
Abstract
Objective
Our objective was to assess the relationship between antihypertensive drugs, loop diuretics, and the risk of hospitalization for hip fracture (HF).
Design
We conducted a population-based study in a cohort of 81,617 patients from Lombardy (Italy) aged 70–90 years who were newly treated with antihypertensive agents or loop diuretics between 2005 and 2009. Cases were the 2153 patients who experienced the outcome (hospitalization for HF before 31 December 2012). For each case, up to three controls were randomly selected from the cohort to be matched for sex, age at cohort entry, and date of initial prescription. The case–control and case-crossover designs and the logistic regression for matched sets were used to measure the strength of the association between current use of an antihypertensive drug (within 30 days before the HF hospitalization) and the risk of outcome.
Results
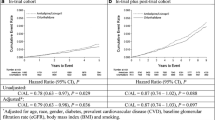
Case–control and case-crossover odds ratios (ORs) for current use of loop diuretics were 1.67 (95 % confidence interval [CI] 1.28–2.18) and 1.49 (95 % CI 1.05–2.10), respectively. Among patients aged 81–90 years, case–control and case-crossover ORs were 1.52 (95 % CI 1.04–2.21) and 1.82 (95 % CI 1.10–3.00) for current use of loop diuretics and 1.86 (95 % CI 1.03–3.35) and 1.88 (95 % CI 1.01–3.48) for α-blockers. No other agent was associated with the outcome.
Conclusions
Evidence that loop diuretics and α-blockers are associated with a higher risk of HF was consistent in the two observational approaches. Clinicians should carefully consider the risk of falls in their selection of drugs for hypertension and in the clinical use of loop diuretics.




Similar content being viewed by others


References
Musini VM, Tejani AM, Bassett K, Wright JM. Pharmacotherapy for hypertension in the elderly. Cochrane Database Syst Rev. 2009;4:CD000028.
HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887–98.
Mukhtar O, Jackson SH. The hypertension in the very elderly trial—latest data. Br J Clin Pharmacol. 2012;75:951–4.
Messerli FH, Sulicka J, Gryglewska B. Treatment of hypertension in the elderly. N Engl J Med. 2008;359:972–3.
Dhruva SS, Redberg RF. Variations between clinical trial participants and Medicare beneficiaries in evidence used for Medicare national coverage decisions. Arch Intern Med. 2008;168:136–40.
Van Spall HG, Toren A, Kiss A, Fowler RA. Eligibility criteria of randomized controlled trials published in high-impact general medical journals: a systematic sampling review. JAMA. 2007;297:1233–40.
Corrao G, Mancia G. Generating evidence from computerized healthcare utilization databases. Hypertension. 2015;65:490–8.
Tinetti ME, Han L, Lee DS, et al. Antihypertensive medications and serious fall injuries in a nationally representative sample of older adults. JAMA Intern Med. 2014;174:588–95.
Nyberg L, Gustafson Y, Berggren D, et al. Falls leading to femoral neck fractures in lucid older people. J Am Geriatr Soc. 1996;44:156–60.
Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in ambulatory care. N Engl J Med. 2003;348:1556–64.
Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107–16.
Field TS, Gurwitz JH, Harrold LR, et al. Risk factors for adverse drug events among older adults in the ambulatory setting. J Am Geriatr Soc. 2004;52:1349–54.
Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med. 2009;169:1952–60.
Gribbin J, Hubbard R, Gladman J, et al. Risk of falls associated with antihypertensive medication: self-controlled case series. Pharmacoepidemiol DS. 2011;20:879–84.
Gribbin J, Hubbard R, Gladman JRF, Smith C, Lewis S. Risk of falls associated with antihypertensive medication: population-based case-control study. Age Ageing. 2010;39:592–7.
Butt DA, Mamdani M, Austin PC, Tu K, Gomes T, Glazier RH. The risk of hip fracture after initiating antihypertensive drugs in the elderly. Arch Intern Med. 2012;172:1739–44.
Berry SD, Zhu Y, Choi H, Kiel DP, Zhang Y. Diuretic initiation and the acute risk of hip fracture. Osteoporos Int. 2013;24:689–95.
Solomon DH, Mogun H, Garneau K, Fischer MA. Risk of fractures in older adults using antihypertensive medications. J Bone Miner Res. 2011;26:1561–7.
Heidrich FE, Stergachis A, Gross KM. Diuretic drug use and the risk for hip fracture. Ann Intern Med. 1991;115:1–6.
Song HJ, Lee J, Y-j Kim, et al. β1 selectivity of β-blockers and reduced risk of fractures in elderly hypertension patients. Bone. 2012;51:1008–15.
Wiens M, Etminan M, Gill SS, Takkouche B. Effects of antihypertensive drug treatments on fracture outcomes: a meta-analysis of observational studies. J Intern Med. 2006;260:350–62.
de Vries F, Souverein PC, Cooper C, et al. Use of β-blockers and the risk of hip/femur fracture in the United Kingdom and The Netherlands. Calcif Tissue Int. 2007;80:69–75.
Schlienger RG, Kraenzlin ME, Jick SS, Meier CR. Use of β-blockers and risk of fractures. JAMA. 2004;292:1326–32.
Thorell K, Ranstad K, Midlöv P, et al. Is use of fall risk-increasing drugs in an elderly population associated with an increased risk of hip fracture, after adjustment for multimorbidity level: a cohort study. BMC Geriatr. 2014;14:131.
Shuto H, Imakyure O, Matsumoto J, et al. Medication use as a risk factor for inpatient falls in an acute care hospital: a case-crossover study. Br J Clin Pharmacol. 2010;69:535–42.
Taggart HM. Do drugs affect the risk of hip fracture in elderly women? J Am Geriatr Soc. 1988;36:1006–10.
Rejnmark L, Vestergaard P, Mosekilde L. Fracture risk in patients treated with loop diuretics. J Intern Med. 2006;259:117–24.
Lim LS, Fink HA, Blackwell T, et al. Loop diuretic use and rates of hip bone loss and risk of falls and fractures in older women. J Am Geriatr Soc. 2009;57:855–62.
Carbone LD, Johnson KC, Bush AJ, et al. Loop diuretic use and fracture in postmenopausal women: findings from the Women’s Health Initiative. Arch Intern Med. 2009;169:132–40.
Corrao G, Nicotra F, Parodi A, et al. Cardiovascular protection by initial and subsequent combination of antihypertensive drugs in daily life practice. Hypertension. 2011;58:566–72.
Mancia G, Parodi A, Merlino L, Corrao G. Heterogeneity in antihypertensive treatment discontinuation between drugs belonging to the same class. J Hypertens. 2011;29:1012–8.
Corrao G, Parodi A, Nicotra F, et al. Better compliance to antihypertensive medications reduces cardiovascular risk. J Hypertens. 2011;29:610–8.
Corrao G, Zambon A, Parodi A, et al. Incidence of cardiovascular events in Italian patients with early discontinuations of antihypertensive, lipid-lowering, and antidiabetic treatments. Am J Hypertens. 2012;25:549–55.
Corrao G, Soranna D, La Vecchia C, et al. Medication persistence and the use of generic and brand-name blood pressure-lowering agents. J Hypertens. 2014;32:1146–53.
Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348:42–9.
Malabu UH, Vangaveti VN, Kennedy RL. Disease burden evaluation of fall-related events in the elderly due to hypoglycemia and other diabetic complications: a clinical review. Clin Epidemiol. 2014;6:287–94.
Helin-Salmivaara A, Korhonen MJ, Lehenkari P, et al. Statins and hip fracture prevention—a population based cohort study in women. PLoS One. 2012;7:e48095.
de Groot MH, van Campen JP, Moek MA, et al. The effects of fall-risk-increasing drugs on postural control: a literature review. Drugs Aging. 2013;30:901–20.
Charlson ME, Charlson RE, Peterson JC, et al. The Charlson comorbidity index is adapted to predict costs of chronic disease in primary care patients. J Clin Epidemiol. 2008;61:1234–40.
Delaney JA, Suissa S. The case-crossover study design in pharmacoepidemiology. Stat Methods Med Res. 2009;18:53–65.
Lambert DG, Thomas GD. {alpha}-Adrenoceptor constrictor responses and their modulation in slow-twitch and fast-twitch mouse skeletal muscle. J Physiol. 2005;563:821–9.
Poon IO, Braun U. High prevalence of orthostatic hypotension and its correlation with potentially causative medications among elderly veterans. J Clin Pharm Ther. 2005;30:173–8.
Gangavati A, Hajjar I, Quach L, et al. Hypertension, orthostatic hypotension, and the risk of falls in a community-dwelling elderly population: the maintenance of balance, independent living, intellect, and zest in the elderly of Boston study. J Am Geriatr Soc. 2011;59:383–9.
Capewell S, Capewell A. “First dose” hypotension and venodilatation. Br J Clin Pharmacol. 1991;31:213–5.
Slavachevsky I, Rachmani R, Levi Z, Brosh D, Lidar M, Ravid M. Effect of enalapril and nifedipine on orthostatic hypotension in older hypertensive patients. J Am Geriatr Soc. 2000;48:807–10.
Lipsitz LA. Abnormalities in blood pressure homeostasis that contribute to falls in the elderly. Clin Geriatr Med. 1985;1:637–48.
Pool JL, Glazer R, Chiang YT, Gatlin M. Dose-response efficacy of valsartan, a new angiotensin II receptor blocker. J Hum Hypertens. 1999;13:275–81.
Butt DA, Mamdani M, Austin PC, Tu K, Gomes T, Glazier RH. The risk of falls on initiation of antihypertensive drugs in the elderly. Osteoporos Int. 2013;24:2649–57.
Poluzzi E, Strahinja P, Vargiu A, et al. Initial treatment of hypertension and adherence to therapy in general practice in Italy. Eur J Clin Pharmacol. 2005;61:603–9.
Hallas J, Pottegård A. Use of self-controlled designs in pharmacoepidemiology. J Intern Med. 2014;275:581–9.
Román Ortiz C, Tenías JM, Estarlich M, Ballester F. Systematic review of the association between climate and hip fractures. Int J Biometeorol. 2015;59:1511–22.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Support for this study come from the Italian Ministry of Education, University and Research grants (“Fondo d’Ateneo per la Ricerca” portion, year 2014).
Disclosures
GC has received research support from the European Community (EC), the Italian Agency of Drugs (AIFA), and the Italian Ministry for University and Research (MIUR). He has taken part in a variety of projects funded by pharmaceutical companies (i.e., Novartis and GSK). He has also received honoraria as member of Advisory Board from Roche.
GM has received honoraria for participation as speaker/chairman in national/international meetings from Bayer, Boehringer Ingelheim, CVRx, Daiichi Sankyo, Ferrer, Medtronic, Menarini Int., Merck, Novartis, Recordati, and Servier.
PM, MMC, FR, LM, and GA declare that they have no conflicts of interest.
Research involving human participants and/or animals
The present research did not involve any trials on human participants or animals.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Corrao, G., Mazzola, P., Monzio Compagnoni, M. et al. Antihypertensive Medications, Loop Diuretics, and Risk of Hip Fracture in the Elderly: A Population-Based Cohort Study of 81,617 Italian Patients Newly Treated Between 2005 and 2009. Drugs Aging 32, 927–936 (2015). https://doi.org/10.1007/s40266-015-0306-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40266-015-0306-5