
Abstract
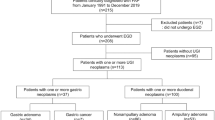
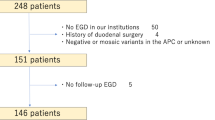
Adenomatous polyps and adenocarcinomas of the periampullary region are the most common upper gastrointestinal neoplasms encountered in familial adenomatous polyposis (FAP) patients. Tumors arising from the liver, biliary tract, and pancreas have also been reported. The purpose of this study was to review the clinical outcome of FAP patients after pancreaticoduodenal surgery for periampullary neoplasms. Of the 61 individuals participating in our prospective FAP registry, 8 underwent surgical resection of periampullary neoplasms between 1987 and 1998. The charts of these individuals were reviewed for clinical indications, type of pancreaticoduodenal surgery, postoperative complications, and outcome. Of the 8 patients identified, 7 had pancreaticoduodenectomy and 1 had duodenotomy with ampullectomy. The indications for surgery were periampullary cancer (3), severe dysplasia within a duodenal villous tumor (4), and solid-pseudopapillary tumor of the pancreas (1). At the time of pancreaticoduodenal surgery, patients ranged in age from 29–65 years, and all but one had undergone colorectal surgery, on average 16 years beforehand. Pancreatic ascites after a pylorus-sparing pancreaticoduodenectomy was the only surgical complication. At a median follow-up of 70.5 months (range 37–162), 2 patients had died, neither from their periampullary neoplasm. The patient treated by local excision subsequently developed gastric cancer arising from a polyp and went on to gastrectomy. Another patient developed confluent benign jejunal adenomas just beyond the gastroenteric anastomosis almost 12 years after pancreaticoduodenectomy for severe dysplasia of a duodenal villous adenoma. Pancreaticoduodenectomy is a safe and appropriate surgical option for FAP patients with duodenal villous tumors containing severe dysplasia or carcinoma. Postoperative morbidity was minimal and there was no perioperative mortality. Good long-term prognosis can be expected in completely resected patients although subsequent proliferative and/or neoplastic lesions may still be detected in the gastrointestinal tract with prolonged follow-up.
Similar content being viewed by others

References
Kinzler KW, Nilbert MC, Su LK, et al. Identification of FAP locus genes from chromosome 5q21. Science 1991;253(5020):661–665.
Guillem JG, Smith AJ, Calle JP, Ruo L. Gastrointestinal polyposis syndromes. Curr Probl Surg 1999;36(4):217–323.
Belchetz LA, Berk T, Bapat BV, et al. Changing causes of mortality in patients with familial adenomatous polyposis. Dis Colon Rectum 1996;39(4):384–387.
Jagelman DG, Decosse JJ, Bussey HJ. Upper gastrointestinal cancer in familial adenomatous polyposis. Lancet 1988;1(8595):1149–1151.
Vasen HF, Bulow S, Myrhoj T, et al. Decision analysis in the management of duodenal adenomatosis in familial adenomatous polyposis. Gut 1997;40(6):716–719.
Offerhaus GJ, Giardiello FM, Krush AJ, et al. The risk of upper gastrointestinal cancer in familial adenomatous polyposis. Gastroenterology 1992;102(6):1980–1982.
Iwama T, Mishima Y, Utsunomiya J. The impact of familial adenomatous polyposis on the tumorigenesis and mortality at the several organs. Its rational treatment. Ann Surg 1993; 217(2):101–108.
Arvanitis ML, Jagelman DG, Fazio VW, et al. Mortality in patients with familial adenomatous polyposis. Dis Colon Rectum 1990;33(8):639–642.
Marcello PW, Asbun HJ, Veidenheimer MC, et al. Gastroduodenal polyps in familial adenomatous polyposis. Surg Endosc 1996;10(4):418–421.
Sanabria JR, Croxford R, Berk TC, et al. Familial segregation in the occurrence and severity of periampullary neoplasms in familial adenomatous polyposis. Am J Surg 1996; 171(1):136–141.
Wallace MH, Phillips RK. Upper gastrointestinal disease in patients with familial adenomatous polyposis. Br J Surg 1998;85(6):742–750.
Enomoto M, Konishi M, Iwami T, et al. The relationship between frequencies of extracolonic manifestations and the position of APC germline mutation in patients with familial adenomatous polyposis. Jpn J Clin Oncol 2000;30(2)82–88.
Davies DR, Armstrong JG, Thakker N, et al. Severe Gardner syndrome in families with mutations restricted to a specific region of the APC gene. Am J Hum Genet 1995;57(5):1151–1158.
Leggett BA, Young JP, Biden K, et al. Severe upper gastrointestinal polyposis associated with sparse colonic polyposis in a familial adenomatous polyposis family with an APC mutation at codon 1520. Gut 1997;41(4):518–521.
Spigelman AD, Williams CB, Talbot IC, et al. Upper gastrointestinal cancer in patients with familial adenomatous polyposis. Lancet 1989;2(8666)783–785.
Noda Y, Watanabe H, Iida M, et al. Histologic follow-up of ampullary adenomas in patients with familial adenomatosis coli. Cancer 1992;70(7):1847–1856.
Heiskanen I, Kellokumpu I, Jarvinen H. Management of duodenal adenomas in 98 patients with familial adenomatous polyposis. Endoscopy 1999;31(6):412–416.
Debinski HS, Spigelman AD, Hatfield A, et al. Upper intestinal surveillance in familial adenomatous polyposis. Eur J Cancer 1995;31A(7-8):1149–1153.
Soravia C, Berk T, Haber G, et al. Management of advanced duodenal polyposis in familial adenomatous polyposis. J Gastrointest Surg 1997;1(5):474–478.
Norton ID, Gostout CJ. Management of periampullary adenoma. Dig Dis 1998;16(5):266–273.
Causeret S, Francois Y, Griot JB, et al. Prophylactic pancreaticoduodenectomy for premalignant duodenal polyposis in familial adenomatous polyposis. Int J Colorectal Dis 1998; 13(1):39–42.
Penna C, Bataille N, Balladur P, et al. Surgical treatment of severe duodenal polyposis in familial adenomatous polyposis. Br J Surg 1998;85(5):665–668.
Wallace MH, Phillips RK. Preventative strategies for periampullary tumours in FAP. Ann Oncol 1999;10(Suppl 4):201–203.
Iwama T, Tomita H, Kawachi Y, et al. Indications for local excision of ampullary lesions associated with familial adenomatous polyposis. J Am Coll Surg 1994;179(4):462–464.
Penna C, Phillips RK, Tiret E, Spigelman AD. Surgical polypectomy of duodenal adenomas in familial adenomatous polyposis: Experience of two European centres. Br J Surg 1993;80(8):1027–1029.
Alarcon FJ, Burke CA, Church JM, van Stolk RU. Familial adenomatous polyposis: Efficacy of endoscopic and surgical treatment for advanced duodenal adenomas. Dis Colon rectum 1999;42(12):1533–1536.
Farnell MB, Sakorafas GH, Sarr MG, et al. Villous tumors of the duodenum: Reappraisal of local vs. extended resection. J GASTROINTEST SURG 2000;4(1):13–23.
Cahen DL, Fockens P, de Wit LT, et al. Local resection or pancreaticoduodenectomy for villous adenoma of the ampulla of Vater diagnosed before operation. Br J Surg 1997;84(7):948–951.
Kadmon M, Tandara A, Herfarth C. Duodenal adenomatosis in familial adenomatous polyposis coli. A review of the literature and results from the Heidelberg Polyposis Register. Int J Colorectal Dis 2001;16(2):63–75.
Braasch JW, Deziel DJ, Rossi RL, et al. Pyloric and gastric preserving pancreatic resection. Experience with 87 patients. Ann Surg 1986;204(4):411–418.
Crist DW, Sitzmann JV, Cameron JL. Improved hospital morbidity, mortality, and survival after the Whipple procedure. Ann Surg 1987;206(3):358–365.
Andersen HB, Baden H, Brahe NE, Burcharth F. Pancreaticoduodenectomy for periampullary adenocarcinoma. J Am Coll Surg 1994;179(5):545–552.
Yeo CJ, Sohn TA, Cameron JL, et al. Periampullary adenocarcinoma: Analysis of 5-year survivors. Ann Surg 1998; 227(6):821–831.
Beckwith PS, van Heerden JA, Dozois RR. Prognosis of symptomatic duodenal adenomas in familial adenomatous polyposis. Arch Surg 1991;126(7):825–828.
Bleau BL, Gostout CJ. Endoscopic treatment of ampullary adenomas in familial adenomatous polyposis. J Clin Gastroenterol 1996;22(3):237–241.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ruo, L., Coit, D.G., Brennan, M.F. et al. Long-term follow-up of patients with familial adenomatous polyposis undergoing pancreaticoduodenal surgery. J Gastrointest Surg 6, 671–675 (2002). https://doi.org/10.1016/S1091-255X(02)00045-8
Issue Date:
DOI: https://doi.org/10.1016/S1091-255X(02)00045-8