
Abstract
Background
Granulomatous amoebic encephalitis (GAE) is a rare central nervous system infection caused by the Balamuthia mandrillaris or Acanthamoeba species. Diagnosis is challenging because of the non-specific clinical presentation, cerebrospinal fluid analysis, and radiological features. There is no effective treatment for GAE to date.
Case presentation
A 54-year-old male was admitted to hospital after experiencing acute onset of numbness and weakness on his left limb. Due to the initial consideration of intracranial tumor, surgical removal of the right parietal lesion was performed. However, the patient had a headache accompanied by diplopia, difficulty walking and a new lesion was found in the left occipital-parietal lobe two weeks after the first operation. High-throughput next-generation sequencing (NGS) detected the presence of high copy reads of the B. mandrillaris genome sequence in the patient’s blood, cerebral spinal fluid (CSF), and brain tissue. Pathological investigation of the brain tissue showed granulomatous changes and amoebic trophozoite scattered around blood vessels under high magnification. The patient was re-operated due to developing progressive confusion caused by subfalcine herniation of the left cerebral hemisphere. The lesions of the right parietal lobe were obviously decreasing in size after the first surgery, and the lesions of the left occipital lobe and the sunfalcine herniation didn’t ameliorate two months after the second surgery. The patient was transferred to local hospital for continuous treatment with sulfamethoxazole and azithromycin. After five months of the second surgery, the patient showed good recovery with mild headache.
Conclusions
This is the first report of a patient with B. mandrillaris encephalitis initially confirmed by NGS and have experienced two excisions, responding favorably to the combination of surgeries and medications. Early surgical resection of intracranial lesions combined with drug treatment may offer the chance of a cure.
Similar content being viewed by others


Background
Granulomatous amoebic encephalitis (GAE) is a rare central nervous system (CNS) infection caused by Balamuthia mandrillaris or Acanthamoeba species; the infection progresses chronically or subacutely, during a period of few weeks to few years. B. mandrillaris is a free-living species of amoebae which was first isolated in 1989 [1]. It exists in water or soil, and infects humans through the skin or respiratory tract. It may also infect humans through organ transplantations by spreading through blood, or through direct invasions in the CNS through the olfactory neuroepithelium [2, 3]. B. mandrillaris encephalitis (BAE) has been predominantly found in South America and the United States. Only few cases have been reported in China. The onset symptom of GAE is insidious and followed by rapid severe neurological decline, including headaches, seizures, altered levels of consciousness, comas, and death. Diagnosis is challenging because of the non-specific clinical presentation, cerebrospinal fluid (CSF) analysis, and radiological features.
Here, we describe a middle-aged male patient from Southern China, who was diagnosed with B. mandrillaris encephalitis confirmed by High-throughput next-generation sequencing (NGS), and survived with two excisions and medications (Additional file 1).
Case presentation
A 54-year-old male experiencing acute onset of numbness and weakness in his left limb was admitted to the First Affiliated Hospital of Guangxi Medical University on Nov. 1, 2020. Initial magnetic resonance imaging (MRI) of the brain showed abnormal signals in the right parietal lobe. Brain computed tomography (CT) (Fig. 1A1) and enhanced MRI (Fig. 2A1) on Nov. 10 showed an ill-defined infiltrating enhanced mass in the right parietal lobe with perilesional edema, which pointed to the possibility of a low-grade glioma. Resection of the mass in the right parietal lobe was performed on Nov. 12. The specimen exhibited granulomatous changes and inflammatory perivascular infiltrate (Fig. 3A) with positive CD68 staining, negative acid-fast, periodic acid-achiff and CD235a staining. The patient consequently received antibiotic therapy: intravenous Linezolid (0.2 g twice daily for 9 days). His left limb weakness improved slightly, as seen in his activity of daily living (ADL) scores. The ADL score was 75 after the surgery in comparison to 70 before the surgery. However, the patient had a headache accompanied by diplopia and difficulty walking when he was taking hyperbaric oxygen therapy on Nov. 28. An emergency head CT on Dec. 2 showed that a new low-density focus occurred in the left occipital lobe (Fig. 1B1). The blood tests on Dec. 5 revealed that erythrocyte sedimentation rate was 31 mm/h (0–15), hypersensitive C-reactive protein was 0.8 mg/L (0-1), immunoglobulin G subtype 4 was 4.04 g/L and antinuclear antibody was weakly positive. The white blood cells, neutrophils, lymphocytes, eosinophils and platelets were in normal range except for a slight decrease of red blood cells and hemoglobin level. The other tests including the vasculitis antibodies, fungal (1-3)-β-D glycan, and galaetomannan test were normal. Brain enhanced MRI on Dec.7 showed a new abnormal signal focus in the left occipital-parietal lobe, and the operation area of the right parietal lobe had more obvious effusion and edema (Fig. 2A2). Lumbar puncture on Dec. 7 revealed high intracranial pressure (330 mmH2O), elevation in white cell count (320*106/L, neutrophils 45%, lymphocytes 55%) and protein (1041 mg/L), as well as a slight decrease in glucose (2.01 mmol/L) and chloride (116.1 mmol/L). No acid fast bacilli, fungi and bacteria were found in the cerebrospinal fluid (CSF) smear and culture. Despite a treatment with intravenous Ceftriaxone Sodium (2 g twice daily for 4 days), the patient still had an obvious headache, diplopia, non-fluent speech and worse muscle strength in his left limbs. Neurological examination on Dec. 10 showed left eyeball adduction, left eyeball abduction, and right eyeball abduction were impaired. Re-examination of lumbar puncture on Dec.11 showed that the CSF data were getting worse (intracranial pressure 330 mmH2O, white cell count 480*106/L with neutrophils 40%, lymphocytes 60% and protein 1422 mg/L, glucose 1.24 mmol/L and chloride 111.5 mmol/L). Intravenous Vancomycin (1.0 g iv drip Q12h) and Meropenem (0.5 g iv drip Q6h) were applied on Dec.11 due to consideration of intracranial infection caused by bacteria. High-throughput next-generation sequencing (Vision Medicals, Guangzhou) detected the presence of Balamuthia mandrillaris with 112 sequence copy reads in serum and 539 sequence copy reads in the CSF (Fig. 4A, B). GAE caused by Balamuthia mandrillaris was thus diagnosed. On Dec.14, the treatment was adjusted to compound treatment with sulfamethoxazole/trimethoprim 0.48 g×2 tablets po. Bid, azithromycin tablets 0.25 g×2 po. Qd, flucytosine 2.5 g iv drip Q12 h, and amphotericin B iv drip Qd (increased gradually with 5–10–15–20–25–30 mg). He did not receive a combination therapy of miltefosine and pentamidine because neither medication was available in China. The patient often went fishing in the past 10 years and worked occasionally in a paddy field. He had no known tick bites or any skin lesions.

The dynamic changes of head CT. A The original lesion in the right parietal lobe was getting smaller; B a new lesion occurring in the left occipital lobe became worse

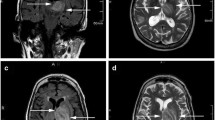
The dynamic changes of brain magnetic resonance imaging (MRI). A1–A4 The lesions of the right parietal lobe were obviously getting smaller on T2-weighted image (T2W2). B1–B3 The lesions of the left occipital lobe and the left cerebral subfalcine herniation became better slightly. Both lesions of the right parietal lobe and the left occipital lobe showed high signal intensity on T2W2, obvious high signal intensity on diffusion-weighted image (DWI) and enhancement on gadolinium-enhanced T1-weighted image (Gd-T1WI) in the left occipital lobe lesions, milder enhancement in the right parietal lobe

Histological examinations. A Granulomatous changes and inflammatory perivascular infiltrate (×100); B Amoea trophozoite (×400)

The results of high-throughput next-generation sequencing (NGS). Balamuthia mandrillaris with 112 sequence copy reads in serum (A), 539 sequence copy reads in CSF (B), and 3723 sequence copy reads in brain tissue (C)
Re-examination of brain MRI on Dec. 23 showed larger lesions on the left cerebral hemisphere with enhancement, causing left subfalcine herniation (Fig. 2B1). The patient was transferred to the department of neurosurgery and was re-operated on Dec. 27. Histological examination of the left occipital lobe confirmed amoebic trophozoite gathering around blood vessels under high magnification (Fig. 3B). The presence of B. mandrillaris with 3723 sequence copy reads was also detected in brain tissue via NGS (Fig. 4C). After surgery, re-examination of brain MRI on Jan. 6, 2021 indicated that the lesion and subfalcine herniation of the left cerebral hemisphere were relieved slightly than before (Fig. 2B2). However, the patient developed progressive confusion. A repeated head CT on Jan. 13 revealed that the left subfalcine herniation became worse (Fig. 1B4) after medication therapy was discontinued for two weeks. A combined medication therapy was restarted with sulfamethoxazole/trimethoprim (0.48 g×2 po. Bid), azithromycin tablets (0.25 g×2 po. Qd), flucytosine (2.5 g iv drip q12h) and fluconazole (0.6 g iv drip Qd). After treatment, the patient felt better than before with a mild headache. ADL scores were 40 before and 45 after the second surgery. An additional head CT on Feb. 22 revealed that the left subfalcine herniation was slightly relieved (Fig. 1B7). The patient was transferred to another local hospital on Feb. 22 for continuous treatment with sulfamethoxazole (po), azithromycin (po) and fluconazole (iv drip).
The patient responded favorably to the first surgery in part as showed in head CT (Fig. 1A1-7) and MRI (Fig. 2A1-4); the lesions of the right parietal lobe were obviously getting smaller. He responded well slightly to the second excision with the left occipital lobe lesions and the subfalcine herniation was getting better in head CT (Fig. 1B1-7) and MRI (Fig. 2B1-3). It is interesting that calcification was seen in the left parietal lobe and basal ganglia after Dec. 18 (Fig. 1B2), as well as the right parietal lobe after Feb. 10 (Fig. 1A6).
At the follow-up by phone, the patient was discharged from the local hospital on April 2, 2021 and showed good recovery with a ADL score of 95, in comparison to past scores of 70 (before the first surgery) and 40 (before the second surgery) as shown in Table 1. At the follow-up by phone on June. 2, 2021, the patient has been taking with sulfamethoxazole (po) and azithromycin (po) and shows slow recovery with a current ADL score of 100 as shown in Table 1.
Discussion and conclusions
To date, over 200 cases of GAE caused by B. mandrillaris have been described worldwide. During 1974–2016, 109 case reports of Balamuthia disease were recorded in the United States. Most (99%) had encephalitis [4]. In China, there have been 28 cases of B. mandrillaris infection during the past 20 years and only 16 cases (57%) developed amoebic encephalitis [5]. Most Balamuthia cases were reported in the western and southern regions of the United States, probably because of the hot and dry environment [4]. Interestingly, this patient has been living in Southern China where it is hot and humid.
The GAE has been described mostly in immunocompromised patients, rarely in an immunocompetent host. Unlike the other amoeba species, B. mandrillaris affects both immunocompromised and immunocompetent people [6]. This patient has been healthy. From the presence of B. mandrillaris in serum, CSF, and brain tissue, he was probably infected with B. mandrillaris through a cutaneous lesion by contacting with the contaminated soil or water.
GAE is always fatal because of delayed diagnosis. In the beginning, this patient was considered to have a brain tumor because of unspecific symptoms and an absence of skin lesions. The progressive neurological decline after the first surgery of this patient raised the attention of neurologists with intracranial infections. Many cases of GAE were diagnosed via autopsy postmortem, sections of the skin, or brain tissue before [4]. However, with the development of NGS for pathogen detection, the diagnosis of GAE is determined in earlier stages of the disease than before. To the best of our knowledge, this is the third case of GAE reported within China via next-generation sequencing [7, 8]. As a rapid and accurate method of pathogen identification, NGS has large potential in the diagnosis of difficult and rare cases. It also has guiding significance for clinicians on deciding the treatment strategy for patients.
The combination drugs of pentamidine, sulfadiazine, flucytosine, fluconazole, azithromycin or clarithromycin, and miltefosine are recommended for treatment of Balamuthia infection in the United States [4]. In China, Lincomycin, azithromycin, interferon-γ, or a combination of these drugs showed effect in treating skin lesions, and one survivor who developed focal encephalitis was treated by excision of the infected brain tissue [5]. The 14 cases with BAE who treated with surgery and medical treatment are summarized in Tables 1, 2 [2, 9,10,11,12,13,14,15,16,17]. Among 14 cases, 4 patients including one child and two of old age (21.4%) responded favorably to the combined therapy with complete recovery. The neurological symptoms of the 3 patients were relatively mild and they were likely to be in the early stage of the disease. The role of surgery in Balamuthia infection is previously applied to diagnostic biopsy. It is now suggested that early surgical resection of intracranial lesions combined with drug therapy may be an important method for the treatment of Balamuthia infection. However, due to the limited number of surgical survivors, prognostic factors and effective treatment options need to be further studied.
In conclusion, this is the first report of an immunocompetent patient with GAE caused by B. mandrillaris survived with two excisions and medications. Early surgical resection of intracranial lesions combined with medication treatment may offer the chance of a cure.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Abbreviations
- GAE :
-
Granulomatous amoebic encephalitis
- NGS :
-
Next-generation sequencing
- CSF :
-
Cerebral spinal fluid
- BAE :
-
B. mandrillaris encephalitis
- MRI :
-
Magnetic resonance imaging
- CT :
-
Computed tomography
- ADL :
-
The activity of daily living
- ESR :
-
Erythrocyte sedimentation rate
- CRP:
-
Hypersensitive C-reactive protein
References
Visvesvara GS, Martinez AJ, Schuster FL, Leitch GJ, Wallace SV, Sawyer T. Leptomyxid ameba, a new agent of amebic meningoencephalitis in humans and animals. J Clin Microbiol. 1990;28(12):2750–6.
Shehab KW, Aboul-Nasr K, Elliott SP. Balamuthia mandrillaris granulomatous amebic encephalitis with renal dissemination in a previously healthy child: case report and review of the pediatric literature. J Pediatric Infect Dis Soc. 2018;7(3):e163-8.
Farnon EC, Kokko KE, Budge PJ, Mbaeyi C, Lutterloh EC, Qvarnstrom Y, da Silva AJ, Shieh WJ, Roy SL, Paddock CD, et al. Transmission of Balamuthia mandrillaris by Organ Transplantation. Clin Infect Dis. 2016;63(7):878–88.
Cope JR, Landa J, Nethercut H, Collier SA, Glaser C, Moser M, Puttagunta R, Yoder JS, Ali IK, Roy SL. The epidemiology and clinical features of balamuthia mandrillaris disease in the United States, 1974-2016. Clin Infect Dis. 2019;68(11):1815–22.
Wang L, Cheng W, Li B, Jian Z, Qi X, Sun D, Gao J, Lu X, Yang Y, Lin K, et al. Balamuthia mandrillaris infection in China: a retrospective report of 28 cases. Emerg Microbes Infect. 2020;9(1):2348–57.
Siddiqui R, Khan NA. Biology and pathogenesis of Acanthamoeba. Parasit Vectors. 2012;5:6.
Yang Y, Hu X, Min L, Dong X, Guan Y. Balamuthia mandrillaris-related primary amoebic encephalitis in China diagnosed by next generation sequencing and a review of the literature. Lab Med. 2020;51(2):e20-6.
Wu X, Yan G, Han S, Ye Y, Cheng X, Gong H, Yu H. Diagnosing Balamuthia mandrillaris encephalitis via next-generation sequencing in a 13-year-old girl. Emerg Microbes Infect. 2020;9(1):1379–87.
Krasaelap A, Prechawit S, Chansaenroj J, Punyahotra P, Puthanakit T, Chomtho K, Shuangshoti S, Amornfa J, Poovorawan Y. Fatal Balamuthia amebic encephalitis in a healthy child: a case report with review of survival cases. Korean J Parasitol. 2013;51(3):335–41.
Deol I, Robledo L, Meza A, Visvesvara GS, Andrews RJ. Encephalitis due to a free-living amoeba (Balamuthia mandrillaris): case report with literature review. Surg Neurol. 2000;53(6):611–6.
Suzuki T, Okamoto K, Genkai N, Kakita A, Abe H. A homogeneously enhancing mass evolving into multiple hemorrhagic and necrotic lesions in amoebic encephalitis with necrotizing vasculitis. Clin Imaging. 2020;60(1):48–52.
Doyle JS, Campbell E, Fuller A, Spelman DW, Cameron R, Malham G, Gin D, Lewin SR. Balamuthia mandrillaris brain abscess successfully treated with complete surgical excision and prolonged combination antimicrobial therapy. J Neurosurg. 2011;114(2):458–62.
Kobayashi S, Tsukadaira A, Kobayashi S, Izumiyama S, Yoon HS. Amoebic encephalitis in a farmer. Pathology. 2015;47(7):720–2.
Galarza M, Cuccia V, Sosa FP, Monges JA. Pediatric granulomatous cerebral amebiasis: a delayed diagnosis. Pediatr Neurol. 2002;26(2):153–6.
Tavares M, Correia da Costa JM, Carpenter SS, Santos LA, Afonso C, Aguiar A, Pereira J, Cardoso AI, Schuster FL, Yagi S, et al. Diagnosis of first case of Balamuthia amoebic encephalitis in Portugal by immunofluorescence and PCR. J Clin Microbiol. 2006;44(7):2660–3.
Yohannan B, Feldman M. Fatal Balamuthia mandrillaris Encephalitis. Case Rep Infect Dis. 2019;2019:9315756.
Lehmer LM, Ulibarri GE, Ragsdale BD, Kunkle J. Cutaneous Balamuthia mandrillaris infection as a precursor to Balamuthia amoebic encephalitis (BAE) in a healthy 84-year-old Californian. Dermatol Online J. 2017;23:7.
Acknowledgements
The authors are grateful to the patient for consent to the publication of this case report.
Funding
Data collection, analysis, and interpretation of the study were supported by Grants from the National Nature Science Foundation of China (82060236) and Natural Science Foundation of Guangxi Province (CN) (2019GXNSFDA245032) which Wen Huang is the Principal Investigator.
Author information
Authors and Affiliations
Contributions
LMP, QZ, YW, XLC, ZLL, MHS, YCY, and WH were all directly involved in the clinical management of this case. LMP and QZ are equal contributors to this study. YW was a major contributor in writing the manuscript under the guidance of WH. WH reviewed and revised the whole manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication. A copy of the written consent is available for review by the editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
CARE Checklist of information to include when writing a case report
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peng, L., Zhou, Q., Wu, Y. et al. A patient with granulomatous amoebic encephalitis caused by Balamuthia mandrillaris survived with two excisions and medication. BMC Infect Dis 22, 54 (2022). https://doi.org/10.1186/s12879-021-07020-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-021-07020-8