One study involved implementers but was included because the intervention recipients were youth [40]. The number of participants within the included studies ranged from 20 to 343. Rorhbach, 2019 [40] did not report the number of implementers (trained program staff). The age of youth participants ranged from 15–24 years in eight studies [33,34,35,36,37, 39, 41, 42]. Three studies did not mention the age of youth participants [32, 38, 44]. One study reported the age of youth participants as ranging from 24 to 29 years for males and 24–30 years for females but was included because participants were aged 15–24 years when the intervention was implemented [43].
Overall, the quality of the included studies was good with nine studies [32, 34, 35, 39,40,41,42,43,44] scoring more than 70% on the quality appraisal tool. Four studies [33, 36,37,38] were rated as fair (scored between 50 and 70% on the quality appraisal tool) [Additional file 1: Table S2–S4].
Barriers and facilitators
Thematic synthesis [30, 31] and mapping of the study findings to the Determinant Framework [17] highlighted a wide range of barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth. A summary of the identified barriers and facilitators across the five Determinant Framework domains is presented in Table 2.
Barriers to HIV prevention interventions for reducing risky sexual behavior among youth
A total of 81 barriers to HIV prevention interventions for reducing risky sexual behavior among youth were identified from the included studies: 42 in the characteristics of the context, 23 in the characteristics of the end users, seven in the characteristics of the implementation object, five in the characteristics of the strategy of facilitating implementation and four in the characteristics of the users domains.
Characteristics of the context
Barriers within the characteristics of the context domain were reported by 10 studies [32,33,34, 36,37,38,39, 42,43,44]. Four types of barriers emerged: interpersonal, community, organizational or institutional and structural barriers. The most common interpersonal barriers identified involve those linked to the reduction of risky sexual behavior among youth, such as partner’s refusal to use an HIV prevention method (e.g., condom use) [32, 33, 38, 39, 42], lack of financial support from family [38, 39, 43], controlling partner [42, 43], peer pressure [38, 43, 44] and lack of child-parent communication on sexual issues [36, 38]. Community barriers that occurred more prominently involve those associated with the reduction of risky sexual behavior among youth. These include gender-biased norms [36, 38, 39, 43, 44], norms discouraging discussion of sexual issues between parents and children [32, 44] and limited resources or services in the community (e.g., programs targeting young people) [32, 33]. Another common set of community barriers identified consists of those associated with young people’s participation in the intervention, such as community violence [34]. Organizational barriers identified involve those linked to the reduction of risky sexual behavior among youth. These include lack of resources (e.g., condoms), inaccessibility of services (e.g., healthcare facilities) and poor quality of services (e.g., lack of confidentiality) [44]. Other organizational barriers reported comprise of those associated with the participation of youth in the intervention. This includes inaccessibility of intervention venue [34, 37]. The most common set of structural barriers reported involve those correlated with the reduction of risky behavior among young people, such as economic constrains [32, 43], gender-based violence [39], unemployment [32] and limited economic opportunities [44].
‘“Safer sex would be safe of course…but at times we can fail to agree on it [condom use]. Eeh… he gives you all sorts of excuses; he is not interested….”’ [38]
‘For the rare young people who may have considered using condoms, access was limited, especially for girls, with intermittent supplies, distant health facilities, and limited confidentiality’ [44]
Characteristics of the end users
Seven studies [32, 33, 38, 41,42,43,44] identified barriers at the level of characteristics of the end users. Barriers that appeared more prominently include those associated with the reduction of risky sexual behavior among youth. Such barriers include low perceptions of the risk of sexually transmitted infections including HIV [33, 38, 42,43,44], fear of relationship breakdown [33, 38, 42, 43], being stubborn or hardheaded and desire for pregnancy or children [42, 43]. Another common set of barriers consists of those related to young people’s participation in the intervention, such as concern for privacy [32, 44] and fear of stigma [44].
Characteristics of the implementation object
Six studies [32,33,34,35, 43, 44] mentioned barriers within the domain of the characteristics of the implementation object. The most common set of barriers identified involves those associated with intervention acceptability among young people. Such barriers include incompatibility of intervention content with the needs of youth [33, 43], long duration of the intervention [33, 35] and complexity of the intervention [35]. Similarly, incompatibility of the intervention content with the needs of community members was mentioned as a barrier to intervention acceptability among community members [44]. Additionally, barriers reported concern those linked to youth’s participation in the intervention, such as restricted days and times of the intervention [34] and age requirements that excluded other youth [33]. Additional barriers that emerged include those associated with the reduction of risky sexual behavior among young people. This includes limited intervention content (e.g., intervention content addresses individual factors such as knowledge without addressing structural factors such as poverty and unemployment) [32, 44].
‘One criticism of the MkV [MEMA kwa Vijana] sessions from some male participants was that they were not linked closely enough to the long-term aspirations of the students.’ [43]
‘…one CBO [community-based organization] staff noted that the upper age limitation of the Link Up project (up to 24 years) likely resulted in lower uptake of services of YMSM [young men who have sex with men] who were partners of MSM [men who have sex with men].’ [33]
‘“….The majority unchanged because education is not enough; they are also in need for other programmes addressing poverty, unemployment and to occupy their spare time.”’ [32]
Characteristics of the strategy of facilitating implementation
Two studies [32, 44] mentioned barriers within the characteristics of the strategy of facilitating implementation domain. The category of barriers identified involves those associated with intervention acceptability among youth. This includes the use of non-participatory facilitating methods [32]. Additional barriers to HIV prevention programs for youth reported within this domain include failure to implement the intervention with fidelity, use of corporal punishment and sexual abuse [44].
‘“At the beginning I liked it [program], but later I found it somewhat boring because they continued advising and advising all the time!”’ [32]
Characteristics of the users
At the level of characteristics of the users, barriers were reported by two studies [37, 44]. Barriers reported comprise of those linked to intervention acceptability among young people. This includes adult or older implementers [37]. Other barriers to program success identified at this level include implementers’ lack of knowledge related to the content of the intervention, poor education or training of implementers and implementers’ lack of exemplary or positive behavior [44].
‘A few expressed concerns that some facilitators being older might not be able to understand
their experiences.’ [37]
Facilitators to HIV prevention interventions for reducing risky sexual behavior among youth
There were 46 facilitators to HIV prevention interventions for reducing risky sexual behavior among youth identified from the included studies: 15 in the characteristics of the strategy of facilitating implementation, 13 in the characteristics of the end users, 12 in the characteristics of the context, four in the characteristics of the users and two in the characteristics of the implementation object domains.
Characteristics of the strategy of facilitating implementation
Facilitators within this domain were mentioned by six studies [32, 35,36,37, 40, 44]. Identified facilitators include those linked to intervention acceptability among youth, such as use of same-sex youth group [36, 37], implementation of intervention with fidelity [37] and use of different or mixed facilitating methods [35]. Further facilitators reported involve those correlated with young people’s participation in the intervention, such as provision of incentives, building of a trusting relationship, mobilization of community members to influence youth to attend the intervention, integration of intervention with other services and use of same-age or peer implementers [32]. Other facilitators within this domain include dissemination of intervention information to community members [32, 36, 37], use of participatory facilitating methods, decreased corporal punishment [44] and collaboration among different stakeholders in delivering the intervention [32].
Characteristics of the end users
Facilitators within the characteristics of the end users domain were reported by seven studies [32, 36, 37, 39, 42,43,44]. Facilitators that emerged more prominently consist of those related to the reduction of risky sexual behavior among youth. Such facilitators include fear of pregnancy or sexually transmitted infections including HIV [32, 37, 43], having strong ambitions or being future-oriented [39, 44], having good problem-solving skills, having high self-confidence, being knowledgeable [42], having high self-motivation [39] and low socio-economic status (e.g., lack of money to pay for sex) [44]. Another group of facilitators identified comprises of those associated with young people’s participation in the intervention. This includes perceived benefits of the intervention [37].
‘“…He asked why I wanted him to use a condom and I pretended I was tired of giving birth but in reality, I feared AIDS [acquired immunodeficiency syndrome] as well as pregnancy.”’ [43]
‘One girl explained that the money was not as important as the knowledge she had acquired, and others discussed enjoyment from attending and participating in activities.’ [37]
Characteristics of the context
Six studies [33, 38, 39, 42,43,44] identified facilitators at the characteristics of the context level. Three classifications of facilitators occurred: interpersonal, community and organizational facilitators. The most common interpersonal facilitators reported involve those associated with the reduction of risky sexual behavior among youth. These include partner’s consent to use an HIV prevention method (e.g., condom use) [42, 43], restrictive parenting [38, 44], family support [39, 44], positive peer influence [38] and teacher advice [38]. Similarly, community facilitators that emerged more prominently comprise of those linked to the reduction of risky sexual behavior among young people. Such facilitators include norms encouraging healthy sexual practices (e.g., abstinence and delaying of sexual debut) [44] and religious beliefs discouraging risky sexual behavior [38]. Organizational facilitators reported involve those associated with intervention acceptability among youth. This includes accessibility and friendliness of intervention venue [33].
‘Four girls with reduced risk described receiving significant support from their households specifically to continue with their education.’ [39]
‘“…I can [abstain] because…it also goes against my Christian values to engage in sex before marriage….”’ [38]
‘“…the drop-in-center is a great space, near to the clinic, friendly, freely and wonderful place…”’ [33]
Characteristics of the users
Four studies [32, 33, 37, 44] reported facilitators at the characteristics of the users level. Identified facilitators involve those linked to intervention acceptability among youth, such as approachability or friendliness of implementers [33, 37] and experience of implementers [37]. Additional facilitators include training of implementers [32] and implementers’ knowledge of intervention content [44].
‘“…If we are interested in blood test [HIV test], peer educators accompanied us to the clinic, that’s the point I like most…feeling like we are not alone…’” [33]
Characteristics of the implementation object
Facilitators within the characteristics of the implementation object domain were identified by four studies [32, 35,36,37]. Two groups of facilitators emerged: those associated with intervention acceptability among youth and those associated with intervention acceptability among implementers. Compatibility of intervention content with the needs of youth [35,36,37] was mentioned as a facilitator to intervention acceptability among youth. Relative advantage of the intervention was reported as a facilitator to intervention acceptability among implementers [32].
Comparison of the identified barriers and facilitators between low\middle- and high-income countries, and male and female youth
There were similarities and differences in identified barriers and facilitators between low/middle- and high-income countries. A major difference noted is that most of the reported barriers within the characteristics of the context domain (mainly community, organizational and structural barriers) affect mostly low/middle-income countries than high-income countries (Additional file 3: Table S1). Also, similarities and differences were observed in reported barriers and facilitators between male and female youth. An important difference observed is that most of the identified barriers and facilitators within the characteristics of the end users and characteristics of the context domains (barriers and facilitators associated with the reduction of risky sexual behavior among youth) affect mostly female youth than male youth. (Additional file 3: Table S2).
Discussion
This review identified and synthesized barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth (15–24 years) worldwide based on quantitative, qualitative and mixed methods studies published in the last decade. Overall, the findings indicate that barriers and facilitators of HIV prevention intervention for reducing risky sexual behavior among youth comprise of factors associated with the intervention, implementers of the intervention, recipients of the intervention, context of the intervention and strategy of implementing the intervention. Additionally, the most barriers to interventions targeting young people involve factors associated with the context of the intervention and recipients of the intervention. Most facilitators include factors associated with the strategy of implementing the intervention and recipients of the intervention. Other important facilitators consist of factors linked to the context of the intervention.
Similarities exist between this review’s findings when comparing with existing literature. For example, Michielsen et al. 2010 [22] also reported barriers associated with the intervention (e.g., limited intervention content). Barriers linked to the implementers of the intervention (e.g., adult implementers) were also identified in other reviews [21, 25]. Additionally, barriers related to the context of the intervention (e.g., limited resources) were also found in previous reviews [19, 22]. The findings of this review concur with other reviews [22, 23] that identified barriers related to the strategy of delivering the intervention (e.g., failure to implement the intervention with fidelity). Furthermore, this review’s findings are consistent with other reviews [14, 16] that found facilitators associated with the implementers of the intervention (e.g., knowledge and experience of implementers). Other reviews [20, 23, 24] also identified facilitators correlated with the strategy of implementing the intervention (e.g., implementation of intervention with fidelity). Another review [46] also mentioned attributes of recipients of the intervention as factors determining the success of interventions targeting young people.
This review’s findings, however, differ from previous reviews in that the present review found numerous barriers linked to the recipients of the intervention (e.g., fear of relationship breakdown, lack of self-confidence, poor decision-making skills) that were not reported in previous reviews [16, 19,20,21,22,23,24,25]. Furthermore, whilst other reviews [16] identified few facilitators associated with the recipients of the intervention (e.g., gender, age and race), the current review found additional facilitators associated with the recipients of the intervention (e.g., fear of pregnancy or sexually transmitted infections, having high self-confidence and having good problem skills). Moreover, previous reviews [16] identified few facilitators related to the context of the intervention, mainly organizational factors (e.g., supportive implementation climate), the present review identified additional facilitators associated with the context of the intervention, mainly interpersonal factors (e.g., positive peer influence, parental advice, family support), community factors (e.g., norms encouraging healthy sexual behaviors and religious beliefs discouraging risky sexual behavior) and organizational factors (e.g., accessibility and friendliness of intervention venue). Additionally, the current review reported additional barriers associated with the strategy of implementing the intervention (e.g., use of non-participatory facilitating methods, use of corporal punishment and sexual abuse) and additional facilitators associated with the strategy of implementing the intervention (e.g., use of participatory facilitating methods, decreased corporal punishment, use of same-age implementers and provision of incentives) not reported in previous reviews [16, 19,20,21,22,23,24,25]. Moreover, the present review identified further facilitators linked to the intervention (e.g., compatibility of the intervention with the needs of youth and relative advantage of the intervention) which were not reported in previous reviews [16, 20, 23,24,25]. The discordance in findings with other reviews may be due to the inclusion of qualitative evidence and the use of a theoretical framework for analysis, which may have contributed to a more holistic findings.
Several limitations should be considered when interpreting the findings of this review. Few included studies (n = 13) in this review could affect the generalizability of the findings. Another limitation is the lack of eligible studies from different high-income countries; all the identified studies (n = 6) from a high-income setting were conducted in the United States of America, and therefore, not representative of all high-income contexts. Additionally, this review was limited to only original peer-reviewed studies; written in English language; and published between January 2010 and April 2022, which may result in publication bias. Also, as some of the included studies did not report the age of youth participants, the review might have included youth not aged 15–24 years. Furthermore, majority of the studies included in this review collected data through self-reports, which may have compromised the quality of the evidence as self-reports are prone to both over-and under-reporting [47]. Whitehead, 2016 [48] argue that the approach to data collection is highly likely to influence the nature and quality of data. Another reason for concern is that determinant frameworks such as the one used to synthesize the factors in this review do not examine causal relationships between the barriers or facilitators and outcomes [17], it is, therefore, difficult to determine with greater certainty whether or not the identified factors influence intervention success.
The review, on the other hand, had its strengths. To the authors’ knowledge, this is the first systematic review incorporating different types of studies to synthesize existing global evidence on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth. The use of a mixed methods approach most likely results in a more comprehensive understanding of the topic under study [28]. Moreover, the review provides a recent summary of literature from 2010 to 2022. Another strength of this review is the use of a theoretical framework to synthesize the factors. This may have helped to highlight key barriers and facilitators, identify gaps in the literature and formulate theory-driven strategies to facilitate improvements. To the authors’ knowledge, this is the first review to undertake a study of this nature using a theory. Using theory to examine barriers and facilitators adds to the growing body of evidence for the utility of theory to synthesize the factors. Additional strength is that other important population groups in HIV prevention interventions for young people such as implementers, community and family members were represented in this review which may have helped to provide more evidence. Futhermore, most of the included studies (n = 9) were of good quality, and four studies were of fair quality. Therefore, the review findings can reliably inform policies and programmatic strategies to promote the success of HIV prevention interventions for youth.
This systematic review has important implications for practice, policy and research. Considering that the findings of this review suggest that several multi-level barriers and facilitators influence interventions targeting youth, there is need for multi-level approaches to address these factors and enhance intervention success. Multi-level interventions consider barriers and facilitators at multiple levels, evaluate the inter-relationships between these factors, and formulate strategies to enhance intervention success [49]. Evidence suggests that multi-level approaches contribute to the success of an intervention [50]. Furthermore, to promote intervention success, the findings of this review imply the need for combination approaches. Research has established that interventions incorporating different prevention strategies are associated with positive outcomes [46, 51, 52].
Furthermore, the findings of the current review suggest that most barriers to interventions targeting youth include factors associated with the context of the intervention and recipients of the intervention. To enhance intervention success, there is need for more intervention efforts to be directed towards removing barriers associated with context of the intervention and recipients of the intervention. Approaches that have been found successful to address barriers linked to context of the intervention include peer education interventions [53], family-based interventions [54], school-based interventions, community-based interventions, health facility-based interventions [55] and structural interventions [56]. Behavioral or individual risk reduction interventions that use behavior change techniques (e.g., condom-use, communication and motivation enhancement, psycho-education and assertiveness skills training) have been found effective to remove barriers associated with recipients of the intervention [16, 57].
In this review, factors associated with the strategy of implementing the intervention were identified as barriers and facilitators to HIV prevention interventions targeting youth. These findings imply the need for intervention implementers to be sensitive to the delivery strategies they use as some implementation methods are counterproductive. Also, there is need for intervention implementers to ensure that interventions are implemented with fidelity or as intended to enhance intervention success. Evidence suggests that implementation of intervention with fidelity promotes intervention success [23, 24].
Other barriers and facilitators to interventions targeting youth found in the present review include factors associated with the intervention. As guided by Sekhon, 2017’s [58] theoretical framework of intervention acceptability, these findings highlight the importance for intervention designers to develop interventions that are compatible with the needs and values of the target population to enhance program success. To identify the needs of the target population and incorporate them into the intervention, it is recommended that preliminary formative research be conducted as it is linked to intervention success [16].
In this review, factors associated with the implementers of the intervention were some of the reported barriers and facilitators to interventions for young people. These results suggest the need to recruit implementers with desirable characteristics, train them, and provide monitoring, support and supervision to promote intervention success. Research has demonstrated that the use of implementers with attractive attributes (e.g., same-age or peer implementers) promotes intervention success [16, 21].
Findings of this review suggest that barriers and facilitators to HIV prevention programs for reducing risky sexual behavior among youth differ by region (low/middle- and high-income countries) and gender of intervention recipients. These results imply the need for intervention strategies that address the specific barriers and facilitators by region and gender of intervention recipients.
Given the small number of studies identified in the current review, further studies of this nature are recommended. As determinant frameworks do not examine causal relationships between barriers or facilitators and outcomes [17], it is recommended that further experimental studies be conducted to identify and determine the most effective, feasible and acceptable strategies to enhance intervention efficacy. Also, it is recommended that future studies utilize theoretical frameworks to highlight the most important factors that influence interventions targeting youth and formulate theory-driven strategies to promote intervention success.
Conclusion
This systematic review synthesized current global evidence on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth. The review shows that barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth include factors associated with the intervention, implementers of the intervention, recipients of the intervention, context of the intervention and strategy of implementing the intervention. Furthermore, the review suggests that most barriers to interventions targeting young people comprise of factors associated with the context of the intervention and recipients of the intervention. Most facilitators involve factors linked to the strategy of implementing the intervention and recipients of the intervention. Other important facilitators include factors associated with the context of the intervention. The findings of this review highlight the need for multi-level and combination approaches to remove barriers and facilitate intervention success. Furthermore, the review suggests the need for further research on barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among young people.

PRISMA flow diagram illustrating selection of studies
Availability of data and materials
Data that support the findings of this study are included in this article and its additional files.
Change history
11 October 2022
A Correction to this paper has been published: https://doi.org/10.1186/s12879-022-07762-z
Abbreviations
- AIDS:
-
Acquired Immunodeficiency Syndrome
- CBO:
-
Community-based organization
- FSW:
-
Female sex worker
- HIV:
-
Human Immunodeficiency Virus
- JBI:
-
Joanna Briggs Institute
- KIU:
-
Keep It up
- MkV:
-
MEMA kwa Vijana
- MSM:
-
Men who have sex with men
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-analysis
- UNAIDS:
-
Joint United Nations Programme on HIV/AIDS
- WHO:
-
World Health Organization
- YR:
-
Yemen rial
- YMSM:
-
Young men who have sex with men
References
World Health Organization. Why the HIV epidemic is not over. 2020. https://www.who.int/news-room/spotlight/why-the-hiv-epidemic-is-not-over. Accessed 9 Oct 2020.
Joint United Nations Programme on HIV/AIDS. AIDSinfo: Global data on HIV epidemiology and response. 2021. http://aidsinfo.unaids.org/. Accessed 21 Sept 2021.
United Nations Children’s Fund. Children and AIDS: Statistical Update. 2017. https://www.childrenandaids.org/sites/default/files/2017-11/Children%20%26%20AIDS%20-%20Statistical%20Update.pdf2017. Accessed 13 Oct 2021.
Centers for Disease Control and Prevention. The Social Ecological Model: A Framework for Prevention. 2014. http://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html. Accessed 15 May 2020.
Kaufman MR, Cornish F, Zimmerman RS, Johnson BT. Health behavior change models for HIV prevention and AIDS care: practical recommendations for a multi-level approach. J Acquir Immune Defic Syndr. 2014;66(Suppl 3):S250.
DiClemente RJ, Crittenden CP, Rose E, et al. Psychosocial predictors of HIV-associated sexual behaviors and the efficacy of prevention interventions in adolescents at-risk for HIV infection: what works and what doesn’t work? Psychosom Med. 2008;70(5):598–605.
Eaton L, Flisher AJ, Aarø LE. Unsafe sexual behaviour in South African youth. Soc Sci Med. 2003;56(1):149–65.
Govender K, Cowden RG, Asante KO, George G, Reardon C. Sexual risk behavior: a multi-system model of risk and protective factors in South African adolescents. Prev Sci. 2019;20(7):1054–65.
Harper GW, Riplinger AJ, Neubauer LC, Murphy AG, Velcoff J, Bangi AK. Ecological factors influencing HIV sexual risk and resilience among young people in rural Kenya: Implications for prevention. Health Educ Res. 2014;29(1):131–46.
Dancy BL, Jere DL, Kachingwe SI, Kaponda CP, Norr JL, Norr KF. HIV risk reduction intervention for rural adolescents in Malawi. J HIV AIDS Soc Serv. 2014;13(3):271–91.
Van Staden A, Badenhorst G. Reviewing gender and cultural factors associated with HIV/AIDS among university students in the South African context. Curationis. 2009;32(4):19–28.
Hosek S, Pettifor A. HIV prevention interventions for adolescents. Curr HIV/AIDS Rep. 2019;16(1):120–8.
Muthoni CN, Kneipp SM, Gichane MW, Caiola CE, Pettifor AE, Williams JR. A systematic review of HIV interventions for young women in sub-Saharan Africa. AIDS Behav. 2020;24:3395–413.
Johnson BT, Scott-Sheldon LJ, Huedo-Medina TB, Carey MP. Interventions to reduce sexual risk for human immunodeficiency virus in adolescents: a meta-analysis of trials, 1985–2008. Arch Pediatr Adolesc Med. 2011;165(1):77–84.
Picot J, Shepherd J, Kavanagh J, et al. Behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19 years: a systematic review. Health Educ Res. 2012;27(3):495–512.
Protogerou C, Johnson BT. Factors underlying the success of behavioral hiv-prevention interventions for adolescents: a meta-review. AIDS Behav. 2014;18:1847–63.
Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53.
Weatherson KA, Gainforth HL, Jung ME. A theoretical analysis of the barriers and facilitators to the implementation of school-based physical activity policies in Canada: a mixed methods scoping review. Implement Sci. 2017;12:41.
Harrison A, Newell ML, Imrie J, Hoddinott G. HIV prevention for South African youth: which interventions work? A systematic review of current evidence. BMC Public Health. 2010;10(1):1–2.
Ibrahim S, Sidani S. Community based HIV prevention intervention in developing countries: a systematic review. Adv Nurs. 2014;2014:174960.
Lazarus JV, Sihvonen-Riemenschneider H, Laukamm-Josten U, Wong F, Liljestrand J. Systematic review of interventions to prevent the spread of sexually transmitted infections, including HIV, among young people in Europe. Croat Med J. 2010;51(1):74–84.
Michielsen K, Chersich MF, Luchters S, De Koker P, Van Rossem R, Temmerman M. Effectiveness of HIV prevention for youth in sub-Saharan Africa: systematic review and meta-analysis of randomized and nonrandomized trials. AIDS. 2010;24(8):1193–202.
Mwale M, Muula AS. Systematic review: a review of adolescent behavior change interventions [BCI] and their effectiveness in HIV and AIDS prevention in sub-Saharan Africa. BMC Public Health. 2017;17(1):1–9.
Sani AS, Abraham C, Denford S, et al. School-based sexual health education interventions to prevent STI/HIV in sub-Saharan Africa: a systematic review and meta-analysis. BMC Public Health. 2016;16(1):1–26.
Scott-Sheldon AJL, Walstrom P, Harrison AC, Kalichman SP, Carey M. Sexual risk reduction interventions for HIV prevention among South African Youth: a meta-analytic review. Curr HIV Res. 2013;11(7):549–58.
Aromataris E, Munn Z, eds. Joanna Briggs Institute Reviewer’s Manual [Internet]. Adelaide: Joanna Briggs Institute, 2017. https://reviewersmanual.joannabriggs.org/. Accessed 26 Apr 2020.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–41.
Teddlie C, Tashakkori A. Foundations of mixed methods research: Integrating quantitative and qualitative approaches in the social and behavioral sciences. Thousand Oaks: Sage; 2009.
Mbengo F, Adama E, Towell-Barnard A, Bhana A. Barriers and facilitators to effectiveness of Human Immunodeficiency Virus (HIV) prevention interventions for reducing risky sexual behaviour in youth (15–24 years): A mixed methods systematic review protocol. PROSPERO 2020 CRD42020187272. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020187272. Accessed 10 Oct 2020.
Hong QN, Pluye P, Bujold M, Wassef M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev. 2017;6(1):61.
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45.
Al-Iryani B, Al-Sakkaf K, Basaleem H, Kok G, van den Borne B. Process evaluation of a three-year community-based peer education intervention for HIV prevention among Yemeni young people. Int Q Community Health Educ. 2011;31(2):133–54.
Aung PP, Ryan C, Bajracharya A, et al. Effectiveness of an integrated community-and clinic-based intervention on HIV testing, HIV knowledge, and sexual risk behavior of young men who have sex with men in Myanmar. J Adolesc Health. 2017;60(2):S45–53.
Garofalo R, Johnson AK, Kuhns LM, Cotton C, Joseph H, Margolis A. Life skills: evaluation of a theory-driven behavioral HIV prevention intervention for young transgender women. J Urban Health. 2012;89(3):419–31.
Greene GJ, Madkins K, Andrews K, Dispenza J, Mustanski B. Implementation and evaluation of the Keep It Up! online HIV prevention intervention in a community-based setting. AIDS Educ Prev. 2016;28(3):231–45.
Jewkes R, Wood K, Duvvury N. ‘I woke up after I joined Stepping Stones’: meanings of an HIV behavioural intervention in rural South African young people’s lives. Health Educ Res. 2010;25(6):1074–84.
Morrison-Beedy D, Passmore D, Carey MP. Exit interviews from adolescent girls who participated in a sexual risk-reduction intervention: implications for community-based health education promotion for adolescents. J Midwifery Womens Health. 2013;58(3):313–20.
Musiimenta A. Contextual mediators influencing the effectiveness of behavioural change interventions: A case of HIV/AIDS prevention behaviours. Online J Public Health Inform. 2012. https://doi.org/10.5210/ojphi.v4i2.3988.
Ridgeway K, Lenzi R, Packer C, et al. ‘I married when I was 16… due to poverty, I had no other way’: multi-level factors influencing HIV-related sexual risk behaviours among adolescent girls in Zambézia. Mozambique Cult Health Sex. 2020. https://doi.org/10.1080/13691058.2020.1715483.
Rohrbach LA, Donatello RA, Moulton BD, Afifi AA, Meyer KI, De Rosa CJ. Effectiveness evaluation of it’s your game: keep it real, a middle school hiv/sexually transmitted infection/pregnancy prevention program. J Adolesc Health. 2019;64(3):382–9.
Sales JM, Brown JL, DiClemente RJ, Rose E. Exploring factors associated with nonchange in condom use behavior following participation in an STI/HIV prevention intervention for African-American adolescent females. AIDS Res Treat. 2012. https://doi.org/10.1155/2012/231417.
Sales JM, DiClemente RJ, Davis TP, Sullivan S. Exploring why young African American women do not change condom-use behavior following participation in an STI/HIV prevention intervention. Health Educ Res. 2012;27(6):1091–101.
Wamoyi J, Mshana G, Doyle AM, Ross DA. Recall, relevance and application of an in-school sexual and reproductive health intervention 7–9 years later: perspectives of rural Tanzanian young people. Health Promot Int. 2012;28(3):311–21.
Wight D, Plummer M, Ross D. The need to promote behaviour change at the cultural level: one factor explaining the limited impact of the MEMA kwaVijana adolescent sexual health intervention in rural Tanzania. A process evaluation BMC Public Health. 2012;12(1):788.
The World Bank. World Bank and Country Lending Groups. Country Classification. 2022. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed 03 Apr 2022.
Ahankari AS, Wray J, Jomeen J, Hayter M. The effectiveness of combined alcohol and sexual risk taking reduction interventions on the sexual behaviour of teenagers and young adults: a systematic review. Public Health. 2019;173:83–96.
Demetriou C, Ozer BU, Essau CA. Self-Report Questionnaires. In: Cautin RL, Lilienfield, SO. (eds). The Encyclopedia of Clinical Psychology. 2015. (pp. 1-6).
Whitehead D, Whitehead L. Sampling data and data collection in qualitative research. In: Schneider Z, Whitehead D. (eds). Nursing and midwifery research: Methods and appraisal for evidence based practice, 5th edn. Chapter 7, pp. 111–123. Australia: Elsevier; 2016.
Lewis CF, Crawford ND. Multi-level interventions/Structural Approaches to HIV Prevention. In: Hope T, Stevenson M, Richman D. (eds). Encyclopedia of AIDS. 2015. (pp. 1-9). Springer, New York.
DiClemente RJ, Patel N. HIV Prevention Among Youth: Designing Effective Evidence-Based HIV Risk-Reduction Programs for Adolescents. In: Chenneville T. (eds). A Clinical Guide to Pediatric HIV. 2016. (pp. 273-295). Springer, Cham.
Thurman TR, Kidman R, Carton TW, Chiroro P. Psychological and behavioral interventions to reduce HIV risk: evidence from a randomized control trial among orphaned and vulnerable adolescents in South Africa. AIDS Care. 2016;28(sup1):8–15.
Firestone R, Rivas J, Lungo S, et al. Effectiveness of a combination prevention strategy for HIV risk reduction with men who have sex with men in Central America: a mid-term evaluation. BMC Public Health. 2014;14(1):1–5.
Mahat G, Scoloveno MA. Effectiveness of adolescent peer education programs on reducing HIV/STI risk: an integrated review. Res Theory Nurs Pract. 2018;32(2):168–98.
Ocasio MA, Lozano A, Lee TK, Feaster DJ, Carrico A, Prado G. Efficacy of a family-based intervention for HIV prevention with hispanic adolescents with same gender sexual behaviors. Prev Sci. 2021;25:1–1.
Mavedzenge SM, Doyle AM, Ross DA. HIV prevention in young people in sub-Saharan Africa: a systematic review. J Adolesc Health. 2011;49(6):568–86.
Baird SJ, Garfein RS, McIntosh CT, Özler B. Effect of a cash transfer programme for schooling on prevalence of HIV and herpes simplex type 2 in Malawi: a cluster randomised trial. The Lancet. 2012;379(9823):1320–9.
Adejumo AO. Influence of psycho-demographic factors and effectiveness of psycho-behavioural interventions on sexual risk behaviour of in-school adolescents in Ibadan City. IFE PsychologIA: An International Journal. 2012;20(1):1–8.
Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):1–3.
Acknowledgements
The authors wish to thank librarian, Lisa Webb for her support with developing the review protocol.
Funding
This research was funded by the Edith Cowan University under a Higher Degree by Research Scholarship awarded to FM. Beyond funding support, the funder had no direct role in the study design, collection, analysis and interpretation of data, or writing the manuscript.
Author information
Authors and Affiliations
Contributions
FM, EA and ATB conceptualized and designed the study, screened and critically appraised the studies. Literature search, data extraction and analysis and writing of the first manuscript draft were done by FM. EA, ATB, AB and MZ critically reviewed the work and provided feedback on the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article has been updated to correct figure 1 and table 1.
Supplementary Information
Additional file 1.
Table S1. Search strategy in MEDLINE. Table S2. Critical appraisal results of included quasi-experimental studies (quantitative studies). Table S3. Critical appraisal results of included randomized controlled trial (quantitative study). Table S4. Critical appraisal results of included qualitative studies and mixed methods study (qualitative component).
Additional file 2.
Additional tables.
Additional file 3. Table S1.
Comparison of the identified barriers and facilitators between low/middle- and high-income countries. Table S2. Comparison of the identified barriers and facilitators between male and female youth
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mbengo, F., Adama, E., Towell-Barnard, A. et al. Barriers and facilitators to HIV prevention interventions for reducing risky sexual behavior among youth worldwide: a systematic review. BMC Infect Dis 22, 679 (2022). https://doi.org/10.1186/s12879-022-07649-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07649-z