
Abstract
Accounting for 15 % of deaths worldwide, hypertension is often treated with hydrochlorothiazide (HCTZ) (50 million prescriptions annually). HCTZ has a <24-h duration of action, is less potent than chlorthalidone and all major antihypertensive drug classes, and is inferior to four antihypertensive drugs for cardiovascular event (CVE) reduction. If there were alternative diuretics, why prescribe HCTZ? Chlorthalidone is often offered as an alternative to HCTZ, but has limited pharmaceutical formulations. However, there are seven evidence-based, single-tablet, alternative diuretics. For reducing CVE, the following are superior to their comparators: chlorthalidone versus four antihypertensives in multiple hypertensive populations; indapamide versus placebo in elderly Chinese (and versus enalapril for left ventricular hypertrophy), triamterene–HCTZ versus placebo in elderly Europeans, amiloride–HCTZ versus three antihypertensives, and indapamide–perindopril versus placebo in three populations. Additionally, chlorthalidone–azilsartan and spironolactone–HCTZ are potent combinations The aldosterone antagonist component of the latter combination has been shown to reduce total mortality by 30 % in heart failure. Five of these seven have multiple dose formulations. Six cost $4–$77 monthly. In conclusion, based on both scientific and practical grounds, new prescriptions for HCTZ are rarely justified.



Similar content being viewed by others
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Ezzati M, Riboli E. Behavioral and dietary risk factors for noncommunicable diseases. NEJM. 2013;369:954–64.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–20.
Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281–357.
Canadian Hypertension Education Program (CHEP) 2014. http://www.hypertension.ca/en/chep. Accessed 9 July 2014.
National Heart Foundation of Australia. Guide to the management of hypertension: assessing and managing raised blood pressure in adults. 2008, Updated 2010. National Heart Foundation of Australia, 2010.
Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, Kenerson JG, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2014;16(1):14–26.
Epstein M, Calhoun DA. Aldosterone blockers (mineralocorticoid receptor antagonism) and potassium-sparing diuretics. J Clin Hypertens. 2011;13:644–8.
Sica DA. Chapter C130: thiazide and loop diuretics. In: Izzo Jr JL, Sica DA, Black HR, editors. Hypertension primer. 4th ed. Dallas: American Heart Association; 2008.
Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, et al. Health outcomes associated with various antihypertensive therapies used as first line agents: a network meta- analysis. JAMA. 2003;289:2534–44.
Wright JM, Musini VM. First-line drugs for hypertension. Cochrane Database Syst Rev. 2009;3, CD001841.
National Institute for Health and Clinical Excellence. Hypertension: clinical management of primary hypertension in adults. MidCity Place, 71 High Holborn, London WC1V 6NA; 2011, August. Recommends INDAP and CTDN over HCTZ for hypertension.
Ernst ME, Carter BL, Goerdt CJ, et al. Comparative antihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension. 2006;47:352–8. A randomized trial demonstrating lower potency of HCTZ relative to chlorthalidone and a less than 24 hour antihypertensive potency of HCTZ.
Ernst ME, Carter BL, Zheng S, Grimm Jr RH. Meta-analysis of dose–response characteristics of hydrochlorothiazide and chlorthalidone: effects on systolic blood pressure and potassium. Am J Hypertens. 2010;23:440–6.
Peterzan MA, Hardy R, Chaturvedi N, Hughes AD. Meta-analysis of dose–response relationships for hydrochlorothiazide, chlorthalidone, and bendroflumethiazide on blood pressure, serum potassium, and urate. Hypertension. 2012;59(6):1104–9.
Ernst ME, Neaton JD, Grimm Jr RH, Collins G, Thomas W, Soliman EZ, et al. Long-term effects of chlorthalidone versus hydrochlorothiazide on electrocardiographic left ventricular hypertrophy in the multiple risk factor intervention trial. Hypertension. 2011;58(6):1001–7.
Dorsch MP, Gillespie BW, Erickson SR, Bleske BE, Weder AB. Chlorthalidone reduces cardiovascular events compared with hydrochlorothiazide: a retrospective cohort analysis. Hypertension. 2011;57(4):689–94.
Roush GC, Holford TR, Guddati AK. Chlorthalidone compared with hydrochlorothiazide in reducing cardiovascular events: systematic review and network meta-analyses. Hypertension. 2012;59(6):1110–7. Evidence that CTDN lowers cardiovascular events by 21% relative to HCTZ.
Dhalla IA, Gomes T, Yao Z, Nagge J, Persaud N, Hellings C, et al. Chlorthalidone versus hydrochlorothiazide for the treatment of hypertension in older adults: a population-based cohort study. Ann Intern Med. 2013;158(6):447–55.
Jackson EK. Chapter 29, Diuretics. In: Hardman JG, Limbird LE, editors. Goodman & Gilman’s the pharmacologic al basis of therapeutics. New York: McGraw Hill; 2001. pages 757–787 and Table A-II-1.
Chen TM, Chiou WL. Large differences in the biological half-life and volume of distribution of hydrochlorothiazide in normal subjects from eleven studies. Correlation with their last blood sampling times. Int J Clin Pharmacol Ther Toxicol. 1992;30(1):34–7.
Pool PE, Applegate WB, Woehler T, Sandall P, Cady WJ. A randomized, controlled trial comparing diltiazem, hydrochlorothiazide, and their combination in the therapy of essential hypertension. Pharmacotherapy. 1993;13(5):487–93.
Lacourcière Y, Poirier L, Lefebvre J, Archambault F, Cléroux J, Boileau G. Antihypertensive effects of amlodipine and hydrochlorothiazide in elderly patients with ambulatory hypertension. Am J Hypertens. 1995;8(12 Pt 1):1154–9.
Pareek A, Basavanagowdappa H, Zawar S, Kumar A, Chandurkar N. A randomized, comparative study evaluating the efficacy and tolerability of losartan-low dose chlorthalidone (6.25 mg) combination with losartan-hydrochlorothiazide (12.5 mg) combination in Indian patients with mild-to-moderate essential hypertension. Expert Opin Pharmacother. 2009;10(10):1529–36.
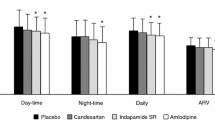
Kwon BJ, Jang SW, Choi KY, Kim DB, Cho EJ, Ihm SH, et al. Comparison of the efficacy between hydrochlorothiazide and chlorthalidone on central aortic pressure when added on to candesartan in treatment-naïve patients of hypertension. Hypertens Res. 2013;36(1):79–84. doi:10.1038/hr.2012.143.
Roush GC, Ernst ME, Kostis JB, Tandon S, Sica DA. Head-to-head comparisons of hydrochlorothiazide with indapamide and chlorthlidone: antihypertensive and metabolic effects. Hypertension 2015; doi:10.1161/HYPERTENSIONAHA.114.05021.
Maxwell MH, Brachfeld J, Itskovitz H, Lunn JA, Moser M, Zawada ET. Blood pressure lowering and potassium conservation by triamterene-hydrochlorothiazide and amiloride-hydrochlorothiazide in hypertension. Clin Pharmacol Ther. 1985;37(1):61–5.
Heran BS, Chen JM, Wang JJ, Wright JM. Blood pressure lowering efficacy of potassium-sparing diuretics (that block the epithelial sodium channel) for primary hypertension. Cochrane Database Syst Rev. 2012;11, CD008167.
Stears AJ, Woods SH, Watts MM, Burton TJ, Graggaber J, Mir FA, et al. A double-blind, placebo-controlled, crossover trial comparing the effects of amiloride and hydrochlorothiazide on glucose tolerance in patients with essential hypertension. Hypertension. 2012;59(5):934–42.
Multicenter Diuretic Cooperative Study Group. Multiclinic comparison of amiloride, hydrochlorothiazide, and hydrochlorothiazide plus amiloride in essential hypertension. Arch Intern Med. 1981;141:482–6.
Maronde RF, Barr J, Vlachakis ND, Spencer CA, Chab L. Oral potassium chloride and amiloride in hydrochlorothiazide-induced potassium loss. Clin Pharmacol Ther. 1984;36:31–5.
Saha C, Eckert GJ, Ambrosius WT, Chun TY, Wagner MA, Zhao Q, et al. Improvement in blood pressure with inhibition of the epithelial sodium channel in blacks with hypertension. Hypertension. 2005;46(3):481–7.
Batterink J, Stabler SN, Tejani AM, Fowkes CT. Spironolactone for hypertension. Cochrane Database Syst Rev. 2010, Issue 8. Art No.: CD008169. doi:10.1002/14651858.
Hilal-Dandan R. Chapter 26. Renin and angiotensin. In: Brunton LL, editor. Goodman & Gillman’s the pharmacological basis of therapeutics. 12th ed. New York: McGraw Hill Medical; 2011. p. 734.
Kang S, Wu YF, An N, Ren M. A systematic review and meta-analysis of the efficacy and safety of a fixed, low-dose perindopril-indapamide combination as first-line treatment of hypertension. Clin Ther. 2004;26(2):257–70.
White WB, Weber MA, Sica D, Bakris GL, Perez A, Cao C, et al. Effects of the angiotensin receptor blocker azilsartan medoxomil versus olmesartan and valsartan on ambulatory and clinic blood pressure in patients with stages 1 and 2 hypertension. Hypertension. 2011;57(3):413–20.
Sica D, White WB, Weber MA, Bakris GL, Perez A, Cao C, et al. Comparison of the novel angiotensin II receptor blocker azilsartan medoxomil vs valsartan by ambulatory blood pressure monitoring. J Clin Hypertens. 2011;13:467–72.
Bakris GL, Sica D, White WB, Cushman WC, Weber MA, Handley A, et al. Antihypertensive efficacy of hydrochlorothiazide vs chlorthalidone combined with azilsartan medoxomil. Am J Med. 2012;125(12):1229.e1–1229.e10.
Eide IK, Torjesen PA, Drolsum A, Babovic A, Lilledahl NP. Low-renin status in therapy-resistant hypertension: a clue to efficient treatment. J Hypertens. 2004;22(11):2217–26.
Hermida RC, Ayala DE, Fernandez JR, Calvo C. Chronotherapy improves blood pressure control and reverts the nondipper pattern in patients with resistant hypertension. Hypertension. 2008;51:69–76.
Ernst ME, Moser M. Use of diuretics in patients with hypertension. NEJM. 2009;361:2153–64.
Hermida RC, Ayala DE, Mojón A, Fernández JR. Influence of circadian time of hypertension treatment on cardiovascular risk: results of the MAPEC study. Chronobiol Int. 2010;27(8):1629–51.
Roush GC, Fapohunda J, Kostis JB. Evening dosing of anti-hypertensives to reduce cardiovascular events: a third type of evidence based on a systematic review and meta-analysis of randomized trials. J Clin Hypertens. 2014;16:561–8.
ABC-H Investigators, Roush G, Fagard R, Pierdomenico S, Reboldi G, Verdecchia P, et al. Prognostic impact from clinic, daytime, and nighttime systolic blood pressure in 9 cohorts of 13,844 patients with hypertension. J Hypertens. 2014;32:2332–40.
Gupta AK, Arshad S, Poulter NR. Compliance, safety, and effectiveness of fixed-dose combinations of antihypertensive agents: a meta-analysis. Hypertension. 2010;55(2):399–407.
Huffman MD, de Cates AN, Ebrahim S. Fixed-dose combination therapy (polypill) for the prevention of cardiovascular disease. JAMA. 2014;312(19):2030–1.
Leren P, Helgeland A. Coronary heart disease and treatment of hypertension. Some Oslo study data. Am J Med. 1986;80(Suppl 2a):3–6.
Wing LM, Reid CM, Ryan P, Beilin LJ, Brown MA, Jennings GL, et al. A comparison of outcomes with angiotensin-converting-enzyme inhibitors and diuretics for hypertension in the elderly. NEJM. 2003;348:583–92.
Jamerson K, Weber MA, Bakris GL, Dahlöf B, Pitt B, Shi V, et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high risk patients. NEJM. 2008;359:2417–28.
SHEP Cooperative Research Group. Prevention of stroke by anti-hypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program. JAMA. 1991;265:3255–64.
ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Diuretic versus alpha blocker as first-step antihypertensive therapy. Final results from the antihypertensive and lipid lowering treatment to prevent heart attack trial (ALLHAT). Hypertension. 2003;42:239–46.
Messerli FH, Makani H, Benjo A, Romero J, Alviar C, Bangalore S. Antihypertensive efficacy of hydrochlorothiazide as evaluated by ambulatory blood pressure monitoring: a meta-analysis of randomized trials. J Am Coll Cardiol. 2011;57:590–600. This paper demonstrates the lesser potency of hydrochlorothiazide relative to other drug classes with ambulatory blood pressure as the outcome.
Ernst ME, Carter BL, Basile JN. All thiazide-like diuretics are not chlorthalidone: putting the ACCOMPLISH study into perspective. J Clin Hypertens (Greenwich). 2009;11(1):5–10.
Kaplan NM. Chlorthalidone versus hydrochlorothiazide: a tale of tortoises and a hare. Hypertension. 2011;58(6):994–5.
Saklayen MG. Which diuretic should be used for the treatment of hypertension? Am Fam Physician. 2008;78(4):444. 446.
Carter BL, Ernst ME, Cohen JD. Hydrochlorothiazide versus chlorthalidone: evidence supporting their interchangeability. Hypertension. 2004;43(1):4–9.
Kurtz TW. Editorial commentary: chlorthalidone: don’t call it “thiazide-like” anymore. Hypertension. 2010;56:335–7.
Woodman R, Brown C, Lockette W. Chlorthalidone decreases platelet aggregation and vascular permeability and promotes angiogenesis. Hypertension. 2010;56:463–70.
ALLHAT officers and coordinators. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs. diuretic. JAMA. 2002;288:2981–97.
Malacco E, Mancia G, Rappelli A, Menotti A, Zuccaro MS, Coppini A, et al. Treatment of isolated systolic hypertension: the SHELL study results. Blood Press. 2003;12:160–7.
PATS Collaborating Group. Post-stroke antihypertensive treatment study. A preliminary result. Chin Med J (Engl). 1995;108(9):710–7.
MRC Working Party. Medical Research Council trial of treatment of hypertension in older adults: principal results. BMJ. 1992;304(6824):405–12.
Brown MJ, Palmer CR, Castaigne A, de Leeuw PW, Mancia G, Rosenthal T, et al. Morbidity and mortality in patients randomised to double-blind treatment with a long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment (INSIGHT). Lancet. 2000;356(9227):366–72.
Amery A, Birkenhäger W, Brixko P, Bulpitt C, Clement D, Deruyttere M, et al. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly trial. Lancet. 1985;1(8442):1349–54.
PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;358(9287):1033–41.
ADVANCE Collaborative Group. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007;370:829–40.
Beckett NS, Peters R, Fletcher AE, Staessen JA, Liu L, Dumitrascu D, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358(18):1887–98.
Taler SJ. Should chlorthalidone be the diuretic of choice for antihypertensive therapy? Curr Hypertens Rep. 2008;10(4):293–7. Review.
Bataillard A, Schiavi P, Sassard J. Pharmacological properties of indapamide. Clin Pharmacokinet. 1999;37 suppl 1:7–12.
Campbell DB, Brackman F. Cardiovascular protective properties of indapamide. Am J Cardiol. 1990;65:11H–27.
Aubert I, Djian F, Rouffy J. Beneficial effects of indapamide on lipoproteins and apoproteins in ambulatory hypertensive patients. Am J Cardiol. 1990;65:77H–80.
Vergely C, Walker MK, Zeller M, Rademakers JR, Maupoil V, Schiavi P, et al. Antioxidant properties of indapamide, 5-OH indapamide and hydrochlorothiazide evaluated by oxygen-radical absorbing capacity and electron paramagnetic resonance. Mol Cell Biochem. 1998;178(1–2):151–5.
Rendu F, Bachelot C, Molle D, Caen J, Guez D. Indapamide inhibits human platelet aggregation in vitro: comparison with hydrochlorothiazide. J Cardiovasc Pharmacol. 1993;22 Suppl 6:S57–63.
Senior R, Imbs JL, Bory M, Amabile G, Denis B, Zannad F, et al. Indapamide reduces hypertensive left ventricular hypertrophy: an international multicenter study. J Cardiovasc Pharmacol. 1993;22 Suppl 6:S106–10.
Carey PA, Sheridan DJ, de Cordoue A, Guez D. Effect of indapamide on left ventricular hypertrophy in hypertension: a meta-analysis. Am J Cardiol. 1996;77(6):17b–9.
Gosse P, Sheridan DJ, Zannad F, Dubourg O, Guéret P, Karpov Y, et al. Regression of left ventricular hypertrophy in hypertensive patients treated with indapamide SR 1.5 mg versus enalapril 20 mg: the LIVE study. J Hypertens. 2000;18(10):1465–75.
Donnelly R, Molyneaux LM, Willey KA, Yue DK. Comparative effects of indapamide and captopril on blood pressure and albumin excretion rate in diabetic microalbuminuria. Am J Cardiol. 1996;77(6):26B–30.
Marre M, Puig JG, Kokot F, Fernandez M, Jermendy G, Opie L, et al. Equivalence of indapamide SR and enalapril on microalbuminuria reduction in hypertensive patients with type 2 diabetes: the NESTOR Study. J Hypertens. 2004;22(8):1613–22.
Molyneaux LM, Willey KA, Yue DK. Indapamide is as effective as captopril in the control of microalbuminuria in diabetes. J Cardiovasc Pharmacol. 1996;27(3):424–7.
Oates JA, Brown NJ. Chapter 3. Antihypertensive agents and the drug therapy of hypertensioin. In: Hardman JG, Limbird LE, editors. Goodman & Gilman’s The pharmacological basis of therapeutics. 10th edn. 2001. p. 874.
Siscovick DS, Raghunathan TE, Psaty BM, Koepsell TD, Wicklund KG, Lin X, et al. Diuretic therapy for hypertension and the risk of primary cardiac arrest. N Engl J Med. 1994;330(26):1852–7.
Widman L, Dyckner T, Wester P-O. Effects of triamterene on serum and skeletal muscle electrolytes in diuretic-treated patients. Eur J Clin Pharmacol. 1988;33:577–9.
Schohn DC, Jahn HA, Pelletier BC. Dose-related cardiovascular effects of spironolactone. Am J Cardiol. 1993;71:40A–5.
Virdis A, Neves MF, Amiri F, Viel E, Touyz RM, Schiffrin EL. Spironolactone improves angiotensin- induced vascular changes and oxidative stress. Hypertension. 2002;40(4):504–10.
Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation. 2008;117(25):e510–26.
Engbaek M, Hjerrild M, Hallas J, Jacobsen IA. The effect of low-dose spironolactone on resistant hypertension. J Am Soc Hypertens. 2010;4(6):290–4.
Chapman N, Dobson J, Wilson S, Dahlöf B, Sever PS, Wedel H, et al. Effect of spironolactone on blood pressure in subjects with resistant hypertension. Hypertension. 2007;49(4):839–45.
Nishizaka MK, Zaman MA, Calhoun DA. Efficacy of low-dose spironolactone in subjects with resistant hypertension. Am J Hypertens. 2003;16(11 Pt 1):925–30.
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709–17.
Jeunemaitre X, Chatellier G, Kreft-Jais C, Charru A, DeVries C, Plouin PF, et al. Efficacy and tolerance of spironolactone in essential hypertension. Am J Cardiol. 1987;60(10):820–5.
Dahlöf B, Gosse P, Guéret P, Dubourg O, de Simone G, Schmieder R, et al. Perindopril/indapamide combination more effective than enalapril in reducing blood pressure and left ventricular mass: the PICXEL study. J Hypertens. 2005;23(11):2063–70.
Mallion JM, Chamontin B, Asmar R, De Leeuw PW, O’Brien E, Duprez D, et al. Twenty-four-hour ambulatory blood pressure monitoring efficacy of perindopril/indapamide first-line combination in hypertensive patients: the REASON study. Am J Hypertens. 2004;17(3):245–51.
de Luca N, Mallion JM, O’Rourke MF, O’Brien E, Rahn KH, Trimarco B, et al. Regression of left ventricular mass in hypertensive patients treated with perindopril/indapamide as a first-line combination: the REASON echocardiography study. Am J Hypertens. 2004;17(8):660–7.
Mogensen CE, Viberti G, Halimi S, Ritz E, Ruilope L, Jermendy G, et al. Effect of low-dose perindopril/indapamide on albuminuria in diabetes: preterax in albuminuria regression: PREMIER. Hypertension. 2003;41(5):1063–71.
IMS Institute for Healthcare Informatics. Medicine use and shifting costs of healthcare: a review of the use of medicines in the United States in 2013. 11 Waterview Boulevard, Parsippany, NJ 07054, USA. Appendix 3.
Kuehlein T, Lauz G, Gutscher A, Goetz K, Szecseny J. Diuretics for hypertension: an inconsistency in primary care prescribing behaviour. Curr Med Res Opin. 2011;27:497–502.
Robinson DM, Wellington K. Indapamide sustained release. A review of its use in the treatment of hypertension. Drugs. 2006;66:257–71.
Compliance with Ethics Guidelines
Conflict of Interest
George C. Roush, Michael E. Ernst, John B. Kostis, Ramandeep Kaur, and Domenic A. Sica declare that they have no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Guidelines/Clinical Trials/Meta-Analysis
Key Points
*Hydrochlorothiazide (HCTZ) has <24-h duration of action, has less antihypertensive potency than chlorthalidone and all first line drug classes, and is inferior to chlorthalidone, hydrochlorothiazide–amiloride, amlodipine, and enalapril in reducing cardiovascular events.
*Chlorthalidone has been offered in response but has limited pharmaceutical formulations.
*There are seven single-tablet, evidence-based diuretic alternatives to HCTZ and a variety of multiple dose formulations.
*Continuing to prescribe HCTZ is rarely justified.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Figure S1
(PDF 872 kb)
Rights and permissions
About this article

Cite this article
Roush, G.C., Ernst, M.E., Kostis, J.B. et al. Not Just Chlorthalidone: Evidence-Based, Single Tablet, Diuretic Alternatives to Hydrochlorothiazide for Hypertension. Curr Hypertens Rep 17, 31 (2015). https://doi.org/10.1007/s11906-015-0540-6
Published:
DOI: https://doi.org/10.1007/s11906-015-0540-6