
Abstract
Background
The objective of this study was to investigate the clinical feasibility of near-infrared spectroscopy (NIRS) for the detection of delayed cerebral ischemia (DCI) in patients with poor-grade subarachnoid hemorrhage (SAH) treated with coil embolization.
Methods
Cerebral regional oxygen saturation (rSO2) was continuously monitored via two-channel NIRS for 14 days following SAH. The rSO2 levels according to DCI were analyzed by using the Mann–Whitney U-test. A receiver operating characteristic curve was generated on the basis of changes in rSO2 by using the rSO2 level on day 1 as a reference value to determine the optimal cutoff value for identifying DCI.
Results
Twenty-four patients with poor-grade SAH were included (DCI, n = 8 [33.3%]; non-DCI, n = 16 [66.7%]). The rSO2 levels of patients with DCI were significantly lowered from 6 to 9 days compared with those in without DCI. The rSO2 level was 62.55% (58.30–63.40%) on day 6 in patients with DCI versus 65.40% (60.90–68.70%) in those without DCI. By day 7, it was 60.40% (58.10–61.90%) in patients with DCI versus 64.25% (62.50–67.10%) those without DCI. By day 8, it was 58.90% (56.50–63.10%) in patients with DCI versus 66.05% (59.90–69.20%) in those without DCI, and by day 9, it was 60.85% (58.40–65.20%) in patients with DCI versus 65.80% (62.70–68.30%) in those without DCI. A decline of greater than 14.5% in the rSO2 rate yielded a sensitivity of 92.86% (95% confidence interval: 66.1–99.8%) and a specificity of 88.24% (95% confidence interval: 72.5–96.7%) for identifying DCI. A decrease by more than 14.7% of the rSO2 level indicates a sensitivity of 85.7% and a specificity of 85.7% for identifying DCI.
Conclusions
Near-infrared spectroscopy shows some promising results for the detection of DCI in patients with poor-grade SAH. Further studies involving a large cohort of the SAH population are required to confirm our results.
Similar content being viewed by others

Introduction
Recent technical advances in neurocritical care have led to a decrease in the overall mortality rate of subarachnoid hemorrhage (SAH) from approximately 50% to 20% [1]. Nevertheless, patients with poor-grade SAH still showed higher mortality rates ranging between 34 and 77%, although the mortality rate in patients with good-grade SAH was less than 10–20% [1, 2]. Therefore, improving the outcome of patients who manifest poor clinical status is the primary concern of neurointensivists and neurosurgeons in real-world clinical practice. Delayed cerebral ischemia (DCI) is a major contributor to poor neurologic outcome after SAH [3]. Early detection and prompt management of DCI is critical to achieving good clinical outcome. Transcranial Doppler ultrasonography (TCD) is used routinely to detect vasospasm by measuring high velocities of the cerebral arteries in most critical care units, whereas computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are adjunct diagnostic modalities for DCI due to severe cerebral vasospasm. However, TCD for the detection of DCI is limited by the increased dependence on the operator and the inadequate acoustic temporal bone window in more than 10% of the patients [4]. In addition, TCD is used only once or twice daily in the clinical setting of the critical care unit. Therefore, a few patients with DCI may remain undetected in the upcoming study. CTA or MRA with perfusion imaging can be used to accurately analyze the degree of vasospasm related to DCI. However, adverse events can occur during patient transfer to the testing sites [5], particularly in patients with unstable and poor-grade SAH with multiple lines and drains. Therefore, a simple and sensitive apparatus for the continuous monitoring of DCI without depending on an operator bedside is necessary for patients with SAH presenting with poor-grade SAH.
Near-infrared spectroscopy (NIRS) has been used to determine cerebral tissue oxygenation on the basis of the exposure of brain to near-infrared light and quantification of the reflected photons [6]. NIRS reflects venous-weighted oxygenation (approximately 70% of venous blood, 25% of arterial blood, and 5% of capillary blood) in the frontal lobe [7, 8]. Currently, cerebral regional oxygen saturation (rSO2) in NIRS is usually used to monitor ischemic events during cardiovascular surgery and endovascular procedures [9]. The rSO2 level was strongly correlated with the baseline mean transit time of the perfusion magnetic resonance image in patients with ischemic stroke [10]. In addition, the levels of rSO2 were improved after recanalization in patients undergoing mechanical thrombectomy [11]. Taussky et al. [11] correlated NIRS oxygenation and regional cerebral blood flow in a perfusion computed tomography imaging study of eight stroke patients (SAH, n = 6; ischemic stroke, n = 1; intracerebral hemorrhage, n = 1) in the critical care unit. Accordingly, NIRS also represents a noninvasive, continuous bedside monitoring tool for cerebral ischemia without operator dependency, in particular for patients with poor-grade SAH who are at a high risk of DCI. In this study, we examined the diagnostic value of NIRS in DCI involving patients with poor-grade SAH.
Methods
Study Population
The study cohort was derived from the stroke database at the regional medical center of the district, a prospective task of an ongoing research study conducted between September 2016 and July 2019 [12,13,14,15]. The inclusion criteria were as follows: (1) spontaneous SAH due to aneurysm rupture, (2) age greater than 18 years, (3) poor-grade SAH, and (4) treatment with endovascular coil embolization. The exclusion criteria were as follows: (1) nonaneurysmal SAH due to trauma or infection, (2) perimesencephalic (PMH) SAH, and (3) treatment with surgical clipping. Poor-grade SAH was defined as a Hunt and Hess (H–H) grade greater than or equal to IV and a Fisher grade greater than or equal to III at admission.
Patient Monitoring
We measured rSO2 continuously for 14 days post ictus using in vivo optical spectroscopy (INVOS) (Somanetics Corp, Troy, MI) as the NIRS system. Two probe pads were uniformly located on the patients’ forehead, and the rSO2 level was measured every 2 s. The results were recorded automatically in the INVOS machine (Fig. 1) [16]. The results were downloaded, and the average values were calculated every 24 h bilaterally. The primary outcome was the differences in rSO2 according to DCI. The secondary outcome was the optimal cutoff value of rSO2 reduction to identify DCI. The reduction rate (percentage) in rSO2 during the follow-up compared with rSO2 on day 1 was used as a reference value in the analysis.

INVOS used to monitor patients with poor-grade SAH in the neuro-intensive care unit. Two probe bands were placed on the forehead (yellow circle), and cerebral regional oxygen saturation (red line) was monitored continuously at bedside without operator dependency
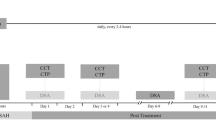
Delayed cerebral ischemia was diagnosed in patients with SAH who were capable of undergoing neurological examination on the basis of the following conditions: (1) newly developed focal neurologic changes or decreased Glasgow Coma Scale score of at least 2 points; (2) sustained symptoms lasting more than 1 h; (3) absence of other possible causes, such as rebleeding, hydrocephalus, seizures, or electrolyte imbalances; and (4) severe cerebral vasospasm on CTA or MRA, defined as a more than 50% decrease in vessel diameter in the follow-up radiological examinations compared with baseline [17, 18]. DCI was monitored by TCD daily in cases of sedation with a mechanical ventilator. CTA or MRA was performed immediately to confirm the degree of vasospasm if severe vasospasm was suspected, indicating a mean flow velocity greater than 200 cm/s in the middle cerebral artery (MCA) or 85 cm/s in the basilar artery on TCD [19, 20]. In addition, CTA was performed routinely on days 3, 7, and 14 after ictus to observe changes in vasospasm because cerebral vasospasm occurs around day 3, peaking on day 7, and resolves after 2 weeks post ictus [21, 22]. Nimodipine (20 μg/kg per hour; Samjin Pharmaceutical, Seoul, Korea) was administered intravenously in an effort to improve prognosis after endovascular coil embolization [23].
Clinical outcome was measured by using the modified Rankin Scale score at 6 months after ictus, with a score of 0–2 indicating favorable outcome [24]. Medical records and radiological images were reviewed independently by a neurologist (JJP) and a neurosurgeon (JPJ). All patients with SAH treated with endovascular coil embolization were monitored via invasive continuous arterial lines for systolic, diastolic, and mean arterial pressure and drug titration. Any disagreement was resolved by a third researcher. This study was approved by the institutional review board of the participating hospital (No. 2016-3, 2017-9, and 2018-6).
Statistical Analysis
Continuous data are presented as the mean and standard deviation (SD). Univariate analysis of factors related to DCI was performed via χ2 tests and Fisher’s exact tests or an independent t-test [25]. Comparative results of the rSO2 according to DCI were analyzed by using the Mann–Whitney U-test. A receiver operating characteristic curve was generated to determine the optimal cutoff point for identifying DCI [5, 26]. The predictive value of severe cerebral vasospasm contributing to DCI was determined by using the area under the receiver operating characteristic curve (AUROC) between NIRS and TCD. All statistical analyses were done with SPSS version 21 (IBM SPSS Statistics, IBM Corpation, Armonk, NY) and MedCalc (www.Medcalc.org). A p value of less than 0.05 was regarded as statistically significant.
Results
Characteristics of the Patients
The patients’ clinical characteristics are listed in Table 1. A total of 24 patients presenting with poor-grade SAH were included. Eight patients (33.3%) showed DCI during the follow-up, with rSO2 levels of 59.6 ± 4.9%. We recorded NIRS values for each hemisphere separately but analyzed the average results of the left and right sides for each patient. The analysis included the average NIRS value derived from eight patients with DCI with 11 hemispheres and 16 patients without DCI with 32 hemispheres. Five patients with DCI underwent unilateral NIRS measurement due to ventriculostomy or craniotomy during the follow-up to control the increased intracranial pressure (Supplemental Table S1).
High mean arterial pressure was maintained in patients with DCI treated with norepinephrine or dopamine. Other clinical and radiological findings did not differ significantly between the two groups. Most aneurysms (87.5%) were anterior circulation aneurysms. Poor clinical outcome was more frequently observed in patients with DCI compared with those without DCI, but the difference was not statistically significant (p = 0.152).
Measurement of rSO 2 Between Patients with DCI and Those Without DCI
The rSO2 levels were similar for 3 days after SAH.ss Patients with DCI experienced a greater decrease in rSO2 levels than patients without DCI beyond 3 days after the ictus (Fig. 2a). The differences in the rSO2 levels were prominent from day 6 to 9. By day 6, the rSO2 level was 62.55% (58.30–63.40%) in the patients with DCI versus 65.40% (60.90–68.70%) in the patients without DCI (p = 0.030). By day 7, it was 60.40% (58.10–61.90%) in the patients with DCI versus 64.25% (62.50–67.10%) in the patients without DCI (p < 0.001). By day 8, it was 58.90% (56.50–63.10%) in the patients with DCI versus 66.05% (59.90–69.20%) in the patients without DCI (p = 0.001). By day 9, it was 60.85% (58.40–65.20%) in the patients with DCI versus 65.80% (62.70–68.30%) in the patients without DCI (p = 0.005) (Fig. 2b). On day 5, the patients with DCI had lower rSO2 levels than the patients without DCI, but the difference was not statistically significant between patients with DCI (63.10%; 56.10–65.30%) compared with patients without DCI (64.85%; 61.80–68.10%) (p = 0.071).

Differences in cerebral regional oxygen saturation (rSO2) of NIRS according to delayed cerebral ischemia (DCI). a Chronological changes of rSO2 of NIRS in patients with DCI and non-DCI following subarachnoid hemorrhage (SAH). b Measurements of rSO2 differed significantly according to DCI on days 6, 7, 8, and 9 after ictus. The results are presented as the median and 25th–75th percentiles
Figure 3 displays the association between rSO2 levels and DCI onset in eight patients with DCI. The varying onset of DCI was as follows: 5 days, n = 1; 6 days, n = 1; 7 days, n = 3; 8 days, n = 2; and 11 days, n = 1. We generated a receiver operating characteristic curve based on changes in rSO2, with the rSO2 level on day 1 as a reference value. The AUROC was equal to 0.885 (95% confidence interval [CI]: 0.749–0.963). A greater than 14.7% decrease in the rSO2 level yielded a sensitivity of 85.7% (95% CI: 57.2–98.2%) and a specificity of 85.7% (95% CI: 67.3–96.0%) for DCI detection (Fig. 4).

Data of eight patients with delayed cerebral ischemia (DCI). Serial changes in rSO2 and the number of patients with different days of DCI onset are shown. Serial rSO2 changes and the day of DCI onset for each patient are presented in different colors

The area under the receiver operating characteristic curve is 0.8855. Reduction rate of rSO2 greater than 14.7% indicates a sensitivity of 85.7% (95% CI: 57.2–98.2%) and a specificity of 85.7% (95% CI: 67.3–96.0%) for DCI detection
Discussion
A threshold based on NIRS data and techniques for the identification of cerebral ischemia in heterogeneous patient groups was used in previous studies [7]. Although NIRS is recommended for monitoring cerebral deoxygenation in neurosurgical patients, the evidence is not strong enough [7]. Therefore, the threshold cannot be used to monitor cerebral ischemia in patients with SAH in the neurointensive care unit. Maslehaty et al. [9] continuously measured nine patients with SAH during a mean of 8.6 days (range 2–12 days) using INVOS. Seven patients with SAH without DCI exhibited constant and stable rSO2, whereas two patients showed a correlation between clinical deterioration and rSO2 declines. Mutoh et al. [27] examined rSO2 in seven patients with SAH with clipped cerebral aneurysms who underwent dobutamine-induced hemodynamic augmentation during 2–5 days. Vascular territories affected by vasospasm showed lower rSO2 levels compared with the contralateral side by 24 ± 4%. NIRS also enabled continuous assessment of cerebral autoregulation following SAH [28]. Ma, an index of cerebral autoregulation based on TCD, was well correlated with NIRS-based autoregulation indices. (r = 0.81). However, the adult patients with SAH were monitored briefly for 62.5 h by using the NIRO 2000 (Hamamatsu Photonics UK Ltd, Hertfordshire, UK), which did not cover the estimated DCI period. In addition, patients with nonaneurysmal SAH were included. Nonaneurysmal SAH exhibited different clinical outcomes according to the patterns of hemorrhage, such as PMH and non-PMH. A meta-analysis [29] demonstrated that patients with PMH SAH experienced significantly lower DCI than patients without PMH SAH (odds ratio = 0.219; 95% CI: 0.144–0.334). Therefore, changes in rSO2 reported in previous studies cannot reflect the hemodynamic changes in DCI in patients with aneurysmal SAH.
A higher H–H grade is closely associated with in-hospital mortality [30]. Lantigua et al. [30] reported that the mortality rates of H–H grades IV and V were 24% and 71%, respectively, which were higher than the in-hospital mortality rates of 3–9% in patients with a lower H–H grade. Accordingly, early detection and prompt management of DCI is essential for patients with poor-grade SAH who are at high risk of DCI. Additional hemodynamic therapies for hypertension and hypervolemia are usually administered to patients with poor-grade SAH compared with those diagnosed with good-grade SAH. Therefore, the cutoff value for rSO2 reduction should be set differently for good-grade and poor-grade SAH cases to reduce false-positive results involving good-grade SAH [31]. In this study, rSO2 observed on NIRS facilitated real-time monitoring of DCI following SAH. The optimal cutoff value of rSO2 reduction for the detection of DCI due to severe cerebral vasospasm was 14.7%, which yielded a sensitivity of 85.7% and a specificity of 85.7%.
Generally, DCI is closely associated with poor clinical outcome. No such association was observed in our study, although patients with DCI tended to show poor clinical outcomes compared with those without DCI. We only enrolled patients with poor-grade SAH, not good-grade SAH. Le Roux et al. [32] reported that poor-grade SAH outcome was closely related to initial hemorrhage and subsequent increased intracranial pressure or cerebral infarction at admission. Nonetheless, it was possible that fewer DCI cases were detected because of the diagnostic difficulty involving sedated or intubated patients.
Near-infrared spectroscopy also can be used during neuroendovascular procedures. Meng et al.[33] analyzed consecutive rSO2 levels during chemical angioplasty for vasospasm in 13 clipped patients. The rSO2 changes ipsilateral to the chemical angioplasty side were more prominent than in the contralateral side. However, changes in NIRS were inconsistent and limited in their application because of pneumocephalus. NIRS reflects the oxygen delivery and consumption only for a small frontal brain tissue after subtracting data from the surface and scalp [7]. Accordingly, air or fluid at the craniotomy sites interferes with the absorption spectrum. Therefore, we only placed the NIRS sensor pad in patients with SAH with coil embolization but not surgical clipping.
Transcranial Doppler ultrasonography is widely used to assess cerebral vasospasm following SAH. Nevertheless, technical difficulties due to poor bone window and operator dependency are a concern, limiting its use in critically ill patients [9]. Carrera et al. [34] reported that approximately 40% of patients with DCI did no show the highest mean flow velocity greater than 120 cm/s. In a case series of seven patients, NIRS successfully identified three to four patients with DCI for whom TCD velocity was ineffective [27, 35]. Compared with TCD, NIRS provides rSO2 data regardless of operator and patient condition. We also found uninterpretable data in three patients with SAH (12.5%). In 21 patients, we compared the diagnositc accuracy of NIRS with that of TCD for the identification of DCI due to severe cerebral vasospasm. As shown in Supplemental Fig. S1, the diagnositc performance of NIRS appeared to be slightly better than that of TCD but was not statistically significant (AUROC = 0.074; 95% CI: − 0.112 to 0.260). Nontheless, additional comparative studies are needed to determine the diagnostic accuracy of NIRS compared with TCD in a large cohort of patients with SAH. During prolonged monitoirng, probe adhesion to the forehead may decerase, which can interfere with data reliability. Accordingly, there is a need to switch to a different probe to obtain robust and reliable data, which can be expensive, especially when it is not covered by insurance in the neurointensive care unit. Nonetheless, there is practically no modality other than NIRS that is currenlty available to monitor DCI continuously for 24 h.
Our study has some limitations. First, we enrolled 24 patients presenting with poor-grade SAH, and the retrospective design of the study has inherent limitations of selection bias. Accordingly, treatment decisions for DCI can be influenced by the investigator not blinded to the study. Second, we defined DCI on the basis of neurological changes or decreased GCS scores concomitant with severe cerebral vasospasm. Accordingly, the study may have excluded some patients with DCI induced by cortical spreading depolarization or microthrombosis. In addition, our analysis may have included cases of angiographic vasospasm, which was not associated with DCI. Third, we merely compared the serial changes in rSO2 between eight patients with DCI and 16 without DCI with poor-grade SAH after ictus using the median and 25th–75th percentiles. The accuracy of longitudinal data analysis is enhanced by using the mean and 95% CI. Additionally, it might be difficult to detect vasospastic vessels on the basis of a simple 24-h average of rSO2 levels. Under this condition, the rSO2 variability increases the ability of rSO2 to detect cerebral vasospasm contributing to DCI. We further analyzed the rSO2 variability, such as SD and coefficient of variation (CoV), on the basis of the hourly averages of rSO2 for the detection of DCI. Compared with patients without DCI (SD 2.980 [2.320–3.380]; CoV 4.370 [3.420–5.010]), patients diagnosed with DCI had higher levels of SD (4.270 [3.560–5.490]; p < 0.001) and CoV (6.655 [5.375–8.150]; p < 0.001). Therefore, large-scale studies are needed given the key role of optimal rSO2 in DCI monitoring following SAH. Fourth, objective parameters, such as blood flow index, can facilitate the assessment of cerebral hemodynamics without prolonged bedside investigations. Keller et al. [36] reported that assessment of regional cerebral blood flow by using NIRS with indocyanine green (ICG) correlated strongly with that of perfusion-weighted magnetic resonance imaging. Terborg et al. [37] also showed that patients with acute MCA occlusion had a significant increase in time to peak and rise time and decreased maximum ICG concentration and blood flow index (maximum delta ICG/rise time) compared with the unaffected hemisphere. Nevertheless, NIRS measurements by using the ICG dye are affected by the pulsatility of systole and diastole and extracerebral path length [36, 38]. Direct comparison with the contralateral side is also inaccurate in patients with poor-grade SAH because of the possibility of bilateral cerebral vasospasm. Because we only enrolled patients with poor-grade SAH in this study, bilateral vasospasm alone was detected and cases of unilateral vasospasm were missed. Accordingly, we could not investigate the nature of DCI. Finally, we used a two-channel NIRS on the forehead in this study. Because the two-channel NIRS reflects regional rSO2 levels of the watershed border zones between the two main MCA and anterior cerebral artery (ACA), NIRS cannot accurately detect vasospasm of the vertebrobasilar artery and the distal M4 segment of the MCA and the A4 segment of the ACA. Lehr and Wickramasinghe [39] demonstrated the conversion of single-channel NIRS into a four-channel NIRS to determine the levels of continuous blood oxygenation in multiple regions of the neonatal brain. NIRS can be used to successfully detect differences in oxygenation and hemodynamic changes of the four regions. Other diagnostic methods using TCD or continuous electroencephalography (cEEG) can overcome the limitations of the two-channel NIRS. Sviri et al. [40] reported that high basilar artery flow velocities exceeding 115 cm/s on TCD were closely associated with delayed ischemia of the posterior circulation. Rosenthal et al. [41] showed that the delayed onset of epileptiform abnormalities in cEEG, which was recorded using the 10–20 scalp electrodes, predicted subsequent DCI in patients with poor-grade SAH. Additionally, cEEG demonstrated higher accuracy in detecting severe vasospasm compared with TCD. Therefore, an efficacy study evaluating the combination of NIRS, TCD, cEEG, or other imaging techniques to evaluate cerebral perfusion is required for early and accurate diagnosis of DCI.
Conclusions
Near-infrared spectroscopy might be a promising tool for real-time detection of DCI in patients with poor-grade SAH at the bedside. Further prospective studies are required to corroborate our findings under various clinical conditions and to set the optimal NIRS protocol for DCI screening in a large cohort of the SAH population.
References
Komotar RJ, Schmidt JM, Starke RM, et al. Resuscitation and critical care of poor-grade subarachnoid hemorrhage. Neurosurgery. 2009;64:397–410.
Hacein-Bey L, Provenzale JM. Current imaging assessment and treatment of intracranial aneurysms. AJR Am J Roentgenol. 2011;196:32–44.
Jeon JS, Sheen SH, Hwang G, Kang SH, Heo DH, Cho YJ. Intravenous magnesium infusion for the prevention of symptomatic cerebral vasospasm after aneurysmal subarachnoid hemorrhage. J Korean Neurosurg Soc. 2012;52:75–9.
Francoeur CL, Mayer SA. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Crit Care. 2016;20:277.
Lee SU, Jeon JP, Lee H, et al. Optic nerve sheath diameter threshold by ocular ultrasonography for detection of increased intracranial pressure in Korean adult patients with brain lesions. Medicine (Baltimore). 2016;95:e5061.
Scheeren TW, Schober P, Schwarte LA. Monitoring tissue oxygenation by near infrared spectroscopy (NIRS): background and current applications. J Clin Monit Comput. 2012;26:279–87.
Khozhenko A, Lamperti M, Terracina S, Bilotta F. Can cerebral near-infrared spectroscopy predict cerebral ischemic events in neurosurgical patients? A narrative review of the literature. J Neurosurg Anesthesiol. 2019;31:378–84.
Rolfe P. In vivo near-infrared spectroscopy. Annu Rev Biomed Eng. 2000;2:715–54.
Maslehaty H, Krause-Titz U, Petridis AK, Barth H, Mehdorn HM. Continuous measurement of cerebral oxygenation with near-infrared spectroscopy after spontaneous subarachnoid hemorrhage. ISRN Neurol. 2012;2012:907187.
Ritzenthaler T, Cho TH, Mechtouff L, et al. Cerebral near-infrared spectroscopy: a potential approach for thrombectomy monitoring. Stroke. 2017;48:3390–2.
Taussky P, O’Neal B, Daugherty WP, et al. Validation of frontal near-infrared spectroscopy as noninvasive bedside monitoring for regional cerebral blood flow in brain-injured patients. Neurosurg Focus. 2012;32:E2.
Kim CH, Jeon JP, Kim SE, Choi HJ, Cho YJ. Endovascular treatment with intravenous thrombolysis versus endovascular treatment alone for acute anterior circulation stroke : a meta-analysis of observational studies. J Korean Neurosurg Soc. 2018;61:467–73.
Cho YD, Kim SE, Lim JW, Choi HJ, Cho YJ, Jeon JP. Protected versus unprotected carotid artery stenting: meta-analysis of the current literature. J Korean Neurosurg Soc. 2018;61:458–66.
Park JJ, Kim BJ, Youn DH, Choi HJ, Jeon JP. A preliminary study of the association between SOX17 gene variants and intracranial aneurysms using exome sequencing. J Korean Neurosurg Soc. 2020;63:559–65.
Kim BJ, Youn DH, Kim Y, Jeon JP. Characterization of the TCR β chain CDR3 repertoire in subarachnoid hemorrhage patients with delayed cerebral ischemia. Int J Mol Sci. 2020;21:3149.
Drayna PC, Abramo TJ, Estrada C. Near-infrared spectroscopy in the critical setting. Pediatr Emerg Care. 2011;27:432–9.
Okazaki T, Kuroda Y. Aneurysmal subarachnoid hemorrhage: intensive care for improving neurological outcome. J Intensive Care. 2018;6:28.
Jeon JS, Sheen SH, Hwang GJ, Kim HC, Kwon BJ. Feasibility of intravenous flat panel detector CT angiography for intracranial arterial stenosis. AJNR Am J Neuroradiol. 2013;34:129–34.
Vora YY, Suarez-Almazor M, Steinke DE, Martin ML, Findlay JM. Role of transcranial Doppler monitoring in the diagnosis of cerebral vasospasm after subarachnoid hemorrhage. Neurosurgery. 1999;44:1237–47.
Samagh N, Bhagat H, Jangra K. Monitoring cerebral vasospasm: How much can we rely on transcranial Doppler. J Anaesthesiol Clin Pharmacol. 2019;35:12–8.
Weir B, Grace M, Hansen J, Rothberg C. Time course of vasospasm in man. J Neurosurg. 1978;48:173–8.
Park JJ, Kim C, Jeon JP. Monitoring of delayed cerebral ischemia in patients with subarachnoid hemorrhage via near-infrared spectroscopy. J Clin Med. 2020;9:1595.
Mijailovic M, Lukic S, Laudanovic D, Folic M, Folic N, Jankovic S. Effects of nimodipine on cerebral vasospasm in patients with aneurysmal subarachnoid hemorrhage treated by endovascular coiling. Adv Clin Exp Med. 2013;22:101–9.
Navi BB, Kamel H, McCulloch CE, et al. Accuracy of neurovascular fellows’ prognostication of outcome after subarachnoid hemorrhage. Stroke. 2012;43:702–7.
Jeon JS, Kim JE, Chung YS, et al. A risk factor analysis of prospective symptomatic haemorrhage in adult patients with cerebral cavernous malformation. J Neurol Neurosurg Psychiatry. 2014;85:1366–70.
Jeon JP, Lee SU, Kim SE, et al. Correlation of optic nerve sheath diameter with directly measured intracranial pressure in Korean adults using bedside ultrasonography. PLoS ONE. 2017;12:e0183170.
Mutoh T, Ishikawa T, Suzuki A, Yasui N. Continuous cardiac output and near-infrared spectroscopy monitoring to assist in management of symptomatic cerebral vasospasm after subarachnoid hemorrhage. Neurocrit Care. 2010;13:331–8.
Zweifel C, Castellani G, Czosnyka M, et al. Continuous assessment of cerebral autoregulation with near-infrared spectroscopy in adults after subarachnoid hemorrhage. Stroke. 2010;41:1963–8.
Lee SU, Hong EP, Kim BJ, Kim SE, Jeon JP. Delayed cerebral ischemia and vasospasm after spontaneous angiogram-negative subarachnoid hemorrhage: an updated meta-analysis. World Neurosurg. 2018;115:e558–69.
Lantigua H, Ortega-Gutierrez S, Schmidt JM, et al. Subarachnoid hemorrhage: who dies, and why? Crit Care. 2015;19:309.
Poon WS, Wong GK, Ng SC. The quantitative time-resolved near infrared spectroscopy (TR-NIRs) for bedside cerebrohemodynamic monitoring after aneurysmal subarachnoid hemorrhage: can we predict delayed neurological deficits? World Neurosurg. 2010;73:465–6.
Le Roux PD, Elliott JP, Newell DW, et al. Predicting outcome in poor-grade patients with subarachnoid hemorrhage: a retrospective review of 159 aggressively managed cases. J Neurosurg. 1996;85:39–49.
Meng L, Settecase F, Xiao J, Yu Z, Flexman AM, Higashida RT. Initial clinical experience with near-infrared spectroscopy in assessing cerebral tissue oxygen saturation in cerebral vasospasm before and after intra-arterial verapamil injection. J Clin Neurosci. 2016;26:63–9.
Carrera E, Schmidt JM, Oddo M, et al. Transcranial Doppler for predicting delayed cerebral ischemia after subarachnoid hemorrhage. Neurosurgery. 2009;65:316–23.
Yokose N, Sakatani K, Murata Y, et al. Bedside assessment of cerebral vasospasms after subarachnoid hemorrhage by near infrared time-resolved spectroscopy. Adv Exp Med Biol. 2010;662:505–11.
Keller E, Nadler A, Alkadhi H, Kollias SS, Yonekawa Y, Niederer P. Noninvasive measurement of regional cerebral blood flow and regional cerebral blood volume by near-infrared spectroscopy and indocyanine green dye dilution. Neuroimage. 2003;20:828–39.
Terborg C, Bramer S, Harscher S, Simon M, Witte OW. Bedside assessment of cerebral perfusion reductions in patients with acute ischaemic stroke by near-infrared spectroscopy and indocyanine green. J Neurol Neurosurg Psychiatry. 2004;75:38–42.
Hopton P, Walsh TS, Lee A. Measurement of cerebral blood volume using near-infrared spectroscopy and indocyanine green elimination. J Appl Physiol. 1985;1999(87):1981–7.
Lehr HP, Wickramasinghe Y. New prototype NIRS instrument [corrected] to investigate multi-regional cerebral blood and tissue oxygenation and haemodynamics. Med Biol Eng Comput. 2000;38:281–6.
Sviri GE, Lewis DH, Correa R, Britz GW, Douville CM, Newell DW. Basilar artery vasospasm and delayed posterior circulation ischemia after aneurysmal subarachnoid hemorrhage. Stroke. 2004;35:1867–72.
Rosenthal ES, Biswal S, Zafar SF, et al. Continuous electroencephalography predicts delayed cerebral ischemia after subarachnoid hemorrhage: a prospective study of diagnostic accuracy. Ann Neurol. 2018;83:958–69.
Funding
This research was supported by the National Research Foundation of Korea and funded by the Ministry of Education (2020R1l1A3070726) and Hallym University Research Fund (HURF-2020-24).
Author information
Authors and Affiliations
Contributions
JPJ designed and obtained funding for the study. JJP and YK collected the data. JJP and JPJ interpreted the data and performed statistical analyses. JPJ and CLC provided input for the final version of the manuscript. All authors reviewed the manuscript and provided editorial feedback.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethical approval/informed consent
This study was approved by the institutional review board of the participating hospital (No. 2016-3, 2017-9, and 2018-6), and informed consent was obtained from the patients or their relatives.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Park, J.J., Kim, Y., Chai, C.L. et al. Application of Near-Infrared Spectroscopy for the Detection of Delayed Cerebral Ischemia in Poor-Grade Subarachnoid Hemorrhage. Neurocrit Care 35, 767–774 (2021). https://doi.org/10.1007/s12028-021-01223-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-021-01223-2