
Abstract
Objectives
Sleep problems in children on the autism spectrum may be affected by core diagnostic characteristics, including stereotypy (restricted and repetitive behaviors). Little is known about the nature of sleep-related stereotypy and its role within sleep disturbance. This study aimed to improve our understanding of the types of sleep-related stereotypy, its potential role within sleep difficulties, and how parents manage night-time stereotypy, in children on the autism spectrum.
Methods
This qualitative study used thematic analysis to analyze clinical assessment reports obtained from 21 parents of children on the autism spectrum referred for behavioral sleep intervention. Five themes, including the types of stereotypy, timing within sleep problems, stereotypy as sleep-interfering, stereotypy as sleep-conducive, and parent-responses, were identified. A clinical case study illustrates the potential role of vocal stereotypy within night wakings, through functional assessment and treatment of sleep problems in a child on the autism spectrum.
Results
Stereotypy included vocal and motor behaviors and repetitive manipulation of objects. Parents perceived stereotypy as both problematic and as beneficial to sleep, which may differentially affect behavioral treatment. Parent responses to stereotypy were varied and included co-sleeping. The case study highlights the complexity of the sleep and stereotypy relationship and the difficulty in treating automatically maintained behavior in the sleep context.
Conclusion
The function that stereotypy serves in relation to sleep disturbance is unclear and may differ across and within children. It is important we seek to better understand the specific ways that stereotypy may affect sleep, and vice versa, to improve clinical management of sleep problems in children on the autism spectrum.
Similar content being viewed by others

Sleep problems in children on the autism spectrum are ubiquitous, affecting up to 80% of children across all cognitive levels (Abel et al., 2018; Cohen et al., 2014). The most frequently reported sleep difficulties are associated with sleep onset and maintenance and include sleep onset delay (SOD), frequent and prolonged night wakings (NWs), poor sleep efficiency, and reduced total sleep time (Cortesi et al., 2010; Johnson et al., 2018; Singh & Zimmerman, 2015). These problems are often accompanied by bedtime resistance, daytime sleepiness, disruptive behaviors (e.g., calling out to parents and caregivers [hereafter referred to as parents], screaming or crying, playing with toys or objects), and unwanted co-sleeping (Cortesi et al., 2010; Kirkpatrick et al., 2019; McLay et al., 2021a; Richdale & Schreck, 2009). Sleep problems in such children do not tend to remit without treatment, often persisting throughout adolescence (Goldman et al., 2012; Mazurek et al., 2019; Sivertsen et al., 2012).
Inadequate sleep has significant detrimental effects on children’s daytime functioning and wellbeing, including increased internalizing and externalizing behavior (e.g., anxiety, aggression) and reduced cognitive and adaptive functioning, and impaired physical health (e.g., obesity, epilepsy; Accardo & Malow, 2015; Bangerter et al., 2020; Cohen et al., 2018; Delahaye et al., 2014; Taylor et al., 2012; Zuckerman et al., 2014). Furthermore, sleep disturbance may exacerbate autism symptom severity, with higher rates of stereotypy and social impairment found in children on the autism spectrum who are also poor sleepers (Abel et al., 2018; Adams et al., 2014; Gabriels et al., 2005; Hundley et al., 2016; Park et al., 2012; Schreck et al., 2004; Veatch et al., 2017). Parents of children with sleep problems are also at heightened risk of sleep deprivation, resulting in elevated levels of stress, anxiety, depression, fatigue, relationship discord, and familial dysfunction (Chu & Richdale, 2009; Johnson et al., 2018; Levin & Scher, 2016; Martin et al., 2019; Meltzer, 2011). Thus, there are many reasons to seek timely and effective treatment of sleep problems to remediate the widespread effects of sleep deprivation (Goldman et al., 2012; Singh & Zimmerman, 2015).
The etiology of sleep disturbance in autism is unknown; however, it is widely agreed that the causes are multifactorial, involving biological, psychological, behavioral, social, medical, and environmental factors, either alone or in combination (Cohen et al., 2014; Cortesi et al., 2010; Mazzone et al., 2018; Richdale & Schreck, 2009). Inclusive within these contributing factors, sleep problems often have a behavioral basis. Sleep is a bio-behavioral state that reinforces the behavior of falling asleep. Falling asleep can be understood as the end point of an operant chain, which begins with bed-preparatory behaviors (e.g., putting on pyjamas, brushing teeth) and ends with behavioral quietude (i.e., lying quietly in bed, with low levels of behavioral, cognitive and emotional arousal; Blampied & Bootzin, 2013; Blampied & France, 1993). Behavioral quietude must be maintained for a sufficient period of time in order for the wake-sleep transition to occur (Blampied, 2013; Blampied & France, 1993). Sleep problems can develop and be maintained when children engage in problem behavior (e.g., calling out, leaving the bed, stereotypy) that disrupts the behavioral chain of falling asleep (Blampied, 2013). Parent responses (e.g., providing attention) to child behavior may also inadvertently reinforce these behaviors (Beresford et al., 2016; Blampied, 2013; Blampied & France, 1993; Richdale & Schreck, 2009). Furthermore, the core characteristics of autism may interfere with the behavioral chain of falling asleep, including that children may experience difficulty transitioning between tasks and interpreting social expectations related to going to bed and to sleep (Mazzone et al., 2018; Reynolds & Malow, 2011; Richdale & Schreck, 2009).
Extant research suggests that stereotypy (e.g., repetitive vocalizations or motor movements) can accompany sleep problems (e.g., SOD, NWs) in children on the autism spectrum (Hunter et al., 2021; Jin et al., 2013; Malow et al., 2006; McLay et al., 2019; Richdale & Schreck, 2009; Weiskop et al., 2005). For example, in a recent case analysis by McLay et al. (2021a) of 41 children and adolescents on the autism spectrum with sleep problems, 27% of participants exhibited stereotypy in the sleep context. Stereotypic behaviors in children on the autism spectrum are heterogeneous, but can broadly be classified as either motor stereotypy, consisting of motor movements (e.g., hand-flapping, body-rocking), repetitive manipulation of objects (RMO; e.g., mouthing or spinning objects), or vocal stereotypy, involving non-contextual vocalizations (i.e., without a clear communicative purpose, e.g., recurring words or non-word sounds; Ahearn et al., 2007; Akers et al., 2020; Cunningham & Schreibman, 2008; DiGennaro Reed et al., 2012; Wang et al., 2020). All forms of stereotypy share a response topography of repetition, invariance, and atypicality (Didden et al., 2012; Rapp & Vollmer, 2005). Stereotypy is an operant behavior that frequently functions to produce automatic reinforcement; that is, the behavior is intrinsically reinforced via non-social sensory consequences (Ahearn et al., 2007; DiGennaro Reed et al., 2012; Rapp & Lanovaz, 2016; Rapp & Vollmer, 2005). There is also evidence to suggest that stereotypy can be socially mediated, through contingencies of positive (e.g., social attention) and negative (e.g., escape from demands) reinforcement (Durand & Carr, 1987; Kennedy et al., 2000; Roantree & Kennedy, 2006; Wilke et al., 2012). Without intervention, stereotypy tends to persist throughout the lifespan and may increase in frequency and intensity over time (Akers et al., 2020; Bodfish et al., 2000; Wang et al., 2020).
Stereotypy can be problematic when the intensity of and/or persistence in the behavior impedes an individual’s adaptive functioning; for example, stereotypy can significantly interfere with socialization and learning in children on the autism spectrum (Akers et al., 2020; Lydon et al., 2017; Wang et al., 2020). Stereotypy can also disrupt family functioning and is associated with severe parental stress (Boyd et al., 2012). As such, stereotypy is a common target for intervention, particularly in the educational setting (Akers et al., 2020; Wang et al., 2020). There is also evidence to suggest that stereotypy may serve as a coping mechanism for individuals on the autism spectrum, possibly helping to alleviate distress and to regulate thoughts and feelings (Gabriels et al., 2005, 2013; McCarty & Brumback, 2021). Individuals on the autism spectrum may report experiencing stereotypy as comforting, calming, and enjoyable (McCarty & Brumback, 2021). In comparison to the literature on daytime stereotypy, very little is known about sleep-related stereotypy (Hunter et al., 2021). The reasons why children on the autism spectrum engage in stereotypy in the sleep context are currently unclear and may be multifaceted across and within individuals (Cunningham & Schreibman, 2008; Kennedy et al., 2000). For example, automatic reinforcement generated through stereotypy may be positive (i.e., producing a sensory consequence) and/or negative (i.e., reducing or eliminating a sensory experience, such as physical discomfort or pain [an instance of escape/avoidance]; Leader & Mannion, 2016). It is possible that sleep-related stereotypy may serve a self-settling purpose, such as rhythmic movements (RM; e.g., body-rocking, head-banging) commonly observed in infants and young children during the sleep onset period (Haywood & Hill, 2012; Hoban, 2003). As for RM and daytime stereotypy, however, sleep-related stereotypy may be considered problematic when persistence in the behavior incurs a clinical consequence including interference with adaptive functioning (Didden et al., 2012; Gwyther et al., 2017). Specifically, in the sleep context, after a child is bid goodnight, stereotypy may become sleep-interfering if it inhibits a child’s ability to establish and maintain the behavioral quietude necessary to initiate and/or re-initiate sleep (i.e., if the child wakes and engages in stereotypy; Hunter et al., 2021; Jin et al., 2013; McLay et al., 2019).
The relationship between autism and sleep problems is understood to be complex and cyclical; for example, greater autism symptom severity may predict greater severity of sleep problems, and vice versa (Adams et al., 2014; Cohen et al., 2014; Hollway & Aman, 2011; Hundley et al., 2016; Schreck et al., 2004). However, the mechanisms of this relationship are currently unclear; a majority of research examining this relationship has been cross-sectional and correlational in design, thereby limiting our understanding of causality and directionality (Adams et al., 2014; Schreck & Richdale, 2020). This includes the impact that stereotypy may have on sleep in children on the autism spectrum, which is not well understood (Hunter et al., 2021). The nature of this relationship requires further investigation, including whether stereotypy primarily interferes with sleep onset, whether it may serve a self-settling function for some children, or whether in fact it may have no impact on sleep (i.e., occur simply by virtue of the child being awake). Furthermore, sleep-related stereotypic behaviors are not well characterized, including the patterns of behavior specific to individuals (Gabriels et al., 2005). For example, it is not clear whether stereotypy differs in topography or function from that which children engage in throughout the day. Better understanding of the types of stereotypy that children on the autism spectrum exhibit at night, and how these behaviors may affect sleep, can provide an avenue for targeted treatment that can generate important primary and secondary benefits for children and parents (Boyd et al., 2012; Cohen et al., 2014; Delahaye et al., 2014; Hundley et al., 2016; Hunter et al., 2020; Mazurek et al., 2019; McLay et al., 2021b).
Typically, it is parents who can detect and respond to children’s sleep problems and stereotypy. Thus, parents can provide valuable insight into stereotypy that occurs in the context of sleep, particularly where self-report is not possible (e.g., owing to younger age and/or limited verbal ability). The present study involved qualitative analysis of semi-structured clinical interviews with the parents of children on the autism spectrum who were assessed for a behavioral sleep intervention. This study examined parent descriptions of stereotypy in relation to sleep disturbance, including types and topography of stereotypic behavior, occurrence within sleep problems, the impact of stereotypy on sleep onset, and parent response to stereotypic behavior. Parent-reported information was then examined with the aim of enhancing our understanding of (a) the types and topography of stereotypy exhibited by children on the autism spectrum at night; (b) the potential role of stereotypy within sleep difficulties (e.g., whether stereotypy interferes with sleep); and (c) how parents manage stereotypy in the sleep context.
Methods
Participants
The participants were parents of a child or adolescent (henceforth referred to as “child”) on the autism spectrum, who was referred or self-referred to a specialist clinic to receive behavioral sleep intervention services. Children who received services were part of a wider study designed to investigate the effectiveness of function-based, parent-implemented interventions for children on the autism spectrum. To be eligible to receive services, children met the following inclusion criteria: (a) aged between 3 and 17 years; (b) a formal diagnosis of autism (American Psychiatric Association, 2013) confirmed by a pediatrician; (c) parent-reported sleep problems including SOD, NWs, bedtime resistance, and/or unwanted co-sleeping, later confirmed by formal assessment measures (e.g., the Children’s Sleep Habits Questionnaire [CSHQ; Owens et al., 2000] and analysis of videosomnography [VSG]). CSHQ total scores were available for 10 children in this study and are included as Supplementary Information (S1); 8/10 children exceeded the clinical cut-off score (41). This study reports findings from a subset of children who engaged in at least one form of stereotypy (e.g., repetitive vocalizations) during sleep onset and/or NWs. Children were excluded from the study if there was contraindication for a behavioral intervention (e.g., if they had a medical condition that affected their sleep).
Parent participants included 21 parents of 15 children on the autism spectrum (see child details below). In six families, both parents participated in the interview; in five families, one parent from a two-parent household participated in the interview, and four children had a solo parent. Parent’s ethnicity included European (n = 14), New Zealand European/Māori (n = 4), Asian (n = 2), and South African (n = 1). Two parents in the same household spoke English as a second language. In 11 families, one or both parents were employed, and in four families, the solo caregiver was unemployed or retired.
Child participants were 11 boys and four girls, aged between 3 and 15 years (median: 5 years). Only one participant was an adolescent (15 years), all other children were ≤ 8 years, and 11 of the 15 children were ≤ 6 years. Co-occurring conditions, as diagnosed by a pediatrician (n = 5) included rare genetic neurodevelopmental disorders (e.g., chromosomal deletions; n = 4), intellectual disability (n = 4), global developmental delay (n = 1) and attention deficit hyperactivity disorder (ADHD; n = 1). Verbal ability ranged from non-verbal (n = 3), language-delayed (i.e., below chronological age, e.g., limited to single words/short sentences; n = 11), and no language difficulties (n = 2). Four children took melatonin at the time of the interview, the remainder were unmedicated. The types of child sleep problems reported were NWs (n = 11, 73%), SOD (n = 10, 67%), unwanted co-sleeping (n = 7, 47%), and bedtime resistance (n = 2, 13%). Eleven children (73%) were reported to have two or more sleep problems.
Procedure
Settings and Personnel
A clinical interview was conducted by the first author (12 families), or another research clinician who was an intern psychologist (three families) as part of a comprehensive intake assessment. The first author, a trained psychologist and doctoral student, has a background in sleep and autism research and experience in clinical interviewing. The interview was conducted either in person or via videoconferencing and was a pre-cursor to the development of an individualized, parent-implemented, behavioral sleep intervention.
Semi-structured Interviews
Following a screening interview and informed consent processes, parents participated in a 1–1.5-h-long, open-ended, semi-structured interview. The purpose of the intake interview was to comprehensively assess each child’s sleep problems, in the context of broader child and family factors. The interview began with a discussion of the child’s presenting sleep problems, including types of sleep problems (e.g., SOD, NWs), typical bedtime routine (e.g., time put to bed, steps in the sequence leading up to bedtime), history of sleep disturbance (e.g., onset of the sleep problem, chronicity) and impact (i.e., on child, parents, wider family) of sleep disturbance. Parents were also asked to describe children’s behavior after they were bid goodnight, including stereotypy. Parents were asked to describe the topography of their child’s night-and day-time stereotypy, setting (e.g., physical location, timing within sleep problems), consequences of the stereotypic behavior (e.g., parent response), their perception of the impact of their response on stereotypy, and parent’s view of the role of their child’s stereotypy in relation to sleep (e.g., what impact, if any, stereotypy had on sleep onset). A list of the questions asked about stereotypy is included as Supplementary Information (S2). If a parent reported more than one type of night-time stereotypic behavior, then questions were asked in relation to each type (e.g., what impact [if any] each of the behaviors had on sleep). Parents also spoke about stereotypy in response to questions non-specific to stereotypy, for example, “tell me what your child does when they wake during the night?” A full developmental history and relevant child (e.g., interests, schooling) and family information (e.g., living situation including sleeping arrangements, employment, parental mental health and wellbeing, sources of support) was also obtained. Finally, parents were asked about their goals for their child’s sleep. A full list of clinical assessment questions is available from the corresponding author upon request.
Data Analyses
This research was conducted within a theoretical thematic analysis framework (Braun & Clarke, 2006), driven by the researcher’s theoretical and analytical interest in stereotypy in relation to sleep disturbance (i.e., the first author focused on the particular feature of stereotypy when coding the data). Themes were identified through a semantic approach, involving a progression from the organization of parent description to interpretation (Braun & Clarke, 2006). This framework enabled exploration of the phenomenon of stereotypy in relation to sleep disturbance in children on the autism spectrum; drawing on parents’ perspectives of their child’s behavior via an interpretive paradigm enabled unique insight into the characteristics of, and parent experiences with, sleep-related stereotypy (Belotto, 2018).
Clinical assessment reports for each child (n = 15) were analyzed by the first author, under the supervision of the second and fourth author, following the guidelines of Braun and Clarke (2006). Thematic analysis involved initially reading and re-reading the reports to ensure familiarization with the parent accounts. All information pertaining to stereotypy were then manually coded, to generate an initial list of codes, and verbatim statements were extracted. Next, the initial codes were organized into broader themes and sub-themes and reviewed for relevance to the research questions. The themes and codes were then refined until definitive codes and themes were established (Braun & Clarke, 2006). The second and fourth authors checked the definitive codes and themes for consistency and coherence.
Reliability
Interrater reliability was assessed for the thematic analysis (Elliot, 2018; O’Connor & Joffe, 2020). A research assistant, who was part of the wider sleep research team with experience conducting sleep treatment research, independently coded the report information for eight (53%) randomly selected, de-identified participants. Interrater reliability was calculated using the formula [Agreement/ (Agreement + Disagreement)] × 100%. Data pertaining to stereotypy were recorded as an agreement if the same definitive code was applied by both the first author and the research assistant. First, the research assistant independently coded the report information for two participants (i.e., to establish satisfactory reliability); the research assistant and first author compared the two sets of coded information and calculated the level of agreement (75% and 80%; Belotto, 2018; O’Connor & Joffe, 2020). Instances of disagreement were discussed and resolved using a process of negotiated agreement; in this case, all disagreements were reconciled through one person deferring to the other, and 100% agreement was reached across both participants (Belotto, 2018; Elliot, 2018). This process was then repeated for the other six participants; initial agreement was 90%, 79%, 71%, 60%, 78%, and 75%. Following discussion, the wording of three codes was amended to resolve ambiguity (e.g., whether stereotypy was a “predominant” behavior) and improved consensus in interpretation (Elliot, 2018); these codes were then re-applied across all data sets to ensure consistency, and 100% agreement was reached. A full list of definitive codes and themes is available from the corresponding author upon request.
Results
The findings of the qualitative analysis of the 15 interview reports are presented below. Five themes, including (1) type and topography of stereotypy; (2) timing of stereotypy; (3) stereotypy as sleep-interfering; (4) stereotypy as sleep-conducive; and (5) parent responses to stereotypy, were identified. Two sub-themes, (a) co-sleeping and (b) escalation, were identified within the “parent responses to stereotypy” and “stereotypy as sleep-interfering” themes, respectively.
Type and Topography of Stereotypy
Parents described a diverse range of stereotypic behaviors exhibited by children on the autism spectrum, in the sleep context. Akin to daytime stereotypy, night-time stereotypy could be grouped into motor behaviors, vocal behaviors, or RMO. Vocal stereotypy (n = 11 children, 73%) encompassed non-word sounds (i.e., throat clearing, humming, croaking, groaning, “babbling,” non-contextual “belly/hysterical” laughing, and squealing), repetition of words (i.e., numbers and letters), and scripting (i.e., television phrases, song lyrics). Many parents described their child’s vocalizations as “talking to him/herself.” Vocalizations were often related to children’s preferences (e.g., Thomas the Tank Engine: “you’re a very useful engine”). Motor behaviors (n = 10, 67%) included repetitive bouncing (on bottom), hand-flapping, body-rocking (on stomach or standing), flicking legs, twiddling fingers, head-banging, and body-rolling (side to side). One parent described their child’s stereotypy as “hip thrashing” on his stomach, while another parent reported “she rocks before she falls asleep, and sucks her thumb, so rocks in a way that doesn’t interfere with her thumb-sucking…sort of pushes off the bed with the other arm.” RMO (n = 4, 27%) was the least common form, and included lining up toys and spinning toy car wheels, twiddling items (e.g., a pen), sniffing a scarf, and manipulating magazine pages: “she will fiddle with pages, and sort of nibble the centre.” Frequently, parents reported that children (n = 8, 53%) engaged in multiple forms of stereotypy, with vocal and motor stereotypy being the most common combination (e.g., simultaneous bouncing and squealing).
Timing of Stereotypy
The timing of when children’s stereotypy occurred was identified as a theme. Six children (40%) engaged in stereotypy during both sleep onset and NWs. Four children (27%) engaged in stereotypy during sleep onset only; and NWs were not a parent-reported problem. Five children (33%) exhibited stereotypy during NWs only; in three of these children, sleep onset was managed with melatonin, and for the other two, sleep onset was not a parent-reported problem. Overall, parents were aware of children engaging in stereotypy both at the start of and during the night if the child woke.
Stereotypy as Sleep-Interfering
Many parents indicated that stereotypic behaviors resulted in the child having difficulty initiating and/or re-initiating sleep. For nine children (60%), stereotypic behaviors were reported to be sleep-interfering; eight of these children (89%) engaged in vocal stereotypy, accompanied in some cases by motor stereotypy (n = 3) and RMO (n = 1). The ninth child engaged in RMO; it was unclear to her parents if she also vocalized. Sleep-interfering stereotypy was often referred to as “play,” with parents indicating the child was in a stimulated state (e.g., “wired,” “vocally active,” or “bouncing off the walls”) and became more wide awake (e.g., “winding/ramping up”) when engaging in stereotypy. Interestingly, a sub-theme was identified, where vocalizations escalated. Specifically, in three children, vocalizations were reported to begin quietly and infrequently, but then to intensify as time went on, particularly in volume. According to one parent: “he starts by whispering numbers and letters to himself.” The child would then “get louder, and start shouting, and get more excited.” In two children, when vocalizations escalated, motor stereotypy also occurred (e.g., the child began bouncing, whilst shouting/laughing). Parents termed nights when children vocalized as “bad” or “unlucky” nights, and vocal stereotypy was strongly viewed as sleep-competing: “the more he babbles, the harder it is for him to get to sleep.” A parent stated “it’s as though (the child) wants to go to sleep, but he’s fighting his body and brain that is keeping him more awake.” Overall, it appeared that in a majority of children, stereotypy, particularly vocal stereotypy, made the initiation of sleep difficult.
Stereotypy as Sleep-Conducive
A contrasting theme was stereotypy as sleep-conducive; including parent report that stereotypy was beneficial to the child (e.g., soothing), and/or the stereotypy occurred during the wake-sleep transition. Stereotypic behaviors in six children (40%), all motor, were classed as sleep-conducive. One parent described her child’s continuous bouncing as a “wind-down” and stated “it helps him prepare for sleep.” Body rolling in another child was described as: “he holds a blanket over him and does his death roll, like a crocodile, he thrashes from side to side.” Another child engaged in a side-to-side rock whilst standing on the bed, pushing off the wall with one hand, until she physically “dropped” into a sleep state: “she has to work very hard to fall asleep.” Interestingly, in five of these children (83%), sleep-conducive motor stereotypy only occurred at night. This was in contrast to vocal stereotypy and RMO, which were frequently reported to also occur throughout the day. One exception was the child who engaged in a standing-rock during the wake-sleep transition, who also rocked (swayed side-to-side) whilst standing throughout the day, albeit at a reduced intensity.
Notably, two children (13%; with severe SOD) were reported to exhibit both sleep-interfering and sleep-conducive stereotypy. In these children, sleep-interfering stereotypy (bouncing, squealing and hand-flapping for one child; RMO with magazines for the other) occurred extensively throughout the day and the sleep onset period. Sleep-conducive stereotypy (body-rolling, and body-rocking, respectively) occurred immediately prior to falling asleep, specific to the wake-sleep transition. Overall, parent report suggests that children’s repetitive behaviors may serve different roles in relation to sleep disturbance, across and within children.
Parent Responses to Stereotypy
Parent responses to stereotypy varied and included no response/ignoring the behavior (i.e., purposefully withholding attention), giving a verbal instruction (e.g., to cease the behavior and/or to go to sleep), and co-sleeping (in the child or parent bed). Parents had a tendency to ignore vocal stereotypy when it occurred at low volume, but to intervene with a verbal instruction (e.g., “it’s time for sleep”) when vocalizations escalated: “if he is being loud, then one of us will go in and have stern words with him.” Seven families co-slept; among parents who co-slept, five (71%) reported doing so as reactive response to NWs, while two families co-slept from the beginning of the night. Interestingly, a sub-theme was identified regarding parent’s intentional use of co-sleeping to manage stereotypy. Parents recounted using their body to try to physically restrict children’s motor stereotypy: “(parent) will use our body, an arm and a leg, to physically help to hold (child) down to try to calm his body enough to help him to get off to sleep.” Parents saw their presence as helpful in reducing motor movements: “so long as I lie with him, he doesn’t bounce” and “if I don’t co-sleep with her, she’ll stand up and rock.” Parents also co-slept in response to vocal stereotypy, particularly if less intensive attempts (i.e., ignoring, verbal instructions) to interrupt vocalizations were unsuccessful. Parent report indicated that children tended to vocalize despite parental presence. One parent explained that their child was unlikely to resettle when brought into the parent bed, instead going into “his own world” continuing to “babble and chat to himself.” Overall, parent responses to children’s behavior varied across and within families. Although coded, not enough data were available to generate a theme regarding the impact of parent response on the child’s behavior (i.e., whether behavior increased, decreased, or was unaltered); thus, it remains unclear.
Case Study
The following case study is provided to expand on the outcomes of the thematic analysis, by further illustrating the potential role of vocal stereotypy within sleep difficulties in a child on the autism spectrum, including examination of the effects of targeted treatment on vocal stereotypy.
Participant, Function-Informed Case Conceptualization, and Treatment Planning
James (pseudonym) was a 7-year-and-10-month-old boy with a diagnosis of autism. James had limited verbal ability and expressed his needs and wants with short sentences. He was referred by his parents for behavioral sleep intervention services, and his data are included within the thematic analysis. James’ sleep problems consisted of SOD and NWs. He had a consistent bedtime routine including taking 1 mg melatonin, and reliable bedtime that was intentionally delayed by his parents (10.00 p.m.) as a means of managing NWs (i.e., they reported an earlier bedtime resulted in a higher frequency of NWs). After being bid goodnight, James took 30–40 min to fall asleep, during which time a parent would intermittently lie with him. His NWs, although infrequent, were long (mean 90 min, range 30–180 min). During NWs, James engaged in vocal stereotypy involving repetition of numbers, movie phrases, and non-contextual laughter. A parent co-slept with James as a pre-emptive means of managing his NWs; when he woke, the parent responded by ignoring his behavior, feigning (modelling) sleep, or using short sentences to redirect James to return to sleep. Parent report indicated these responses did not alter James’ behavior. In the morning, James woke on his own at inconsistent times and frequently napped at school during the day.
Functional behavior assessment (FBA), a comprehensive assessment process that identifies the role of the environment and learning (i.e., functions) in sleep problems (Blampied, 2013; McLay et al., 2021a), was undertaken using clinical interviewing, the Sleep Assessment and Treatment Tool (SATT; Hanley, 2005) and parent-recorded sleep diaries, to identify the factors likely to be contributing to James’ sleep problems. The SATT is an FBA measure designed to identify the topography and function of a child’s sleep problems with information obtained through parent interviews, including the antecedents (e.g., inconsistent bedtime routine), motivating operations (e.g., insufficient sleep pressure owing to naps), and reinforcement contingencies (e.g., night-time parent–child interactions) underpinning sleep problems for an individual (Jin et al., 2013). The outcomes of FBA were used to develop an individualized case conceptualization and treatment plan (Blampied, 2013). The function-informed case conceptualization indicated that multiple, antecedent, and consequence-based factors were likely to be contributing to James’ sleep problems (see Table 1; Jin et al., 2013; McLay et al., 2021a). Antecedent factors included the intermittent presence of a parent during the sleep onset period (i.e., an inconsistent discriminative stimulus for sleep onset) and decreased physiological sleep pressure owing to inconsistent wake times and daytime naps. Stereotypic vocalizations during NWs actively competed with behavioral quietude and thereby prevented the re-initiation of sleep. Parent perception of vocal stereotypy was that it was problematic (e.g., disruptive) and interfered with sleep. The reinforcing consequences for vocal stereotypy were likely to be automatic (e.g., auditory sensory feedback produced by the vocalizations), because the vocalizations occurred regardless of external consequences (e.g., if he was alone, or not; Kennedy et al., 2000; Rapp & Lanovaz, 2016). However, because vocal stereotypy often resulted in parent-attention, it was also possible that the behavior was (partially) reinforced by social attention. Parent attention (social interactions whilst awake) was also likely to contribute to the maintenance of NWs, which were further complicated by James’ reliance on a parent’s presence as a discriminative stimulus for sleep. Treatment goals were informed by parent’s preferences in accordance with normative sleep recommendations (Hirshkowitz et al., 2015), and included a reduction in SOD (i.e., ≤ 15 min), duration of vocal stereotypy and NWs. James’ parents also wished to eliminate use of melatonin (1 mg). Co-sleeping was not a parent-defined problem; however, James’ parents preferred to sleep independently if his sleep problems (particularly NWs) were able to be managed by other, more adaptive means.
Baseline and Intervention
James was randomly allocated a 3-week baseline, which was extended to a total of 36 nights (baseline 1) to accommodate family needs. Prior to intervention, melatonin (1 mg) was eliminated in accordance with parents’ goals yielding an additional 15 nights (baseline 2). With the exception of melatonin, James’ parents were asked to maintain his existing sleep habits during the baseline phases. A written copy of the treatment plan was provided to James’ parents and discussed with them to ensure consensus (Sanders & Burke, 2014).
The individualized function-based intervention was parent-implemented immediately at the end of baseline. Evidence-based treatment components were selected according to their suitability to address the function of the behavior (McLay et al., 2021a) and were implemented sequentially across treatment phases in order to independently examine the effects of each treatment component. Strategies were ordered in accordance with minimally intrusive (i.e., least restrictive and time intensive) principles (Kazdin, 1984; van Deurs et al., 2021), beginning with antecedent (e.g., altering the environment/instructional context and motivational variables for sleep) followed by consequence-based (e.g., extinction) strategies. Treatment (T) proceeded to the next phase if reductions across target sleep variables were not evident. Intervention ran for 80 nights and consisted of four sub-phases with sequential addition of treatment elements, specifically (T1) white noise (night 52 to 71); (T2) white noise, sleep restriction and visual supports (night 72 to 101); (T3) white noise, sleep restriction, visual supports, and gradual reduction of parental presence (night 102 to 121); (T4) white noise, sleep restriction, visual aids, and the full removal of parental presence (night 122 to 131). The target variables included sleep onset latency (SOL), frequency and duration of NWs, and duration of vocal stereotypy.
Vocal stereotypy was targeted first because it was identified in the FBA as a primary problem behavior, and targeting stereotypy in isolation (i.e., independently of other sleep-related variables) enabled the impact of treatment on stereotypy to be examined. It was hypothesized that if vocal stereotypy interfered with James’ ability to re-initiate sleep, then interrupting stereotypy may subsequently reduce the duration (but not frequency) of NWs. Matched stimulation in the form of white noise was selected to target the putative automatic auditory consequences produced by his vocalizations. Matched stimulation, involving continuous access to stimuli that delivers sensations similar to the putative sensory consequences for the target behavior (e.g., noncontingent access to music), is an evidence-based intervention for reducing daytime vocal stereotypy in children on the autism spectrum (Lanovaz & Sladeczek, 2012; Rapp & Lanovaz, 2016; Wang et al., 2020). The mechanism underlying the effects of matched stimulation is unclear; however, it is possible that consumption of the alternative auditory consequence satiates the child (i.e., is an abolishing operation), thereby reducing the child’s motivation to engage in vocal stereotypy (Lanovaz & Sladeczek, 2012; Michael, 1982). Consideration was also given to what was feasible for implementation in the sleep context. Matched stimulation is suited to the treatment of sleep-related stereotypy because the consummatory response of listening (i.e., to white noise) is likely to be less sleep-disruptive than the self-produced vocalizations; white noise was specifically selected because it was expected to be less stimulating than music. The use of white noise in relation to sleep is widespread (Reidy et al., 2021), and studies suggest it is a cost-effective strategy that is easily-implemented by parents in the home-setting overnight, and is well-tolerated by children (Knight & Johnson, 2014; McLay et al., 2019; Turner & Johnson, 2013).
The first treatment phase (T1) involved playing white noise (continuous rain sound) in James’ bedroom through an application on a portable device. James’ parents turned on the white noise once James was in bed and turned it off once James was awake in the morning. The volume was held consistent at 70 dB across treatment and follow-up phases; this volume helped to mask sounds whilst being comfortable for James. On night 72 (T2), sleep restriction procedures were implemented to increase physiological sleep pressure, thereby strengthening James’ motivation to initiate and maintain sleep during the night. This involved establishing a consistent morning wake time (7:30 a.m.) and the elimination of daytime naps. James’ bedtime of 10:00 p.m. was continued. In addition, visual aids in the form of a Gro-clock™ and a social “sleep” story were introduced to help to establish discriminative control for sleep-conducive behavior. The Gro-clock™ (a digital clock that displays either a star or a sun on its face, to provide unambiguous discriminative stimuli for sleeping/waking) was introduced to help to reduce NWs. An individualized sleep story, following the conventions outlined by Gray and Garand (1993), was written for James, with photos and text illustrating his sleep routine and expectations around sleep, with an emphasis on sleep-conducive behavior (e.g., lying quietly in bed). The ending depicted a reward for James for appropriate behavior. The sleep story was read to James each night as part of his bedtime routine, and at any other time upon request. On night 102 (T3), a parental presence program (i.e., extinction with graduated parental presence; France, 2011) was implemented to improve stimulus control for sleep onset (i.e., during SOL) and to eliminate the possible attention-seeking function to vocal stereotypy and NWs. During the sleep onset period, a parent sat on a chair near James’ bed without interacting with him, and during the night, following a NW, a parent slept in James’ room but in a bed separate to him. The parent was instructed to ignore James’ behavior during SOL and NWs, where safe to do so. On night 122 (T4), parental presence was fully removed; rather than sitting on a chair during SOL the parent bid James goodnight and left the room, and during the night slept in the parent bed, ignoring James’ behavior during any NWs where safe to do so. The treatment phase ended when parents felt their goals for James’ sleep had been met. Follow-up data were recorded for seven nights during short-term (STFU) and long-term (LTFU) follow-up.
Interobserver Agreement
Interobserver agreement (IOA) was calculated by a member of the research team blind to parent sleep diary recordings. The researcher coded 20–29% (mean: 25%) of VSG data across each study phase; agreement between parent report and direct observation data extracted from VSG was then calculated using the equation [Agreement/(Agreement + Disagreement)] × 100%. Measures of duration (e.g., SOD) were recorded as agreement if parent and researcher report were ± 15 min.
Results
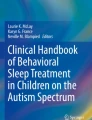
The duration of SOL (minutes), frequency and duration (minutes) of NWs, and total duration (minutes) of vocal stereotypy are shown in Fig. 1. IOA scores indicated a high degree (mean: 90%) of correspondence between objective and subjective measures of the target sleep variables. Parent ratings of treatment acceptability, and parent adherence to the behavioral sleep program, were also high.

The total duration of James’ sleep onset latency (minutes), night wakings (minutes), and vocal stereotypy (minutes) across baseline, intervention, and follow-up phases. The night waking graph also shows frequency; the numeral 2 on this graph (night 60) is the only night James’ woke twice (on all other nights he woke only once). Note. m, male; min, minutes; mo, months; LTFU, long-term follow-up; STFU, short-term follow-up; T1–T4, treatment phases 1–4; yr, years
During baseline 1, James took 30–40 min to fall asleep on average. Following the elimination of melatonin, James’ SOL during baseline ranged from 5 to 45 min (mean 21 min). In comparison to baseline 2, there was no evidence of a treatment effect during T1, T2, or T3; however, in T4, a reduction in SOL was observed, with all nights ≤ 30 min, and 7/10 nights ≤ 15 min. This effect was maintained during STFU as James fell asleep within 20 min each night (6/7 nights ≤ 15 min). At LTFU, however, a treatment effect was no longer evident.
During baselines 1 and 2, James woke infrequently but for prolonged periods of 30–210 min. During T1, there was no evidence of a treatment effect, and on one occasion James woke twice. In T2, NWs reduced to near zero, with only two wakes in 29 nights (duration: 30 and 120 min). During T3, James woke on four occasions (duration of either 60 or 120 min), and in T4 James woke on one occasion for 60 min. No NWs occurred during the follow-up phases.
During baselines 1 and 2, the duration of James’ vocal stereotypy during NWs ranged from 15 to 180 min (mean: 87 min). There was no evidence of a treatment effect on the duration of vocalizations during T1 (white noise) nor throughout the other treatment phases. Although James continued to vocalize during NWs, the occurrence of stereotypy reduced in accordance with reductions in NWs, as described above.
In sum, white noise alone had no effect on target sleep variables including vocal stereotypy. A combination of white noise, sleep restriction, and visual aids appears to have reduced the frequency of NWs, at least partially. A further change in NWs and a change in SOL were evident when the parent was subsequently fully removed from the bedroom, supporting the hypothesis that SOD and NWs were at least partially maintained by social attention. Improvements may have also occurred owing to James’ ability to initiate and re-initiate sleep independently (i.e., there was improved stimulus control for sleep). Although the frequency of NWs reduced, the duration of NWs did not. When James woke, he tended to remain awake for an hour or more, and to vocalize during this time. The absence of NWs particularly at follow-up concomitantly resulted in the elimination of vocal stereotypy; that is, it appears vocal stereotypy reduced owing to a lack of opportunity to perform the behavior, because he was no longer waking at night.
Discussion
This study drew upon the perspectives of parents of children on the autism spectrum with sleep problems, to increase our understanding of the types and topography of sleep-related stereotypic behavior, how parents are managing stereotypic behaviors in the sleep context, and the potential role of stereotypy in relation to sleep disturbance. Parents reported their children exhibiting a wide range of stereotypic behaviors at night, broadly including motor and vocal behaviors, and to a lesser extent RMO. This finding is unsurprising, as it is widely accepted that stereotypy presents heterogeneously across and within individuals (Cunningham & Schreibman, 2008; Rapp & Vollmer, 2005); however, it does underscore extant research (e.g., Hunter et al., 2021; Jin et al., 2013; McLay et al., 2019, 2021a) suggesting children on the autism spectrum can engage in a wide variety of repetitive behaviors both at the start of and/or during the night. Future research is needed to better understand the types of stereotypy children engage in at night, including characterizing the topography, severity (e.g., frequency, duration), prevalence, and patterns (e.g., temporal occurrence) of behavior, which ultimately will help practitioners to align treatment to the individual needs of children on the autism spectrum. The relationship between day- and night-time stereotypy also requires further investigation, including the extent to which behaviors may differ, and whether treating daytime stereotypy reduces the occurrence of stereotypy at night, and vice versa.
Parent responses to children’s sleep-related stereotypy varied in intensity, from no response, to co-sleeping. That some parents employ co-sleeping (i.e., a response that was undesired by the parents) as an intentional attempt to manage sleep problems including stereotypy, particularly motor stereotypy, suggests parents may struggle to overcome these behaviors alone, and require specialist support. Although the impact of parent response on behavior was not able to be established, this also raises important questions regarding the behavioral function of children’s stereotypy. Notably, given that children are typically alone when they engage in stereotypy (i.e., in their bedroom), it is likely that stereotypy frequently functions to produce automatic reinforcement. That parents tend to ignore stereotypy may be a product of their response having little to no impact on automatically reinforced behavior. The extent to which stereotypy serves other or additional functions in the sleep context, however, requires further investigation. In many cases in this study, children’s stereotypy eventually resulted in parental attention, including co-sleeping; the possibility that stereotypy is socially mediated, even partially, cannot be ruled out. It is also feasible that escalations in children’s behavior are reinforced by parents consistently responding to stereotypy at heightened levels. Furthermore, stereotypy may operate as a form of escape (i.e., negative reinforcement), for example, from the demand to go to sleep or mitigating physical discomfort. Careful consideration of the possible motivating consequences for stereotypy is important, to inform function-based treatment (Cunningham & Schreibman, 2008; Jin et al., 2013; McLay et al., 2019). Specifically, as was reported by parents and further illustrated in this case study, if behavior is multiply determined, it may be necessary to eliminate external motivators for behavior (e.g., parent attention), as well as addressing underlying automatic sensory consequences (Cunningham & Schreibman, 2008; Gwyther et al., 2017; Jin et al., 2013; McLay et al., 2019).
The distinction between sleep-interfering and sleep-conducive stereotypy was an interesting finding, which underscores the importance in utilizing FBA to inform individualized case conceptualizations and treatment plans, and holds pragmatic value for treatment. In a majority of children, stereotypy, particularly vocalizations, were conceptualized as sleep-interfering; however, this was not reported to be the case for all children. This raises questions about whether stereotypy may differentially affect sleep onset across and within children and is an important consideration in clinical assessment and treatment, and an interesting avenue for further research. Sleep-interfering stereotypy might be considered a form of stimulation or “play” that directly competes with behavioral quietude, and thus inhibits the onset of sleep. In such instances, the underlying issue may be motivational, in that the reinforcer of stereotypy is more salient, immediate, and desirable than the delayed reinforcer of sleep (Blampied & Bootzin, 2013; Blampied & France, 1993; Rapp et al., 2017). Accordingly, treatment focus would be on the reduction of sleep-interfering behavior to allow opportunity for behavioral quietude to occur, and strategies that increase motivation for sleep (e.g., through sleep restriction or faded bedtime procedures; Hunter et al., 2021; Jin et al., 2013; McLay et al., 2021a; Piazza & Fisher, 1991). In this case study, sleep restriction in combination with white noise, visual aids, and the removal of social attention appears to have reduced NWs and concurrently vocal stereotypy, although it is not possible to determine which treatment components (or combination of components) were effective. Stereotypy can be difficult to treat owing to the challenges inherent in interrupting automatic reinforcement contingencies that are not accessible to external control; in the case of vocal stereotypy, for example, the reinforcer is concomitant with the behavior itself and highly immediate (Akers et al., 2020; Boyd et al., 2012; Lanovaz & Sladeczek, 2012; Rapp & Vollmer, 2005). Procedures that increase motivation to initiate and maintain sleep, in effect removing the opportunity for engagement in sleep-interfering behaviors, may be a particularly useful means to treat stereotypic behavior that is otherwise hard to manipulate (Hunter et al., 2021).
In this case study, white noise had no effect on target sleep variables including vocal stereotypy. This is unsurprising given that James’ sleep problems were hypothesized to be multiply determined and therefore required multiple, function-based treatment components to sufficiently address the variables maintaining his sleep problems (McLay et al., 2021a). The lack of effect on stereotypy is more interesting, however, given the evidence that matched stimulation can effectively reduce vocal stereotypy in individuals on the autism spectrum (DiGennaro Reed et al., 2012; Lanovaz et al., 2011; Saylor et al., 2012; Wang et al., 2020). There are several reasons why white noise may have had no effect in this study, including that satiation did not occur, or that vocal stereotypy was reinforced by consequences other than, or in addition to, auditory stimulation (e.g., the tactile sensation of throat vibrations, or the content of vocalizations relating to an enjoyable memory). One of the core challenges in treating automatically reinforced behavior is that it may be impractical or impossible to identify and truly eliminate all possible specific reinforcers maintaining behavior (Shore et al., 1997). In addition, studies suggest that preferred forms of matched stimulation are more effective than non-preferred stimulation (Lanovaz et al., 2012; Wang et al., 2020); for example, Saylor et al. (2012) compared the effects of three types of noncontingent auditory stimulation (white noise, music and recordings of vocal stereotypy) on vocal stereotypy in two children on the autism spectrum. Results showed that music, which was the most preferred treatment selected by both children, reduced vocalizations most effectively for each child. In this case study, white noise was selected because it was expected to be less sleep-disruptive than music, however, future research could help to determine whether matched but also preferred auditory stimulation may help to decrease sleep-related stereotypy in children on the autism spectrum. Although the impact of stereotypy on sleep in this study remains unclear, these results highlight the reciprocal nature of the relationship between sleep disturbance and stereotypy, in that sleep disturbance may increase stereotypy but increased stereotypy may also interfere with sleep (Adams et al., 2014; Hollway & Aman, 2011). In this case study, NWs precipitated vocal stereotypy, and in return, vocal stereotypy may have perpetuated NWs.
In contrast to sleep-interfering stereotypy, it is possible that sleep-conducive stereotypy represents a learned type of self-settling behavior in some children, perhaps similar to RM in infants and young children (Haywood & Hill, 2012; Hoban, 2003). If sleep-conducive stereotypy is a learned variety of self-settling, a greater treatment emphasis may need to be placed on teaching replacement skills (e.g., relaxation leading to behavioral quietude), so the child is taught more adaptive, efficient means to initiate sleep. The distinction between sleep-interfering and sleep-conducive stereotypy requires further investigation, including whether such a distinction exists, and how varying types of stereotypy fit within these categories (e.g., if vocalizations are primarily interfering). Furthermore, the mechanisms underlying the stereotypy and sleep relationship warrant further attention; for example, motor stereotypy may serve to modulate anxiety in some children on the autism spectrum (Russell et al., 2019); anxiety is prevalent in individuals on the autism spectrum (Adams et al., 2019) and may contribute to sleep disturbance (Mazurek & Petroski, 2015; Richdale & Baglin, 2015). It is noteworthy that when considering whether sleep-related stereotypy is problematic, it is the relationship of the behavior to sleep onset that is important (Gwyther et al., 2017); sleep-conducive stereotypy may still warrant targeted treatment if a child’s ability to settle and/or re-settle to sleep efficiently is impaired through perseverance with repetitive behavior.
The degree of overlap between sleep-related motor stereotypy as identified in this study and rhythmic movement disorder (RMD; a form of parasomnia) is unclear (Veatch et al., 2015). There may be a high degree of correspondence, given RMD is defined by stereotyped and rhythmic movements often involving large muscle groups (e.g., body-rocking, head-rolling), that occur in association with sleep (often during the wake-sleep transition), and which can impair sleep by delaying sleep onset (Gwyther et al., 2017; Haywood & Hill, 2012; Veatch et al., 2015). As a parasomnia, rhythmic movements in RMD can also occur during sustained sleep, and disrupt sleep quality (Gwyther et al., 2017; Haywood & Hill, 2012; Hoban, 2003). Diagnosis of RMD is typically based on parent report (Gwyther et al., 2017). The degree of overlap between stereotypic and RM behaviors requires further investigation; for example, it is unclear whether the child in this study who engaged in a standing-rock until she “dropped” into sleep would constitute an extreme variety of RMD. Notably, there is insufficient information regarding RMD in populations outside of children with typical development (Gwyther et al., 2017) to understand its overlay with autism-related stereotypy. Interestingly, persistent RMD (i.e., beyond 5 years of age) has been associated with developmental disorders, particularly ADHD, but also autism (Gwyther et al., 2017; Hoban, 2003; Johnson et al., 2009; Stepanova et al., 2005).
Conversely, motor stereotypy, although strongly associated with autism, is not exclusive to autism and occurs in children with typical development, particularly during early childhood (Goldman et al., 2009; Singer, 2009). This raises important questions regarding how repetitive behaviors are classified and understood in autism, for example, whether RMD and sleep-related motor stereotypy are a similar or entirely different phenomenon, of shared or distinct etiology. It also highlights the complexity and multiplicity of sleep problems that children on the autism spectrum can experience; for example, sleep-related repetitive behaviors may be linked to insomnia (e.g., SOD/NWs), parasomnia (e.g., RMD), or both. For example, in a study by Weiskop et al. (2005), one participant child on the autism spectrum exhibited stereotypic rocking during NWs. Weiskop et al. (2005) reported that it was unable to be determined whether the night-time rocking was a form of automatically reinforced stereotypy or occurred whilst the child was asleep and was thus a form of parasomnia. Other sleep-related movement disorders are also relevant to autism, such as restless leg syndrome involving repetitive movement of the legs, or larger muscle groups (e.g., body-rocking) involving the legs, during the wake-sleep transition (Kanney et al., 2020; Veatch et al., 2015). Restless leg syndrome is often associated with periodic limb movements in sleep, involving repetitive movements of extremities during sleep (Veatch et al., 2015). Understanding the distinction between repetitive movements in relation to sleep disturbance is important to knowing how to treat such behavior (Veatch et al., 2015; Weiskop et al., 2005). It is necessary to determine whether a child is awake and there are operant qualities to repetitive behavior when evaluating sleep problems for behavioral treatment.
The findings of this research underscore the importance of determining parent’s views in relation to the assessment and treatment of children’s sleep problems. Parents are in a unique position to report on child behavior that occurs within the home environment; qualitative methods provide a means of exploring parent perceptions of child behavior, which can add insight and understanding of the complex nature of sleep problems in children on the autism spectrum (Kirkpatrick et al., 2019). Furthermore, parents’ sleep-related cognitions are an important consideration in treatment planning, not least because they inform parent’s own response to child behavior, which may be unintentionally reinforcing sleep problems (e.g., lying with a child in response to NWs; Hastings, 2002; Levin & Scher, 2016), and may inform parents’ help-seeking behavior (McLay et al., 2020). For example, parents who view their child’s behavior as beneficial to the child (e.g., stereotypy as soothing) may be less likely to seek or be willing to engage with treatment aimed at reducing the behavior. In this case study, parent perception of stereotypy as problematic (i.e., sleep-interfering) informed (at least partially) parent response (e.g., co-sleeping) and treatment goals to reduce the behavior. The sleep context also poses unique challenges for the treatment of sleep-related stereotypy, including that parents must act (where possible) as primary interventionists within their own home (Hanley et al., 2014; Jin et al., 2013). It is important, therefore, that sleep problems are assessed and addressed in collaboration with parents (Jin et al., 2013; Moes & Frea, 2002; Pattison et al., 2020), and that treatment includes parent education, training, and up-skilling, to help parents to manage sleep-related behaviors within their own home (Boyd et al., 2012; Haywood & Hill, 2012; Lanovaz et al., 2016; Specht et al., 2017).
Limitations and Future Research
Several limitations may limit confidence in the overall reliability of results. First, this study focused on children who were referred for sleep intervention services and whose parents reported engagement in sleep-related stereotypy. Results are therefore representative of a subset of children on the autism spectrum experiencing clinically significant sleep disturbance and stereotypy and may not accurately reflect the wider population. Second, stereotypy data were obtained using semi-structured interviewing within the context of a clinical assessment. This enabled the researchers to ensure consistency in how core information was elicited across parents, whilst allowing parents to share individualized experiences with depth (Belotto, 2018). However, given the purpose of the interview (i.e., to clinically assess children’s sleep problems), the types of questions asked may have influenced the types of responses provided by parents (e.g., questions about stereotypy were asked in relation to known sleep problems). Furthermore, thematic analysis was conducted by coding clinical assessment reports; thus, prior to coding, data were limited to that which were clinically relevant and may have excluded information pertinent to this topic. Finally, the same author primarily conducted the interviews and led the data analysis; whilst steps were taken to mitigate risk of bias (i.e., interrater reliability), the results may not be entirely free of interactions and influences of the author’s own values and biases. Thus, the findings of this study are tentative and are presented for the purpose of stimulating future research.
Future research could clarify and strengthen the results of this study by examining parent perspectives of sleep-related stereotypy in children on the autism spectrum using a broader interview framework to transcribe, code, and analyze parents’ verbatim responses. This is likely to generate fuller, unconstrained data sets for analysis. The incorporation of instrumented sleep measures (e.g., VSG) into assessment would help to triangulate parent-report and broaden insight into children’s stereotypic sleep-related behavior, including behavior which parents may be unaware of and therefore unable to report on. For example, it is possible that children engaged in a wider range of stereotypy, with differing implications for sleep, than what was identified in this research. Ideally, this should include assessment of vocalizations, as a limitation of this case study was the inability of VSG to capture audio, which meant IOA of vocal stereotypy was not possible. It is important that future research specifically investigate whether a reduction in sleep-related stereotypy decreases SOD and/or the duration of NWs. Based on the findings of this analysis, it may be hypothesized that reducing sleep-related stereotypy (particularly vocal stereotypy) decreases SOD and/or the duration of NWs, which would suggest that stereotypy interferes with sleep onset. Finally, future research should explore whether children on the autism spectrum without sleep problems engage in stereotypy in the sleep context and how this may differ to sleep-interfering stereotypic behavior. It may be hypothesized that the severity (e.g., frequency, duration), prevalence, and patterns (e.g., temporal occurrence) of behavior differ in accordance with varying severity of sleep problems (e.g., no sleep problems, mild-moderate, and severe sleep disturbance). For example, in children who sleep well, stereotypy may be limited to the initial sleep onset period (in the absence of NWs) and occur briefly, such that perseverance with repetitive behavior does not disrupt sleep. Such research would enhance our understanding of the sleep-stereotypy nexus; for example, it is possible that sleep-related stereotypy commonly occurs in children on the autism spectrum, but may not be considered problematic, detected and/or reported by parents.
References
Abel, E. A., Schwichtenberg, A. J., Brodhead, M. T., & Christ, S. L. (2018). Sleep and challenging behaviors in the context of intensive behavioral intervention for children with autism. Journal of Autism and Developmental Disorders, 48, 3871–3884. https://doi.org/10.1007/s10803-018-3648-0
Accardo, J. A., & Malow, B. A. (2015). Sleep, epilepsy, and autism. Epilepsy and Behavior, 47, 202–206. https://doi.org/10.1016/j.yebeh.2014.09.081
Adams, H. L., Matson, J. L., Cervantes, P. E., & Goldin, R. L. (2014). The relationship between autism symptom severity and sleep problems: Should bidirectionality be considered? Research in Autism Spectrum Disorders, 8(3), 193–199. https://doi.org/10.1016/j.rasd.2013.11.008
Adams, D., Young, K., & Keen, D. (2019). Anxiety in children with autism at school: A systematic review. Review Journal of Autism and Developmental Disorders, 6, 274–288. https://doi.org/10.1007/s40489-019-00172-z
Ahearn, W. H., Clark, K. M., MacDonald, R. P., & Chung, B. I. (2007). Assessing and treating vocal stereotypy in children with autism. Journal of Applied Behavior Analysis, 40(2), 263–275. https://doi.org/10.1901/jaba.2007.30-06
Akers, J. S., Davis, T. N., Gerow, S., & Avery, S. (2020). Decreasing motor stereotypy in individuals with autism spectrum disorder: A systematic review. Research in Autism Spectrum Disorders, 77, 101611. https://doi.org/10.1016/j.rasd.2020.101611
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
Bangerter, A., Chatterjee, M., Manyakov, N. V., Ness, S., Lewin, D., Skalkin, A., Boice, M., Goodwin, M. S., Dawson, G., Hendren, R., Leventhal, B., Shic, F., Ebensen, A., & Pandina, G. (2020). Relationship between sleep and behavior in autism spectrum disorder: Exploring the impact of sleep variability. Frontiers in Neuroscience, 24(14), 211. https://doi.org/10.3389/fnins.2020.00211
Belotto, M. J. (2018). Data analysis methods for qualitative research: Managing the challenges of coding, interrater reliability, and thematic analysis. The Qualitative Report, 23(11), 2622–2633. https://doi.org/10.46743/2160-3715/2018.3492
Beresford, B., Stuttard, L., Clarke, S., & Maddison, J. (2016). Parents’ experiences of psychoeducational sleep management interventions: A qualitative study of parents of children with neurodevelopmental disabilities. Clinical Practice in Pediatric Psychology, 4, 164–175. https://doi.org/10.1037/cpp0000144
Blampied, N. M. (2013). Functional behavioral analysis of sleep in infants and children. In A. R. Wolfson & H. E. Montgomery-Downs (Eds.), The Oxford handbook of infant, child, and adolescent sleep and behaviour (pp. 169–188). Oxford University Press.
Blampied, N. M., & Bootzin, R. R. (2013). Sleep: A behavioral account. In G. J. Madden, W. V. Dube, T. D. Hackenberg, G. P. Hanley, & K. A. Lattal (Eds.), APA handbook of applied behavior analysis: Translating principles into practice (Vol. 2, pp. 425–454). American Psychological Association.
Blampied, N. M., & France, K. G. (1993). A behavioral model of infant sleep disturbance. Journal of Applied Behavior Analysis, 26, 477–492. https://doi.org/10.1901/jaba.1993.26-477
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30, 237–243. https://doi.org/10.1023/A:1005596502855
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Boyd, B. A., McDonough, S. G., & Bodfish, J. W. (2012). Evidence-based behavioral interventions for repetitive behaviors in autism. Journal of Autism and Developmental Disorders, 42(6), 1236–1248. https://doi.org/10.1007/s10803-011-1284-z
Chu, J., & Richdale, A. L. (2009). Sleep quality and psychological wellbeing in mothers of children with developmental disabilities. Research in Developmental Disabilities, 30(6), 1512–1522. https://doi.org/10.1016/j.ridd.2009.07.007
Cohen, S., Conduit, R., Lockley, S. W., Rajaratnam, S. M. W., & Cornish, K. M. (2014). The relationship between sleep and behavior in autism spectrum disorder (ASD): A review. Journal of Neurodevelopmental Disorders, 6(44), 2–10. https://doi.org/10.1186/1866-1955-6-44
Cohen, S., Fulcher, B. D., Rajaratnam, S. M. W., Conduit, R., Sullivan, J. P., St Hilaire, M. A., Phillips, A. J. K., Loddenkemper, T., Kothare, S. V., McConnell, K., Braga-Kenyon, P., Ahearn, W., Shlesinger, A., Potter, J., Bird, F., Cornish, K. M., & Lockley, S. W. (2018). Sleep patterns predictive of daytime challenging behavior in individuals with low-functioning autism. Autism Research, 11(2), 391–403. https://doi.org/10.1002/aur.1899
Cortesi, F., Giannotti, F., Ivanenko, A., & Johnson, K. (2010). Sleep in children with autistic spectrum disorder. Sleep Medicine, 11(7), 659–664. https://doi.org/10.1016/j.sleep.2010.01.010
Cunningham, A. B., & Schreibman, L. (2008). Stereotypy in autism: The importance of function. Research in Autism Spectrum Disorders, 2(3), 469–479. https://doi.org/10.1016/j.rasd.2007.09.006
Delahaye, J., Kovacs, E., Sikora, D., Hall, T. A., Orlich, F., Clemons, T. E., van der Weerd, E., Glick, L., & Kuhlthau, K. (2014). The relationship between health-related quality of life and sleep problems in children with autism spectrum disorder. Research in Autism Spectrum Disorders, 8(3), 292–303. https://doi.org/10.1016/j.rasd.2013.12.015
Didden, R., Sturmey, P., Sigafoos, J., Lang, R., O’Reilly, M. F., & Lancioni, G. E. (2012). Nature, prevalence, and characteristics of challenging behavior. In J. L. Matson (Ed.), Functional assessment for challenging behaviors (pp. 25–44). Springer New York.
DiGennaro Reed, F. D., Hirst, J. M., & Hyman, S. R. (2012). Assessment and treatment of stereotypic behavior in children with autism and other developmental disabilities: A thirty year review. Research in Autism Spectrum Disorders, 6(1), 422–430. https://doi.org/10.1016/j.rasd.2011.07.003
Durand, V. M., & Carr, E. G. (1987). Social influences on “self-stimulatory” behavior: Analysis and treatment application. Journal of Applied Behavior Analysis, 20(2), 119–132. https://doi.org/10.1901/jaba.1987.20-119
Elliott, V. (2018). Thinking about the Coding Process in Qualitative Data Analysis. The Qualitative Report, 23(11), 2850-2861. https://doi.org/10.46743/21603715/2018.356
France, K. G. (2011). Extinction with parental presence. In M. L. Perlis, M. Aloia, & B. Kuhn (Eds.), Behavioral treatments for sleep disorders: a comprehensive primer of behavioral sleep medicine interventions (pp. 275–283). Elsevier. https://doi.org/10.1016/B978-0-12-381522-4.00028-6
Gabriels, R. L., Agnew, J. A., Pan, Z., Holt, K. D., Reynolds, A., & Laudenslager, M. L. (2013). Elevated repetitive behaviors are associated with lower diurnal salivary cortisol levels in autism spectrum disorder. Biological Psychology, 93, 262–268. https://doi.org/10.1016/j.biopsycho.2013.02.017
Gabriels, R. L., Cuccaro, M. L., Hill, D. E., Ivers, B. J., & Goldson, E. (2005). Repetitive behaviors in autism: Relationships with associated clinical features. Research in Developmental Disabilities, 26(2), 169–181. https://doi.org/10.1016/j.ridd.2004.05.003
Goldman, S. E., Richdale, A. L., Clemons, T., & Malow, B. A. (2012). Parental sleep concerns in autism spectrum disorders: Variations from childhood to adolescence. Journal of Autism and Developmental Disorders, 42(4), 531–538. https://doi.org/10.1007/s10803-011-1270-5
Goldman, S., Wang, C., Salgado, M. W., Greene, P. E., Kim, M., & Rapin, I. (2009). Motor stereotypies in children with autism and other developmental disorders. Developmental Medicine and Child Neurology, 51(1), 30–38. https://doi.org/10.1111/j.1469-8749.2008.03178.x
Gray, C. A., & Garand, J. D. (1993). Social stories: Improving response of students with autism with accurate social information. Focus on Autistic Behavior, 8, 1–10. https://doi.org/10.1177/108835769300800101
Gwyther, A. R. M., Walters, A. S., & Hill, C. M. (2017). Rhythmic movement disorder in childhood: An integrative review. Sleep Medicine Reviews, 35, 62–75. https://doi.org/10.1016/j.smrv.2016.08.003
Hanley, G. P. (2005). Sleep Assessment and Treatment Tool [Measurement Instrument]. Retrieved May 26, 2017, from https://practicalfunctionalassessment.files.wordpress.com/2015/06/satt.pdf
Hanley, G. P., Jin, S. C., Vanselow, N. R., & Hanratty, L. A. (2014). Producing meaningful improvements in problem behavior of children with autism via synthesized analyses and treatments. Journal of Applied Behavior Analysis, 47(1), 16–36. https://doi.org/10.1002/jaba.106
Hastings, R. P. (2002). Parental stress and behavioural problems of children with developmental disability. Journal of Intellectual and Developmental Disability, 27(3), 149–160. https://doi.org/10.1080/1366825021000008657
Haywood, P. M., & Hill, C. M. (2012). Rhythmic movement disorder: Managing the child who head-bangs to get to sleep. Pediatrics and Child Health, 22(5), 207–2010. https://doi.org/10.1016/j.paed.2012.02.010
Hirshkowitz, M., Whiton, K., Albert, S. M., Alessi, C., Bruni, O., DonCarlos, L., Hazen, N., Herman, J., Katz, E. S., Kheirandish-Gozal, L., Neubauer, D. N., O’Donnell, A. E., Ohayon, M., Peever, J., Rawding, R., Sachdeva, R. C., Setters, B., Vitiello, M. V., Ware, C., & Adams Hillard, P. J. (2015). National Sleep Foundation’s updated sleep duration recommendations. Sleep Health, 1, 233–243. https://doi.org/10.1016/j.sleh.2015.10.004
Hoban, T. F. (2003). Rhythmic movement disorder in children. CNS Spectrum, 8(2), 135–138. https://doi.org/10.1017/s1092852900018368
Hollway, J. A., & Aman, M. G. (2011). Sleep correlates of pervasive developmental disorders: A review of the literature. Research in Developmental Disabilities, 32(5), 1399–1421. https://doi.org/10.1016/j.ridd.2011.04.001
Hundley, R. J., Shui, A., & Malow, B. A. (2016). Relationship between subtypes of restricted and repetitive behaviors and sleep disturbance in autism spectrum disorder. Journal of Autism and Developmental Disorders, 46, 3448–3457. https://doi.org/10.1007/s10803-016-2884-4
Hunter, J. E., McLay, L. K., France, K. G., & Blampied, N. M. (2021). Sleep and stereotypy in children with autism: Effectiveness of function-based behavioral treatment. Sleep Medicine, 80, 301–304. https://doi.org/10.1016/j.sleep.2021.01.062
Hunter, J. E., McLay, L. K., France, K. G., & Blampied, N. M. (2020). Systematic review of the collateral effects of behavioral sleep interventions in children and adolescents with autism spectrum disorder. Research in Autism Spectrum Disorders, 79, 101677. https://doi.org/10.1016/j.rasd.2020.101677
Jin, C. S., Hanley, G. P., & Beaulieu, L. (2013). An individualised and comprehensive approach to treating sleep problems in young children. Journal of Applied Behavior Analysis, 46(1), 161–180. https://doi.org/10.1002/jaba.16
Johnson, C. R., Smith, T., DeMand, A., Lecavalier, L., Evans, V., Gurka, M., Swiezy, N., Bearss, K., & Scahill, L. (2018). Exploring sleep quality of young children with autism spectrum disorder and disruptive behaviors. Sleep Medicine, 44, 61–66. https://doi.org/10.1016/j.sleep.2018.01.008
Johnson, K. P., Giannotti, F., & Cortesi, F. (2009). Sleep patterns in autism spectrum disorders. Child and Adolescent Psychiatric Clinics of North America, 18(4), 917–928. https://doi.org/10.1016/j.chc.2009.04.001
Kanney, M. L., Durmer, J. S., Trotti, L. M., & Leu, R. (2020). Rethinking bedtime resistance in children with autism: is restless leg syndrome to blame? Journal of Clinical Sleep Medicine, 16(12), https://doi.org/10.5664/jcsm.8756
Kazdin, A. E. (1984). Acceptability of aversive procedures and medication as treatment alternatives for deviant child behavior. Journal of Abnormal Child Psychology, 12, 289–301. https://doi.org/10.1007/BF00910669
Kennedy, C. H., Meyer, K. A., Knowles, T., & Shukla, S. (2000). Analyzing the multiple functions of stereotypical behavior for students with autism: Implications for assessment and treatment. Journal of Applied Behavior Analysis, 33(4), 559–571. https://doi.org/10.1901/jaba.2000.33-559
Kirkpatrick, B., Gilroy, S. P., & Leader, G. (2019). Qualitative study on parents’ perspectives of the familial impact of living with a child with autism spectrum disorder who experiences insomnia. Sleep Medicine, 62, 59–68. https://doi.org/10.1016/j.sleep.2019.01.032
Knight, R. M., & Johnson, C. M. (2014). Using a behavioral treatment package for sleep problems in children with autism spectrum disorders. Child and Family Behavior Therapy, 36(3), 204–221. https://doi.org/10.1080/07317107.2014.934171
Lanovaz, M. J., Rapp, J. T., Maciw, I., Dorion, C., & Prégent-Pelletier, É. (2016). Preliminary effects of parent-implemented behavioural interventions for stereotypy. Developmental Neurorehabilitation, 19(3), 193–196. https://doi.org/10.3109/17518423.2014.986821
Lanovaz, M. J., & Sladeczek, I. E. (2012). Vocal stereotypy in individuals with autism spectrum disorders: A review of behavioral interventions. Behavior Modification, 36(2), 146–164. https://doi.org/10.1177/0145445511427192
Lanovaz, M. J., Sladeczek, I. E., & Rapp, J. T. (2011). Effects of music on vocal stereotypy in children with autism. Journal of Applied Behavior Analysis, 44(3), 647–651. https://doi.org/10.1901/jaba.2011.44-647
Lanovaz, M. J., Sladeczek, I. E., & Rapp, J. T. (2012). Effects of noncontingent music on vocal stereotypy and toy manipulation in children with autism spectrum disorders. Behavioral Interventions, 27, 207–223. https://doi.org/10.1002/bin
Leader, G., & Mannion, A. (2016). Gastrointestinal disorders. In Matson J. (eds) Comorbid conditions among children with autism spectrum disorders. Autism and Child Psychopathology Series (pp. 257–281). Springer, Cham. https://doi.org/10.1007/978-3-319-19183-6_11
Levin, A., & Scher, A. (2016). Sleep problems in young children with autism spectrum disorders: A study of parenting stress, mothers’ sleep-related cognitions, and bedtime behaviors. CNS Neuroscience and Therapeutics, 22(11), 921–927. https://doi.org/10.1111/cns.12651
Lydon, S., Moran, L., Healy, O., Mulhern, T., & Enright Young, K. (2017). A systematic review and evaluation of inhibitory stimulus control procedures as a treatment for stereotyped behavior among individuals with autism. Developmental Neurorehabilitation, 20(8), 491–501. https://doi.org/10.1080/17518423.2016.1265604
Malow, B. A., Marzec, M. L., McGrew, S. G., Wang, L., Henderson, L. M., & Stone, W. L. (2006). Characterizing sleep in children with autism spectrum disorders: A multidimensional approach. Sleep, 29(12), 1563–1571. https://doi.org/10.1093/sleep/29.12.1563
Martin, C. A., Papadopoulos, N., Chellew, T., Rinehart, N. J., & Sciberras, E. (2019). Associations between parenting stress, parent mental health and child sleep problems for children with ADHD and ASD: Systematic review. Research in Developmental Disabilities, 93, 1–15. https://doi.org/10.1016/j.ridd.2019.103463
Mazurek, M. O., Dovgan, K., Neumeyer, A. M., & Malow, B. A. (2019). Course and predictors of sleep and co-occurring problems in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 49, 2101–2115. https://doi.org/10.1007/s10803-019-03894-5
Mazurek, M. O., & Petroski, G. F. (2015). Sleep problems in children with autism spectrum disorder: Examining the contributions of sensory-over-responsivity and anxiety. Sleep Medicine, 16(2), 270–279. https://doi.org/10.1016/j.sleep.2014.11.006
Mazzone, L., Postorino, V., Siracusano, M., Riccioni, A., & Curatolo, P. (2018). The relationship between sleep problems, neurobiological alterations, core symptoms of autism spectrum disorder, and psychiatric comorbidities. Journal of Clinical Medicine, 7(5), E102. https://doi.org/10.3390/jcm7050102
McCarty, M. J., & Brumback, A. C. (2021). Rethinking stereotypies in autism. Seminars in Pediatric Neurology, 38, 100897. https://doi.org/10.1016/j.spen.2021.100897
McLay, L., France, K., Blampied, N., & Hunter, J. (2019). Using functional behavioral assessment to treat sleep problems in two children with autism and vocal stereotypy. International Journal of Developmental Disabilities, 65(3), 175–184. https://doi.org/10.1080/20473869.2017.1376411
McLay, L., France, K., Blampied, N., van Deurs, J., Hunter, J., Knight, J., Hastie, B., Carnett, A., Woodford, E., Gibbs, R., & Lang, R. (2021a). Function-based behavioral interventions for sleep problems in children and adolescents with autism: Summary of 41 clinical cases. Journal of Autism and Developmental Disorders, 51, 418–432. https://doi.org/10.1007/s10803-020-04548-7
McLay, L., Hansen, S. G., Carnett, A., France, K. G., & Blampied, N. M. (2020). Attributions, causal beliefs, and help-seeking behavior of parents of children with autism spectrum disorder and sleep problems. Autism, 24(7), 1829–1840. https://doi.org/10.1177/1362361320924216
McLay, L. L., France, K. G., Blampied, N. M., Hunter, J. E., van Deurs, J. R., Woodford, E. C., Gibbs, R., & Lang, R. (2021b). Collateral child and parent effects of function-based behavioral interventions for sleep problems in children and adolescents with autism. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-021-05116-3
Meltzer, L. J. (2011). Factors associated with depressive symptoms in parents of children with autism spectrum disorders. Research in Autism Spectrum Disorders, 5(1), 361–367. https://doi.org/10.1016/j.rasd.2010.05.001
Michael, J. (1982). Distinguishing between discriminative and motivational functions of stimuli. Journal of Experimental Analysis of Behavior, 37, 149–155. https://doi.org/10.1901/jeab.1982.37-149
Moes, D. R., & Frea, W. D. (2002). Contextualized behavioral support in early intervention for children with autism and their families. Journal of Autism and Developmental Disorders, 32(6), 519–533. https://doi.org/10.1023/A:1021298729297
O’Connor, C., & Joffe, H. (2020). Intercoder reliability in qualitative research: Debates and practical guidelines. International Journal of Qualitative Methods, 19, 1–13. https://doi.org/10.1177/1609406919899220
Owens, J. A., Spirito, A., & McGuinn, M. (2000). The children’s sleep habits questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep, 23(8), 1–9.
Park, S., Cho, S.-C., Cho, I. H., Kim, B.-N., Kim, J.-W., Shin, M.-S., Chung, U.-S., Park, T.-W., Son, J.-W., & Yoo, H. J. (2012). Sleep problems and their correlates and comorbid psychopathology of children with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(3), 1068–1072. https://doi.org/10.1016/j.rasd.2012.02.004
Pattison, E., Papadopoulos, N., Marks, D., McGillivray, J., & Rinehart, N. (2020). Behavioural treatments for sleep problems in children with autism spectrum disorder: A review of recent literature. Current Psychiatry Reports, 22, 46. https://doi.org/10.1007/s11920-020-01172-1
Piazza, C. C., & Fisher, W. W. (1991). A faded bedtime with response cost protocol for treatment of multiple sleep problems in children. Journal of Applied Behavior Analysis, 24, 129–140. https://doi.org/10.1901/jaba.1991.24-129
Rapp, J. T., Cook, J. L., McHugh, C., & Mann, K. R. (2017). Decreasing stereotypy using NCR and DRO with functionally matched stimulation: Effects on targeted and non-targeted stereotypy. Behavior Modification, 41(1), 45–83. https://doi.org/10.1177/0145445516652370
Rapp, J. T., & Lanovaz, M. J. (2016). Stereotypy. In N. N. Singh (Ed.), Clinical handbook of evidence-based practices for individuals with intellectual and developmental disabilities (pp. 751–780). Springer, Cham. https://doi.org/10.1007/978-3-319-26583-4_28
Rapp, J. T., & Vollmer, T. R. (2005). Stereotypy I: A review of behavioral assessment and treatment. Research in Developmental Disabilities, 26(6), 527–547. https://doi.org/10.1016/j.ridd.2004.11.005
Reidy, S. M., Smith, M. G., Rocha, S., & Basner, M. (2021). Noise as a sleep aid: A systematic review. Sleep Medicine Reviews, 55, 101385. https://doi.org/10.1016/j.smrv.2020.101385
Reynolds, A. M., & Malow, B. A. (2011). Sleep and autism spectrum disorders. Pediatric Clinics of North America, 58(3), 685–698. https://doi.org/10.1016/j.pcl.2011.03.009
Richdale, A. L., & Baglin, C. L. (2015). Self-report and caregiver-report of sleep and psychopathology in children with high-functioning autism spectrum disorder: A pilot study. Developmental Neurorehabilitation, 18, 272–279. https://doi.org/10.3109/17518423.2013.829534
Richdale, A. L., & Schreck, K. A. (2009). Sleep problems in autism spectrum disorders: Prevalence, nature, & possible biopsychosocial aetiologies. Sleep Medicine Reviews, 13(6), 403–411. https://doi.org/10.1016/j.smrv.2009.02.003
Roantree, C. F., & Kennedy, C. H. (2006). A paradoxical effect of presession attention on stereotypy: Antecedent attention as an establishing, not an abolishing, operation. Journal of Applied Behavior Analysis, 39(3), 381–384. https://doi.org/10.1901/jaba.2006.97-05
Russell, K. M., Frost, K. M., & Ingersoll, B. (2019). The relationship between subtypes of repetitive behaviors and anxiety in children with autism spectrum disorder. Research in Autism Spectrum Disorders, 62, 48–54. https://doi.org/10.1016/j.rasd.2019.03.006
Sanders, M. R., & Burke, K. (2014). The “hidden” technology of effective parent consultation: A guided participation model for promoting change in families. Journal of Child and Family Studies, 23, 1289–1297. https://doi.org/10.1007/s10826-013-9827-x
Saylor, S., Sidener, T. M., Reeve, S. A., Fetherston, A., & Progar, P. R. (2012). Effects of three types of noncontingent auditory stimulation on vocal stereotypy in children with autism. Journal of Applied Behavior Analysis, 45(1), 185–190. https://doi.org/10.1901/jaba.2012.45-185
Schreck, K. A., Mulick, J. A., & Smith, A. F. (2004). Sleep problems as possible predictors of intensified symptoms of autism. Research in Developmental Disabilities, 25(1), 57–66. https://doi.org/10.1016/j.ridd.2003.04.007
Schreck, K. A., & Richdale, A. L. (2020). Sleep problems, behavior, and psychopathology in autism: Inter-relationships across the lifespan. Current Opinion in Psychology, 34, 105–111. https://doi.org/10.1016/j.copsyc.2019.12.003
Shore, B. A., Iwata, B. A., DeLeon, I. G., Kahng, S. W., & Smith, R. G. (1997). An analysis of reinforcer substitutability using object manipulation and self-injury as competing responses. Journal of Applied Behavior Analysis, 30(1), 21–41. https://doi.org/10.1901/jaba.1997.30-21
Singer, H. S. (2009). Motor Stereotypies. Seminars in Pediatric Neurology, 16(2), 77–81. https://doi.org/10.1016/j.spen.2009.03.008
Singh, K., & Zimmerman, A. W. (2015). Sleep in autism spectrum disorder and attention deficit hyperactivity disorder. Seminars in Pediatric Neurology, 22(2), 113–125. https://doi.org/10.1016/j.spen.2015.03.006
Sivertsen, B., Posserud, M.-B., Gillberg, C., Lundervold, A. J., & Hysing, M. (2012). Sleep problems in children with autism spectrum problems: a longitudinal population-based study. Autism, 16(2), 139–150. https://doi.org/10.1177/1362361311404255
Specht, M. W., Mahone, E. M., Kline, T., Waranch, R., Brabson, L., Thompson, C. B., & Singer, H. S. (2017). Efficacy of parent-delivered behavioral therapy for primary complex motor stereotypies. Developmental Medicine & Child Neurology, 59(2), 168–173. https://doi.org/10.1111/dmcn.13164
Stepanova, I., Nevsimalova, S., & Hanusova, J. (2005). Rhythmic movement disorder in sleep persisting into childhood and adulthood. Sleep, 28(7), 851–857. https://doi.org/10.1093/sleep/28.7.851
Taylor, M. A., Schreck, K. A., & Mulick, J. A. (2012). Sleep disruption as a correlate to cognitive and adaptive behavior problems in autism spectrum disorders. Research in Developmental Disabilities, 33, 1408–1417. https://doi.org/10.1016/j.ridd.2012.03.013
Turner, K. S., & Johnson, C. R. (2013). Behavioral interventions to address sleep disturbances in children with autism spectrum disorders: A review. Topics in Early Childhood Special Education, 33(3), 144–152. https://doi.org/10.1177/0271121412446204
van Deurs, J. R., McLay, L. K., France, K. G., & Blampied, N. M. (2021). Sequential implementation of functional behavioural assessment informed treatment components for sleep disturbance in autism: A case study. Behavioral Sleep Medicine, 19(3), 333–351. https://doi.org/10.1080/15402002.2020.1758701
Veatch, O. J., Maxwell-Horn, A. C., & Malow, B. A. (2015). Sleep in autism spectrum disorders. Current Sleep Medicine Reports, 1, 131–140. https://doi.org/10.1007/s40675-015-0012-1
Veatch, O. J., Sutcliffe, J. S., Warren, Z. E., Keenan, B. T., Potter, M. H., & Malow, B. A. (2017). Shorter sleep duration is associated with social impairment and comorbidities in ASD. Autism Research, 10(7), 1221–1238. https://doi.org/10.1002/aur.1765
Wang, D., Mason, R. A., Lory, C., Kim, S. Y., David, M., & Guo, X. (2020). Vocal stereotypy and autism spectrum disorder: A systematic review of interventions. Research in Autism Spectrum Disorders, 78, 101647. https://doi.org/10.1016/j.rasd.2020.101647
Weiskop, S., Richdale, A., & Matthews, J. (2005). Behavioural treatment to reduce sleep problems in children with autism or fragile X syndrome. Developmental Medicine and Child Neurology, 47(2), 94–104. https://doi.org/10.1017/S0012162205000186
Wilke, A. E., Tarbox, J., Dixon, D. R., Kenzer, A. L., Bishop, M. R., & Kakavand, H. (2012). Indirect functional assessment of stereotypy in children with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(2), 824–828. https://doi.org/10.1016/j.rasd.2011.11.003
Zuckerman, K. E., Hill, A. P., Guion, K., Voltolina, L., & Fombonne, E. (2014). Overweight and obesity: Prevalence and correlates in a large clinical sample of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 1708–1719. https://doi.org/10.1007/s10803-014-2050-9
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
JH: conceptualization, methodology, formal analysis, investigation, writing (original draft), writing—review and editing. LM: conceptualization, methodology, validation, writing (review and editing), supervision, project administration. KF: conceptualization, methodology, writing (review and editing), supervision, project administration. CS: methodology, formal analysis, validation, writing—review and editing). NB: conceptualization, methodology, formal analysis, writing (review and editing), visualization, supervision.
Corresponding author
Ethics declarations
Ethics Approval
This research was approved by the University of Canterbury Human Ethics Committee. Informed consent to use data for research purposes was attained from each child’s parent(s) and informed consent or assent was obtained from child participants as appropriate.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hunter, J.E., McLay, L.K., France, K.G. et al. Parent Perceptions of Sleep-Related Stereotypy Within Sleep Problems in Children on the Autism Spectrum: Implications for Behavioral Treatment. Adv Neurodev Disord 6, 456–472 (2022). https://doi.org/10.1007/s41252-022-00246-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-022-00246-w