
Abstract
Introduction
We investigated improvement of electrocardiographic LVH detection by adding measures of adiposity and/or novel electrocardiographic measures. Left ventricular hypertrophy (LVH) is an important risk factor for adverse cardiovascular outcomes. Improvement of electrocardiographic criteria for LVH is desirable, since electrocardiography is widely used.
Methods
We included 1091 participants of the Netherlands Epidemiology of Obesity Study (NEO) who underwent cardiac magnetic resonance imaging (MRI). Performance of Sokolow–Lyon and Cornell voltage and product criteria was assessed. Stepwise regression analysis was performed with each conventional electrocardiographic criterion and age, sex, body mass index (BMI), waist circumference, and waist:hip ratio (p-entry < 0.05, p-removal > 0.10). T-wave abnormalities or the spatial QRS-T angle (SA) were added to the improved models.
Results
The study population had a mean (SD) age of 56 (6) years, BMI of 26.1 (4.0) kg/m2 and 46% were men. MRI-LVH was present in 10% of participants. The c-statistic for Sokolow–Lyon voltage was 0.58, R2 was 0.02 and sensitivity at 90% specificity was 16%, for Sokolow–Lyon product this was 0.62, 0.02, and 21%, for Cornell voltage 0.65, 0.04, and 28% and for Cornell product 0.67, 0.04, and 25%. Best performing models were obtained by addition of both BMI and SA (Sokolow-Lyon voltage: c-statistic 0.74, R2 0.11, sensitivity of 41% at 90% specificity; Sokolow-Lyon product: 0.75, 0.12, 42%; Cornell voltage: c-statistic 0.70, R2 0.08, sensitivity of 38% at 90% specificity; Cornell product: c-statistic 0.72, R2 0.08, sensitivity of 44% at 90% specificity).
Conclusions
Electrocardiographic detection of LVH improved by adding BMI and SA to a model with conventional electrocardiographic criteria. This approach would require little extra effort and application in clinical practice is feasible. However, results should first be replicated in high-risk populations.
Similar content being viewed by others

Why carry out this study? |
Electrocardiography is widely used, among others for detection of left ventricular hypertrophy, an important risk factor for adverse cardiovascular outcomes. |
We investigated whether electrocardiographic left ventricular hypertrophy detection could be improved by adding measures of adiposity and/or novel electrocardiographic measures. |
What was learned from the study? |
Adding body mass index and the spatial QRS-T angle to conventional electrocardiographic criteria improved performance in left ventricular hypertrophy detection. |
The practical application of these additions to conventional electrocardiographic criteria is feasible and this approach would require little extra effort, however these results first need to be replicated in other relevant populations. |
Introduction
Left ventricular hypertrophy (LVH) is an important risk factor for cardiovascular events and cardiovascular death [1, 2]. Several electrocardiographic criteria for the diagnosis of LVH exist, e.g., Sokolow–Lyon voltage and Cornell voltage criterion. However, these criteria show limited performance compared with diagnosis of LVH by echocardiography or (the ‘gold standard’) cardiac magnetic resonance imaging (MRI). With acceptable specificities, sensitivities are often low (7–40% for Sokolow–Lyon voltage and 2–19% for Cornell voltage criterion) [3]. Nevertheless, electrocardiograms are more easily obtainable and cost-effective compared with echocardiography or cardiac MRI, and for those reasons more often used in current clinical practice. Therefore, improvement of the electrocardiographic diagnosis of LVH is desired.
The performance of electrocardiographic criteria for the diagnosis of LVH can be influenced by body fat. Obesity is often accompanied by systemic hypertension and associated with a higher prevalence of LVH, but also, adipose tissue can attenuate electrocardiographic voltages, which interferes with LVH detection by electrocardiographic criteria [4, 5]. To take measures of body fat together with conventional electrocardiographic criteria into the diagnostic model for LVH has previously been proposed in the literature as a method that might lead to improved electrocardiographic LVH detection [5,6,7,8]. Several studies investigated the addition of BMI and showed improved performance [5,6,7,8]. However, to our knowledge, there are no studies that have investigated the addition of other measures of body fat and body fat distribution to the conventional electrocardiographic criteria.
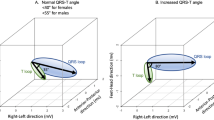
Furthermore, LVH is associated with alterations in ventricular repolarization and depolarization through several mechanisms, such as an increase in collagen interstitial matrix or changes in ionic channels [9, 10]. These changes in ventricular depolarization and repolarization can be reflected in T-wave abnormalities and the spatial QRS-T angle [11], which can both be determined from the electrocardiogram. Therefore, these measures might also be useful in the electrocardiographic diagnosis of LVH. It was previously shown that a combination of body surface area and spatial QRS-T angle can improve electrocardiographic diagnosis of LVH [12].
This study aimed to investigate whether addition of measures of body fat and body fat distribution and additional T-wave abnormalities or spatial QRS-T angle to conventional electrocardiographic criteria of LVH could improve the electrocardiographic detection of LVH.
Methods
Study Design and Population
The Netherlands Epidemiology of Obesity study (NEO) is a population-based cohort study including 6671 individuals. Men and women aged between 45 and 65 years with a BMI ≥ 27 kg/m2 living in the area of greater Leiden (The Netherlands) could participate in the NEO study. In addition, all inhabitants aged between 45 and 65 years from one municipality (Leiderdorp) were invited irrespective of their BMI, allowing for a reference distribution of BMI. Of the participants without contra-indications for MRI (most notably metallic devices, claustrophobia, or a body circumference of more than 1.70 m), a random subsample of approximately 20% of participants underwent cardiac MRI. Individuals completed a questionnaire with demographic, lifestyle, and clinical information. At the study center in the Leiden University Medical Centre (LUMC), all individuals underwent an extensive physical examination, including anthropometry, blood sampling (after an overnight fast), and electrocardiography. The present analysis is a cross-sectional analysis using the baseline measurements of the NEO study. We excluded participants in whom no cardiac MRI was performed or measurement of left ventricular mass (LVM) was missing, participants with abnormalities that could interfere with the electrocardiographic detection of LVH or the assessment of the spatial QRS-T angle, namely individuals with complete bundle branch block, ventricular pre-excitation (Wolff–Parkinson–White syndrome), previous myocardial infarction or a paced rhythm, and also individuals with missing values of the spatial QRS-T angle. Further details of the study design and population have been described in detail elsewhere [13]. The Medical Ethical Committee of the LUMC approved the design of the study and all individuals gave their written informed consent.
Data Collection
Ethnicity was self-identified in eight categories and grouped into white and other. Body height and weight were measured without shoes and 1 kg was subtracted from the weight to correct for clothing. Waist circumference was measured with a horizontally placed flexible tape in the middle of the distance between the lowest rib and the iliac crest. Hip circumference was measured at the maximum circumference of the buttocks. Brachial blood pressure was measured in a seated position on the right arm using a validated automatic oscillometric device (OMRON, Model M10-IT, Omron Health Care Inc, Chicago, IL, USA). Blood pressure was measured three times with 5 min of rest between consecutive measurements. The mean systolic and diastolic blood pressure was calculated. Blood samples were drawn after an overnight fast of 10 h. Fasting glucose was measured with the enzymatic colorimetric method (Roche Modular Analytics P800, Roche Diagnostics Mannheim, Germany).
Electrocardiography
After a resting period of at least 10 min, 12-lead electrocardiograms were obtained using a Mortara Eli-350 (Mortara Instrument Inc., Milwaukee, WI, USA). The raw data were extracted and transferred to the University of Glasgow electrocardiogram (ECG) core lab where ECGs were automatically processed and Minnesota codes were assigned using the University of Glasgow ECG analysis program [14]. We investigated four conventional electrocardiographic criteria for LVH (continuous variables): two widely used voltage index electrocardiographic criteria, namely Sokolow–Lyon voltage and Cornell voltage, and two voltage-duration product criteria, namely Sokolow–Lyon product, and Cornell product [15,16,17,18]. Sokolow–Lyon voltage was defined as |SV1| + RV5/6 and Sokolow–Lyon product as Sokolow–Lyon voltage × QRS duration. Cornell voltage was defined as RaVL + |SV3| with 600 μV added for women and Cornell product was defined as Cornell voltage × QRS duration. T-wave abnormalities were defined as Minnesota Codes 5-1 or 5-2.
Standard 10-s ECGs were each stored in an 8-lead (I, II, II, V1–V6), 5000 sample comma-separated-value file. The Kors matrix was used to calculate vector cardiograms from the eight independent ECG leads [19]. ECGs and vector cardiograms were analyzed using the automatic MATLAB-based (The MathWorks, Natick, MA, USA) program BEATS and the semiautomatic program LEADS [20, 21]. BEATS was used to detect the timings of all QRS complexes and calculated R–R intervals (ms). The QRS and T integral vectors were approximated by calculating the numerical sum of x–y–z deflections (amplitudes of positive deflections are added and those of negative deflections subtracted). The spatial QRS-T angle was defined as the angle (°) between the integral QRS vector and the integral T vector.
Magnetic Resonance Imaging
In 1150 participants, LVM was assessed using cardiac magnetic resonance imaging. The heart was imaged in the short-axis orientation by using ECG gated breath-hold balanced steady-state free precession imaging. Using in-house-developed software packages (MASS and FLOW; LUMC, Leiden, The Netherlands), image postprocessing was performed and decisions were based on consensus between two experienced observers.
LVM was indexed by height1.7 to obtain left ventricular mass index (LVMI). LVM was not indexed by body surface area to prevent underestimation of the prevalence of LVH in the NEO study population, which has a high prevalence of overweight and obese individuals [22]. Cut-offs for LVH were based on the sex-specific upper limits of normality (95th percentile) from a subgroup of 252 healthy individuals from the NEO study, with a BMI < 30 kg/m2, normal blood pressure (< 135/< 85 mmHg and no use of antihypertensive medication), no history of cardiovascular disease and normal glucose metabolism (no self-reported diabetes mellitus I or II or medication and fasting plasma glucose < 7 mmol/l). LVH was defined as LVMI > 51.9 g/m1.7 in men and LVMI > 41.8 g/m1.7 in women.
Statistical Analysis
Adjustments for the oversampling of individuals with BMI ≥ 27 kg/m2 in the NEO study were made to correctly represent baseline associations in the general population. This was done by weighting individuals towards the BMI distribution of participants from the Leiderdorp municipality, whose BMI distribution was similar to the BMI distribution of the general Dutch population. Baseline characteristics are presented as mean (SD), median (IQR), or as percentage.
First, univariate discriminative performance for LVH of the conventional electrocardiographic criteria, namely Sokolow–Lyon voltage, Sokolow–Lyon product, Cornell voltage, and Cornell product was assessed using the area under the curve (AUC) of the receiver operating characteristic (ROC) curve. The AUC reflects how well individuals are classified as having LVH or no LVH. Also, sensitivities of the conventional electrocardiographic criteria were determined at a specificity of 90%, since especially specificities of 90–100% are clinically relevant for detection of LVH. Second, univariate discriminative performance for LVH of age, sex, BMI, waist circumference, and waist:hip ratio was assessed with the AUC. Then, stepwise logistic regression analysis with an entry criterion of p < 0.05 and removal criterion of p > 0.10 was performed with LVH as dependent variable and each conventional electrocardiographic criterion separately with addition of the variables age, sex, BMI, waist circumference, and waist:hip ratio as independent variables. AUC, R2, and sensitivity at 90% specificity of the selected models were assessed. Univariate discriminative performance for LVH of T-wave abnormalities (dichotomous) and the spatial QRS-T angle was also assessed using the AUC. Finally, for each conventional electrocardiographic criterion separately, the best performing models were determined, consisting of a combination of the best performing measure of body fat and the best of T-wave abnormalities and spatial QRS-T angle. AUC, R2, sensitivities at a specificity of 90% and calibration plots were reported for the new models for LVH detection. Furthermore, the internal validity of the estimated AUC values was assessed using bootstrapping. Data were analyzed using STATA (StataCorp, College Station, TX, USA), version 14.
Compliance with Ethics Guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Medical Ethical Committee of the LUMC and the study conformed with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all participants.
Results
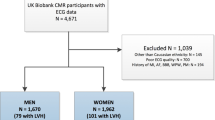
Cardiac magnetic resonance imaging was performed in 1278 participants. Participants in whom measurement of LVM was missing (n = 128), in addition to participants with left or right bundle branch block (n = 21), history of myocardial infarction (n = 14), Wolff–Parkinson–White syndrome (n = 1) or missing spatial QRS-T angle (n = 23) were excluded. Baseline characteristics of the 1091 individuals included in the study are presented in Table 1. The study population had a mean (SD) age of 56 (6) years and 46% were men. Mean (SD) blood pressure was 131.5 (18.2)/84.1 (10.8) mmHg and 22% of the study population was taking antihypertensive medication. According to the MRI-based sex-specific cut-offs, 10% of this study population was defined as having LVH.
Univariate discriminative performance of the conventional electrocardiographic criteria alone was poor. AUC for Sokolow–Lyon voltage was 0.58 (95% CI 0.53, 0.63) and R2 0.02, for Sokolow–Lyon product 0.62 (0.57, 0.66) and 0.02, for Cornell voltage 0.65 (0.61, 0.70) and 0.04 and for Cornell product 0.67 (0.63, 0.72) and 0.04. Furthermore, at a specificity of 90%, Sokolow–Lyon voltage showed a sensitivity of 16%, Sokolow–Lyon product a sensitivity of 21%, Cornell voltage a sensitivity of 28% and Cornell product a sensitivity of 25%. ROC curves for the conventional electrocardiographic criteria are displayed in Fig. 1a.

Receiver operating characteristic curves and area under the curve values of electrocardiographic criteria (a) and age, sex, body mass index, waist circumference and waist:hip ratio (b) for detection of LVH, in 1091 participants aged 45–65 years from the Netherlands Epidemiology of Obesity Study. Results were based on analyses weighted towards the BMI distribution of the general population. BMI body mass index, WHR waist:hip ratio
Univariate discriminative performance of age, sex, BMI, waist circumference, and waist:hip ratio was also estimated with the AUC. BMI (0.67, 95% CI 0.63, 0.72), waist circumference (0.66; 0.61, 0.71) and waist:hip ratio (0.57; 0.52, 0.62) showed discriminative power for LVH, whereas age (0.50; 0.45, 0.55) and sex (0.52; 0.48, 0.56) did not. ROC curves for age, sex, BMI, waist circumference, and waist:hip ratio are displayed in Fig. 1b.
Using stepwise regression analyses with the variables age, sex, BMI, waist circumference and waist:hip ratio, models for each conventional electrocardiographic criterion and additionally BMI were selected. Addition of BMI to models with Sokolow–Lyon voltage, improved the AUC to 0.71 (p < 0.01) and AUC was improved to 0.73 for Sokolow–Lyon product (p < 0.01), 0.70 for Cornell voltage (p = 0.01) and 0.72 for Cornell product (p = 0.01). The addition of BMI also led to improvements in R2 and sensitivity at 90% specificity, as shown in Table 2.
The addition of waist circumference to models with the conventional electrocardiographic criteria also led to improvements in R2 and sensitivity at 90% specificity, as shown in Table S1. Addition of waist circumference led to smaller improvement of the models than the addition of BMI did.
Presence of T-wave abnormalities (dichotomous) had no discriminative performance for LVH with AUC 0.51 and this was 0.62 for spatial QRS-T angle (ROC curves shown in Figure S1). When T-wave abnormalities were added to models with each conventional electrocardiographic criteria in combination with BMI, AUC did not improve (results not shown).
Addition of spatial QRS-T angle to the models with each conventional electrocardiographic criterion and BMI did lead to improved performance, as is presented in Table 3. Models with the conventional electrocardiographic criteria and additionally BMI and spatial QRS-T angle showed the best performance. ROC curves for these models, compared with models with each electrocardiographic criterion alone, are presented in Fig. 2. The combination of Sokolow–Lyon voltage, BMI, and spatial QRS-T angle showed an AUC of 0.74, R2 of 0.11, and a sensitivity of 41% at a matched specificity of 90%. This was 0.75, 0.12, and 42% for the combination of Sokolow–Lyon product, BMI and spatial QRS-T angle, 0.70, 0.08, and 38% for the combination of Cornell voltage, BMI, and spatial QRS-T angle, and 0.72, 0.08, and 44% for the combination of Cornell product, BMI, and spatial QRS-T angle. For these four models, calibration plots are presented in Figure S2. Furthermore, bootstrapping showed good internal validity for the estimated AUC values. In conclusion, the best performance in the detection of LVH was reached by a combination of Sokolow–Lyon product, BMI and spatial QRS-T angle.

Receiver operating characteristic curves and area under the curve values of the conventional electrocardiographic criteria alone and with addition of body mass index and spatial QRS-T angle for detection of left ventricular hypertrophy, in 1091 participants aged 45–65 years from the Netherlands Epidemiology of Obesity Study. Results were based on analyses weighted towards the BMI distribution of the general population. BMI body mass index
Discussion
In this population of middle-aged men and women, in whom cardiac MRI was performed, adding BMI (which is easily determinable) to conventional electrocardiographic criteria, more so than waist circumference or waist:hip ratio, improved performance in detection of LVH. Additionally, adding the spatial QRS-T angle to the models with both the ECG criterion and BMI improved performance even further. For example, AUC for detection of LVH of Sokolow–Lyon product was 0.62 and sensitivity at a specificity of 90% was 21%, and with addition of BMI and spatial QRS-T angle this improved to AUC 0.75 and 42%.
Comparison with Previous Literature
The poor performance of conventional electrocardiographic criteria for LVH detection has previously been described [3]. A systematic review showed that in primary care settings, sensitivity of Sokolow–Lyon voltage criteria ranged from 8 to 40% at specificities 53–100% and sensitivity of Cornell voltage criteria ranged from 2 to 19% at specificities 89–100% [3]. In individuals with systemic hypertension, the combination of Cornell voltage with BMI improved the performance in LVH detection [6]. In a population-based study (n = 3351), adding both BMI and age to Cornell product improved its performance and in another study adding BMI to Sokolow–Lyon voltage or Cornell voltage improved their performance [5, 8]. To our knowledge, few studies have investigated the addition of spatial QRS-T angle to electrocardiographic LVH criteria [12]. In 196 individuals, a combination of body surface area and spatial QRS-T angle yielded the best diagnostic accuracy for LVH (using echocardiography as reference standard), superior to that of conventional electrocardiographic criteria [12]. In our study, a combination of BMI and spatial QRS-T angle alone (without other electrocardiographic criteria) would yield an AUC of 0.70, which is higher than the AUC of the conventional electrocardiographic criteria alone, but, however not higher than the conventional electrocardiographic criteria combined with BMI and spatial QRS-T angle.
Interpretation and Mechanisms
LVH is a pathological remodeling of the left ventricle, often in response to increased afterload. Presence of increased afterload is commonly seen with systemic hypertension, increased peripheral resistance and increased arterial stiffness, which are prevailing in obese individuals [23]. Next to the known association of obesity with an increased risk of LVH, several studies showed that electrocardiographic criteria for LVH have very limited performance, especially in obese individuals [24, 25]. Also in this present study, discriminative performance of the conventional electrocardiographic criteria is poor, especially of the Sokolow–Lyon criteria (AUC Sokolow–Lyon voltage 0.58, Sokolow–Lyon product 0.62). Probably, precordial electrocardiographic voltages (affecting Sokolow–Lyon voltage and product more than Cornell voltage and product) are reduced due to the presence of increased epicardial fat mass and a large chest wall, which corresponds to the findings in this present study. Before addition of BMI to the conventional electrocardiographic criteria, Sokolow–Lyon voltage and product performed worse than Cornell voltage and product, and after adjustment for BMI, performances of Sokolow–Lyon and Cornell criteria were similar. This may partly be explained by the fact that the Sokolow–Lyon criteria depend more on precordial voltages than Cornell criteria do.
Hypertrophy of the left ventricle is often accompanied by electrophysiological changes and repolarization inhomogeneities [26]. In the hypertrophic heart, action potential duration is prolonged because of delayed conduction and also several other mechanisms are at play, among which are alterations in ionic channels and changes in ventricular repolarization induced by an increase in collagen interstitial matrix [9, 10, 27, 28]. These changes can be reflected in T-wave abnormalities or widening of the spatial QRS-T angle, as described in literature [29, 30]. Computation of the spatial QRS-T angle from the ECG has become easier and therefore taking into account the spatial QRS-T angle in detecting LVH, which is shown valuable in this study, could possibly be translated into clinical practice.
Strengths and Limitations
This study has several important strengths. Firstly, LVH was determined by ‘the gold standard’ MRI in a large number of individuals (n = 1091), in whom also electrocardiographic LVH criteria, spatial QRS-T angle and T-wave abnormalities were available. Also, we were able to assess addition of several anthropometric measures, whereas other studies could only investigated addition of BMI. Several limitations apply to this study. First, since our study was performed in a population-based cohort of mostly white, middle-aged individuals (45–65 years), extrapolation to other populations with different ethnic backgrounds, age ranges or patient populations should be done with caution. Furthermore, in this study we chose to focus on four widely used electrocardiographic criteria of LVH. However, more electrocardiographic criteria for LVH diagnosis exist, which were not included in this study, since they are less often used in clinical practice. Finally, the approach requires to be validated in relevant patient populations.
Conclusions
ECGs are easily obtainable, low-cost and widely used in clinical practice, and therefore improvements in electrocardiographic detection of LVH, which is strongly associated with adverse cardiovascular outcomes, is very relevant. This study shows possible improvement of electrocardiographic LVH criteria by addition of BMI and the spatial QRS-T angle, which could be useful in clinical practice. Results provided by this study should first be replicated in different patient populations or more high-risk populations.
References
Kannel WB, Gordon T, Offutt D. Left ventricular hypertrophy by electrocardiogram. Prevalence, incidence, and mortality in the Framingham study. Ann Intern Med. 1969;71(1):89–105.
Hawkins NM, Wang D, McMurray JJ, et al. Prevalence and prognostic implications of electrocardiographic left ventricular hypertrophy in heart failure: evidence from the CHARM programme. Heart. 2007;93(1):59–64.
Pewsner D, Juni P, Egger M, Battaglia M, Sundström J, Bachmann LM. Accuracy of electrocardiography in diagnosis of left ventricular hypertrophy in arterial hypertension: systematic review. BMJ. 2007;335(7622):711.
Masui A, Tsuji H, Tamura K, et al. Effect of body characteristics on the variables of signal-averaged electrocardiograms in healthy subjects. Chest. 1994;105(5):1357–9.
Cuspidi C, Facchetti R, Bombelli M, et al. Does QRS voltage correction by body mass index improve the accuracy of electrocardiography in detecting left ventricular hypertrophy and predicting cardiovascular events in a general population? J Clin Hypertens (Greenwich). 2016;18(5):415–21.
Angeli F, Verdecchia P, Iacobellis G, Reboldi G. Usefulness of QRS voltage correction by body mass index to improve electrocardiographic detection of left ventricular hypertrophy in patients with systemic hypertension. Am J Cardiol. 2014;114(3):427–32.
Robinson C, Woodiwiss AJ, Libhaber CD, Norton GR. Novel approach to the detection of left ventricular hypertrophy using body mass index-corrected electrocardiographic voltage criteria in a group of African ancestry. Clin Cardiol. 2016;39(9):524–30.
Norman JE Jr, Levy D. Adjustment of ECG left ventricular hypertrophy criteria for body mass index and age improves classification accuracy. The effects of hypertension and obesity. J Electrocardiol. 1996;29:241–7.
Xu X, Rials SJ, Wu Y, et al. Left ventricular hypertrophy decreases slowly but not rapidly activating delayed rectifier potassium currents of epicardial and endocardial myocytes in rabbits. Circulation. 2001;103(11):1585–90.
Pye MP, Cobbe SM. Mechanisms of ventricular arrhythmias in cardiac failure and hypertrophy. Cardiovasc Res. 1992;26(8):740–50.
Draisma HH, Schalij MJ, van der Wall EE, Swenne CA. Elucidation of the spatial ventricular gradient and its link with dispersion of repolarization. Heart Rhythm. 2006;3(9):1092–9.
Man S, Rahmattulla C, Maan AC, et al. Role of the vectorcardiogram-derived spatial QRS-T angle in diagnosing left ventricular hypertrophy. J Electrocardiol. 2012;45(2):154–60.
de Mutsert R, den Heijer M, Rabelink TJ, et al. The Netherlands Epidemiology of Obesity (NEO) study: study design and data collection. Eur J Epidemiol. 2013;28(6):513–23.
Blackburn H, Keys A, Simonson E, Rautaharju P, Punsar S. The electrocardiogram in population studies. A classification system. Circulation. 1960;21:1160–75.
Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J. 1949;37(2):161–86.
Casale PN, Devereux RB, Alonso DR, Campo E, Kligfield P. Improved sex-specific criteria of left ventricular hypertrophy for clinical and computer interpretation of electrocardiograms: validation with autopsy findings. Circulation. 1987;75(3):565–72.
Molloy TJ, Okin PM, Devereux RB, Kligfield P. Electrocardiographic detection of left ventricular hypertrophy by the simple QRS voltage-duration product. J Am Coll Cardiol. 1992;20(5):1180–6.
Okin PM, Roman MJ, Devereux RB, Kligfield P. Electrocardiographic identification of increased left ventricular mass by simple voltage-duration products. J Am Coll Cardiol. 1995;25(2):417–23.
Kors JA, van Herpen G, Sittig AC, van Bemmel JH. Reconstruction of the Frank vectorcardiogram from standard electrocardiographic leads: diagnostic comparison of different methods. Eur Heart J. 1990;11(12):1083–92.
Man SC, Maan AC, van der Wall EE, Schalij MJ, Swenne CA. Beats: an interactive research oriented ECG analysis system. Comput Cardiol. 2010;37:1007–10.
Draisma HHM, Swenne CA, van der Vooren H, et al. LEADS: an interactive research oriented ECG/VCG analysis system. Comput Cardiol. 2005;32:515–8.
Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–63.
Sutton-Tyrrell K, Newman A, Simonsick EM, et al. Aortic stiffness is associated with visceral adiposity in older adults enrolled in the study of health, aging, and body composition. Hypertension. 2001;38(3):429–33.
Fraley MA, Birchem JA, Senkottaiyan N, Alpert MA. Obesity and the electrocardiogram. Obes Rev. 2005;6(4):275–81.
Cuspidi C, Rescaldani M, Sala C, Grassi G. Left-ventricular hypertrophy and obesity: a systematic review and meta-analysis of echocardiographic studies. J Hypertens. 2014;32(1):16–25.
Hansen DE. Mechanoelectrical feedback effects of altering preload, afterload, and ventricular shortening. Am J Physiol. 1993;264(2 Pt 2):H423–32.
Winterton SJ, Turner MA, O’Gorman DJ, Flores NA, Sheridan DJ. Hypertrophy causes delayed conduction in human and guinea pig myocardium: accentuation during ischaemic perfusion. Cardiovasc Res. 1994;28(1):47–54.
McIntyre H, Fry CH. Abnormal action potential conduction in isolated human hypertrophied left ventricular myocardium. J Cardiovasc Electrophysiol. 1997;8(8):887–94.
Dilaveris P, Gialafos E, Pantazis A, Synetos A, Triposkiadis F, Gialafos J. The spatial QRS-T angle as a marker of ventricular repolarisation in hypertension. J Hum Hypertens. 2001;15(1):63–70.
Oikarinen L, Vaananen H, Dabek J, et al. Relation of twelve-lead electrocardiographic T-wave morphology descriptors to left ventricular mass. Am J Cardiol. 2002;90(9):1032–5.
Acknowledgements
We express our gratitude to all participants of the Netherlands Epidemiology in Obesity Study, in addition to all participating general practitioners. We furthermore thank P.R. van Beelen and all research nurses for collecting the data and P.J. Noordijk and her team for sample handling and storage and I. de Jonge for data management.
Funding
This work was supported by the participating Departments; the Division and the Board of Directors of the Leiden University Medical Centre, and by the Leiden University, Research Profile Area ‘Vascular and Regenerative Medicine’. No Rapid Service Fee was received by the journal for the publication of this article.”
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Theodora W. Elffers, Stella Trompet, Renée de Mutsert, Arie C. Maan, Hildo J. Lamb, Peter W. Macfarlane and Frits R. Rosendaal have nothing to disclose. J Wouter Jukema is a member of the journal’s Editorial Board.
Compliance with Ethics Guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Medical Ethical Committee of the LUMC and the study conformed with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all participants.
Data Availability
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request. Due to the privacy of the participants of the NEO study and legal reasons, we cannot publicly deposit the data. Also, NEO study participants did not sign informed consent to make their data publicly available. Data will be made available upon request to interested qualified researchers. Data requests should be sent to the NEO Executive Board which can be contacted via https://www.lumc.nl/org/neo-studie/contact/. https://www.lumc.nl/org/neo-studie/contact/.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.9952463.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Elffers, T.W., Trompet, S., de Mutsert, R. et al. Electrocardiographic Detection of Left Ventricular Hypertrophy; Adding Body Mass Index and Spatial QRS-T Angle: A Cross-Sectional Study. Cardiol Ther 8, 345–356 (2019). https://doi.org/10.1007/s40119-019-00151-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40119-019-00151-9